Introduction
Bony inner ear malformations are fairly rare anomalies, representing approximately 20 per cent of congenital sensorineural hearing loss (SNHL) cases. The remaining 80 per cent of cases are membranous malformations in which the bony architecture of the inner ear is normal and the pathology is at the cellular level.Reference Sennaroglu and Saatci1 Congenital inner ear anomalies are important indicators for cochlear implantation, and an exact diagnosis is crucial for clinicians to plan the therapy.Reference Young, Ryan and Young2 Anomalies of the bony labyrinth can be diagnosed using high-resolution computed tomography (CT) of the temporal bone because it provides excellent delineation of the intricate bony inner ear anatomy. Magnetic resonance imaging (MRI) is increasingly used in conjunction with high-resolution CT in the pre-operative investigation for cochlear implantation to assess the status of the cochleovestibular nerve and the membranous labyrinth.Reference Young, Ryan and Young2
The cochlear nerve canal, also known as the cochlear aperture or cochlear fossette, is the bony transition point between the internal auditory canal and the cochlear modiolus.Reference Wilkins, Prabhu, Huang, Ogando and Kenna3 It transmits the cochlear nerve to the modiolus and into the cochlea. Studies have found that cochlear nerve canal stenosis can indicate hypoplasia or aplasia of the cochlear nerve.Reference Adunka, Jewells and Buchman4,Reference Miyasaka, Nosaka, Morimoto, Taiji and Masaki5 Previous studies have shown that severe hearing loss is correlated with cochlear nerve canal stenosis plus additional inner ear structural abnormalities.Reference Wilkins, Prabhu, Huang, Ogando and Kenna3
The semicircular canal is a structure within the inner ear that comprises three semicircular canals orientated perpendicular to each other and connected to the vestibule. The prevalence of different semicircular canal anomalies varies according to the overall severity of the anomaly; for example, a mild anomaly of the lateral semicircular canal is the most common malformation of the bony labyrinth whereas complete semicircular canal aplasia is very rare.Reference Satar, Mukherji and Telian6
Recent studies aiming to assess the correlation between semicircular canal morphology and SNHL have shown conflicting results and therefore the correlation still remains controversial.Reference Satar, Mukherji and Telian6–Reference Tahir, Bajin, Atay, Mocan and Sennaroǧlu8 To our knowledge, an association between semicircular canal abnormalities and cochlear nerve canal stenosis has not been widely studied. Therefore, this study aimed to examine the prevalence of cochlear nerve canal stenosis in our study population and the associated semicircular canal abnormalities and additional inner ear anomalies, particularly of the cochlea, among our paediatric SNHL cohort.
Materials and methods
Case selection
This study was approved by our institutional medical research committee (approval number: FF-2017-357). The study was conducted in a tertiary care centre that is one of the largest centres for cochlear implantation in Malaysia. Access to the patient database was obtained from the cochlear implant registry from the Department of Otorhinolaryngology at our hospital. All patients had severe-to-profound hearing loss that was either bilateral or unilateral and required cochlear implantation because hearing aids had failed to correct the problem.
We retrospectively reviewed the CT images of 265 consecutive patients who underwent high-resolution CT scans of the temporal bone (as part of the pre-operative investigation prior to cochlear implantation) at the hospital between January 2008 and December 2017 (10 years' duration).
Patients who had been listed more than once in the registry (mostly due to revision of implants for various reasons), were over 20 years old or had CT images that were suboptimal for interpretation (i.e. images with slice thickness more than 1.0 mm or images degraded by artefacts) were excluded. Patients who had complete labyrinthine aplasia and cochlear aplasia were also excluded because we were unable to measure the cochlear nerve canal. Therefore, there were 132 patients excluded from the study, leaving 265 ears (1 ear showed cochlear aplasia, which prevents evaluation of the cochlear nerve canal, and was therefore excluded) from 133 patients who met the inclusion criteria of the study.
CT scanning techniques and reformats
Non-contrast high-resolution CT was performed as part of the workup of cochlear implantation. The majority of patients required oral sedation or intravenous sedation if oral sedation failed. The paediatric patients who had undergone an MRI scan to view the internal acoustic canal right before the CT scan would have received a single general anaesthetic that covered both scans. Scanning was performed with a 64-channel multidetector CT scanner (Somatom Sensation 64; Siemens Medical Solutions, Erlangen, Germany). Axial scans were acquired in a plane parallel to the orbitomeatal plane in the helical mode with section thickness of 0.6 mm and reconstructed in an axial plane at 0.6 mm using a bone algorithm at 0.6 mm intervals. Some of the earlier images were scanned with a section thickness of 1.0 mm, reconstructed at 1.0 mm with 1.0 mm intervals. Reformatted images were made in the axial plane in all cases (parallel to the lateral semicircular canal) with a slice thickness of 0.60 mm (or 1.0 mm for earlier images aforementioned). Images were viewed using the standard bone window with a window width of 3000 Hounsfield units and window centre of 350 Hounsfield units using a medical picture archiving and communication system (‘PACS’) Osirix® workstation.
Image evaluation
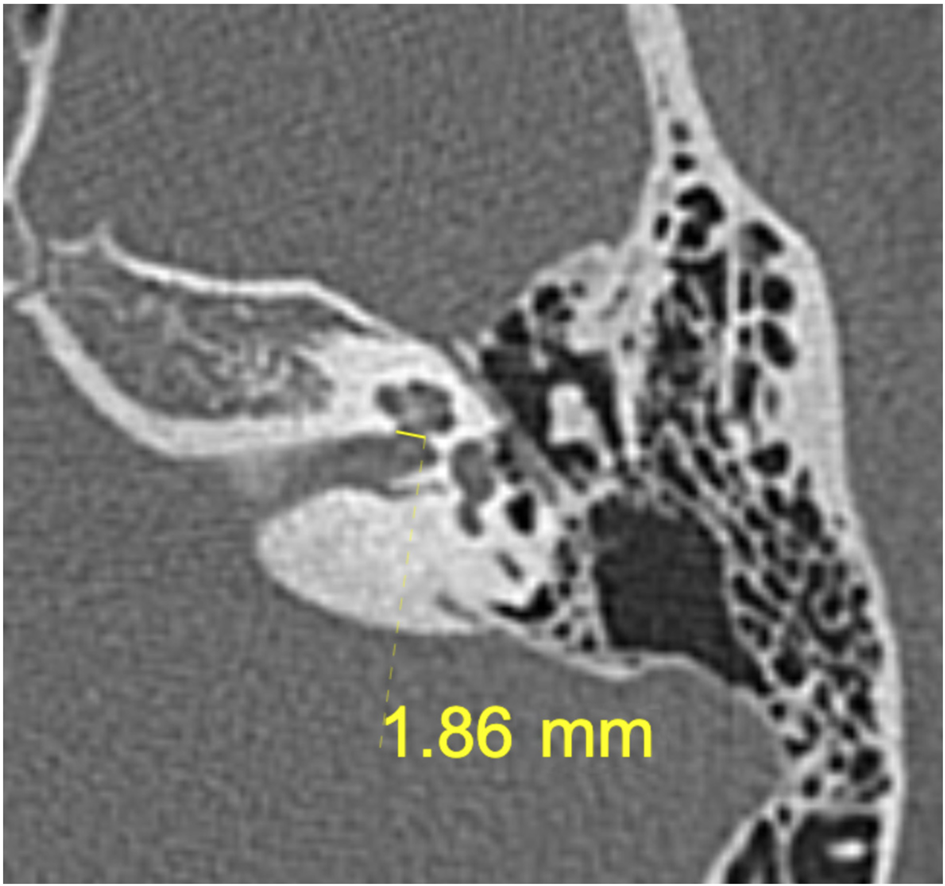
Each ear was evaluated separately. The diameter of the cochlear nerve canal was measured using calipers on the axial images for each ear along the inner margin of the bony wall from the mid-portion through the base of the modiolus. The measurement was recorded in millimetres (Figure 1). Two independent measurements were performed for each cochlear nerve canal by two radiology registrars with the mean of the two readings taken as the final measurement of the cochlear nerve canal. The morphology of the inner ear structures, particularly the cochlea and the semicircular canal, was evaluated by a radiologist with a subspecialty in paediatric neuroradiology.
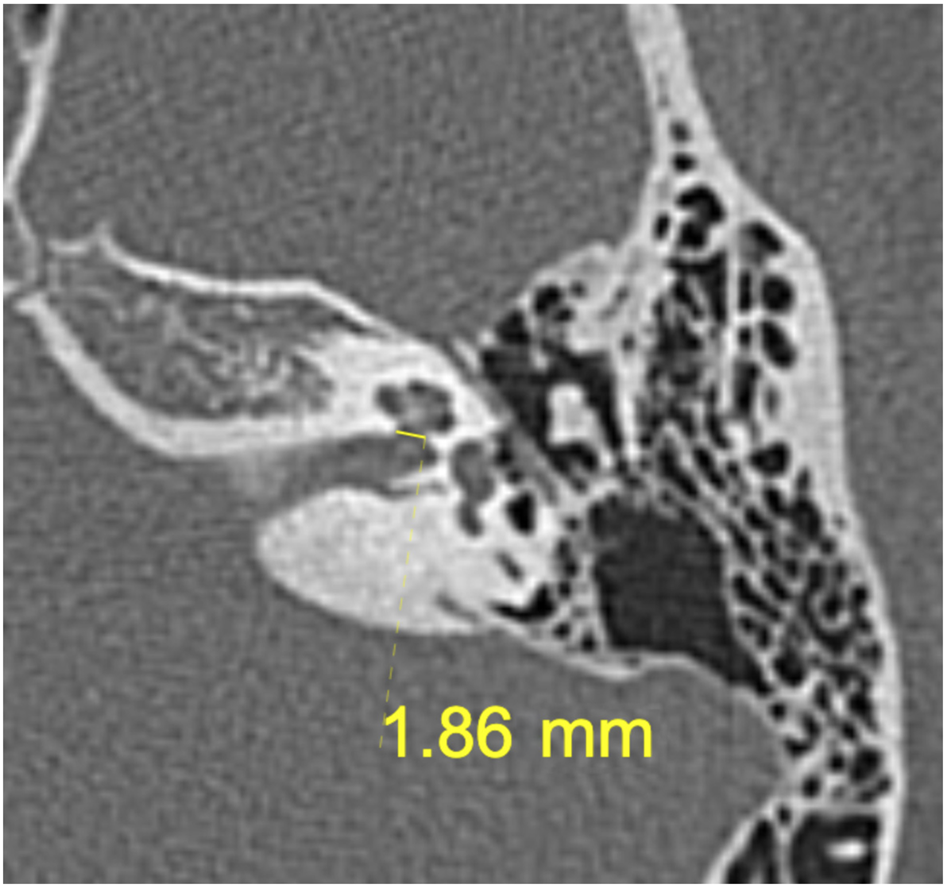
Fig. 1. Axial computed tomography image showing the cochlear nerve canal measurement (straight line).
A cochlear nerve canal with axial measurements of 1.5 mm or less was considered stenotic. This cut-off value of 1.5 mm for the diameter of cochlear nerve canal was based on earlier studies.Reference Miyasaka, Nosaka, Morimoto, Taiji and Masaki5,Reference Tahir, Bajin, Atay, Mocan and Sennaroǧlu8,Reference Stjernholm and Muren9 In cases where the cochlear nerve canal appeared to be completely stenosed and no measurements were possible, this was recorded as an atretic cochlear nerve canal and quantified as 0 mm.
When evaluating the abnormal semicircular canal, we categorised it as aplastic, hypoplastic or dilated. Aplasia of the semicircular canal was noted when the canal was completely absent and an isolated vestibule was present. The semicircular canal was categorised as hypoplastic if one or more of the canals were not completely formed. Cochlear anomalies were classified based on the cochleovestibular malformations classification system developed by Sennaroglu and Saatci where anomalies were classed as common cavity deformity, cochlear hypoplasia, incomplete partition type I or incomplete partition type II.Reference Sennaroglu and Saatci1
Statistical analysis
Statistical analysis was performed using IBM SPSS® (version 21) statistical software. A single measure intraclass correlation using a two-way mixed analysis of variance model was used to estimate the inter-rater reliability of the measurements of the cochlear nerve canal. Pearson correlation coefficients were calculated to determine whether there was significant correlation between the cochlear nerve canal diameter and semicircular canal and other inner ear structure morphology. In all statistical analyses, the significance level was p < 0.05.
Results
Demographics
The mean age of the group was 4 years old (range, 1 to 17 years). Out of the 265 ears included in this study, 54.3 per cent were from male patients and 45.7 per cent were from female patients with a male to female ratio of 1.2:1. The ratio was reversed for the stenotic cochlear nerve canal group with a male to female ratio of 1:1.7. The majority of the patients were Chinese (51 per cent), followed by Malay (43 per cent), Indian (4.5 per cent) and others (1.5 per cent), as shown in Table 1.
Table 1. Age, gender and race distributions among patients with normal and stenotic cochlear nerve canals

*n = 200; †n = 65
Cochlear nerve canal and inner ear anomalies
The intraclass correlation with 95 per cent cochlear implantation of the cochlear nerve canal measurements of the right and left ear were 0.82 (0.76, 0.87) and 0.8 (0.72, 0.86), respectively, both of which indicated good reliability. Therefore, cumulative values were used for the final cochlear nerve canal diameter.
Of the 265 ears (133 patients), the cochlear nerve canal was stenotic in 65 ears (24 per cent). Three ears had a measurement of 0 mm indicating an atretic cochlear nerve canal. The mean and median cochlear nerve canal measurement for the 65 ears were 0.96 mm and 1.26 mm, respectively (range, 0–1.49 mm).
Of the 65 ears with a stenotic cochlear nerve canal, 17 ears (26 per cent) had an abnormal semicircular canal (Figure 2). The Pearson chi-square analysis showed significant correlation between cochlear nerve canal stenosis and semicircular canal abnormalities (p = 0.00). The most common semicircular canal abnormality accompanying a stenotic cochlear nerve canal was lateral semicircular canal dilatation (n = 5). Out of the 65 ears with a stenotic cochlear nerve canal, 17 ears (26 per cent) had cochlear abnormalities (Figure 3). The correlation was not as strong as p = 0.05. Seven ears with cochlear nerve canal stenosis had both semicircular canal and cochlear anomalies although Pearson analysis showed no significant correlation (p = 0.06) (Figure 4). Table 2 shows the prevalence of abnormalities and correlations between cochlear nerve canal stenosis and semicircular canal and cochlear anomalies.

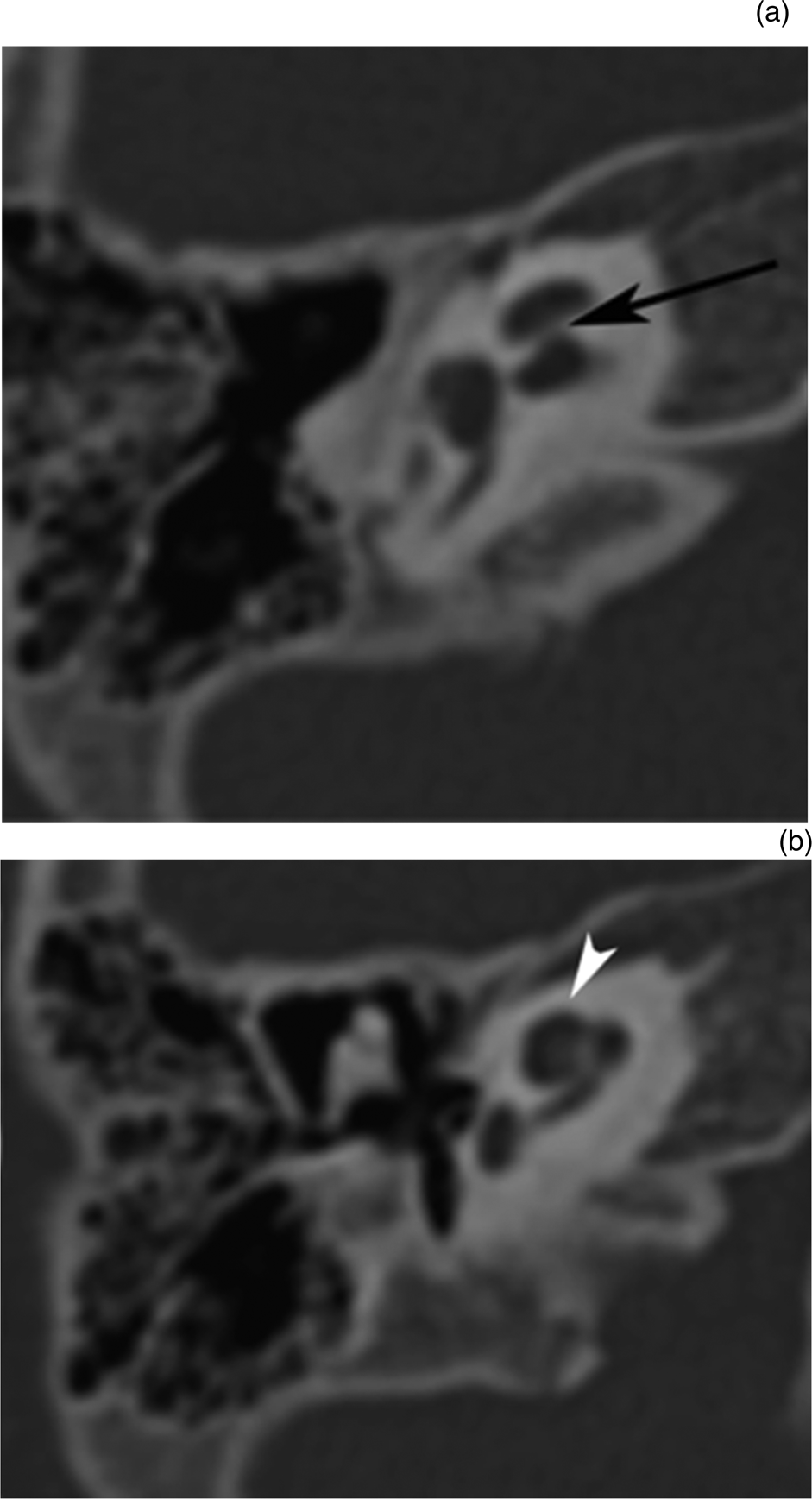
Fig. 2. Axial computed tomography scans from the same patient as in Figure 1, showing: (a) cochlear nerve canal stenosis (black arrow) and (b) lateral semicircular canal aplasia (white arrowhead). In this case, the vestibule is dilated (asterisk).

Fig. 3. Axial computed tomography scans from the same patient as in Figure 1, showing: (a) cochlear nerve canal stenosis (black arrow) and (b) cystic cochlear apex in incomplete partition type II (white arrowhead).

Fig. 4. Axial computed tomography images showing: (a) cochlear nerve canal stenosis (black arrow), (b) lateral semicircular canal dilatation (black arrowhead) and (c) incomplete partition type II (white arrowhead) occurring in the same patient. The vestibule is also dilated (white asterisk).
Table 2. Correlations between CNC stenosis and abnormal SCC, abnormal cochlea and abnormal SCC and cochlea

*n = 200; †n = 65; ‡significant value, p < 0.05; **chi-square test. CNC = cochlear nerve canal; SCC = semicircular canal
Overall, 29 ears (45 per cent) in the stenotic group had accompanying anomalies. The most common anomaly was incomplete partition type II (n = 15 ears; 23 per cent), followed by lateral semicircular canal dilatation (n = 5 ears; 7.6 per cent) and bilateral semicircular canal aplasia (n = 4 ears; 6 per cent). There were 36 ears (55 per cent) with a stenotic cochlear nerve canal that occurred without accompanying semicircular canal or cochlear anomalies.
Semicircular canal and cochlear morphology
Overall, 35 of 265 ears (13 per cent) had congenital semicircular canal abnormalities: 10 had lateral semicircular canal dilatation, 8 had lateral semicircular canal aplasia, 7 had lateral semicircular canal hypoplasia (Figure 5), 4 had complete semicircular canal aplasia, and 1 had posterior semicircular canal hypoplasia. The remaining five ears had labyrinthine ossificans (n = 5). Complete absence of the bilateral semicircular canal was seen in two patients. One patient had features consistent with ‘CHARGE’ (coloboma, heart defect, atresia choanae, growth retardation, genital abnormalities and ear abnormalities) syndrome (Figure 6), and another had no documented syndrome but had co-existing congenital anomalies of the ventricular septal defect, patent ductus arteriosus and polydactyly. Both patients also had concurrent cochlear anomalies of incomplete partition type II. There were 9 ears (3 per cent) that had semicircular canal abnormalities alone without cochlear nerve canal stenosis or cochlear anomalies. The most frequent isolated semicircular canal abnormality was lateral semicircular canal aplasia.

Fig. 5. (a–c) Consecutive axial computed tomography sections showing lateral semicircular canal hypoplasia (black arrows). No other inner ear abnormalities were detected in this patient.

Fig. 6. Axial computed tomography scan showing bilateral aplasia of the semicircular canal with abnormal vestibule configuration (black arrows) in a patient with ‘CHARGE’ syndrome (i.e. coloboma, heart defect, atresia choanae, growth retardation, genital abnormalities and ear abnormalities). In this case, the internal auditory canals are slightly dilated (white asterisk).
Out of 265 ears, 48 (18 per cent) had cochlear anomalies: 37 were incomplete partition type II, 7 were incomplete partition type I and 1 was cochlear hypoplasia. The remaining 5 had labyrinthine ossificans.
Discussion
The cochlear nerve canal is also called the cochlear aperture, bony cochlear nerve canal and cochlear fossette. There is also some variation across the literature in what is considered a normal versus narrow diameter of the cochlear nerve canal. Despite the variation, the literature consistently reports that patients with SNHL are more likely to have narrower cochlear nerve canals than patients with normal hearing, and a significantly narrowed cochlear nerve canal is often associated with cochlear nerve hypoplasia or aplasia.Reference Adunka, Jewells and Buchman4,Reference Miyasaka, Nosaka, Morimoto, Taiji and Masaki5,Reference Kono10 Wilkins et al. also found that there is a statistically significant relationship between the degree of hearing loss and the degree of stenosis. In addition, more severe hearing loss is also correlated with cochlear nerve canal stenosis plus additional inner ear anomalies, and these structural abnormalities may occur more often than previously appreciated.Reference Wilkins, Prabhu, Huang, Ogando and Kenna3
The most common malformation of the semicircular canal bony labyrinth is a lateral semicircular canal anomaly, which was also seen in our study.Reference Satar, Mukherji and Telian6,Reference Breheret, Brecheteau, Tanguy and Laccourreye11 As reported in previous literature, complete semicircular canal aplasia is very rare, and we only depicted it in 4 out of 265 ears (1.5 per cent) in our study.Reference Satar, Mukherji and Telian6 Complete semicircular canal aplasia has been universally associated with ‘CHARGE’ syndromeReference Morimoto, Wiggins, Hudgins, Hedlund, Hamilton and Mukherji12 as demonstrated in one of our patients and has been reported to occur in Goldenhar syndrome,Reference Wineland, Menezes, Shimony, Shinawi, Hullar and Hirose13 Noonan syndromeReference Satar, Mukherji and Telian6 and persistent petrosquamosal sinus,Reference Goetz14 but few case studies have reported it to occur in isolation, without an associated syndrome or other inner ear anomaly. Breheret et al. reported one such case of isolated bilateral complete semicircular canal aplasia in a non-syndromic adult patient presenting with unilateral hearing loss.Reference Breheret, Brecheteau, Tanguy and Laccourreye11
This study found that there was significant correlation between cochlear nerve canal stenosis and semicircular canal abnormalities (p = 0.00), and that the most frequent semicircular canal abnormality associated with cochlear nerve canal stenosis was lateral semicircular canal dilatation. The correlation between cochlear nerve canal stenosis and cochlear anomalies was less statistically significant. Previous literature provides conflicting results with regard to this.Reference Yi, Lim, Kang, Park, Park and Lee15–Reference Yu, Mukherji, Carrasco, Pillsbury and Shores17 Yi et al.Reference Yi, Lim, Kang, Park, Park and Lee15 found that the most common associated inner ear anomaly in cochlear nerve canal stenosis was internal auditory canal stenosis whereas Wilkins et al.Reference Wilkins, Prabhu, Huang, Ogando and Kenna3 reported cochlear anomalies, in particular hypoplasia of the modiolus and cochlear turn abnormalities, as the most common associated anomalies. In this study, although we found that the same percentage of patients (26 per cent) had semicircular canal or cochlear anomalies in the setting of cochlear nerve canal stenosis, the non-significant correlation may be because more cases of cochlear anomalies were seen without cochlear nerve canal stenosis (31 ears versus 17 ears with cochlear nerve canal stenosis). Similarly, when semicircular canal abnormalities and cochlear anomalies occur together, there was no significant correlation between cochlear nerve canal stenosis and these conditions (p = 0.06).
Most of the patients with semicircular canal anomalies and cochlear nerve canal stenosis presented with SNHL without any other otology symptoms such as imbalance or otalgia. Previous studies also showed similar clinical findings, and genetic and molecular testing has been advocated in the literature because semicircular canal anomalies are currently known to be associated with certain genetic abnormalities such as ‘CHARGE’ and Goldenhar syndrome, among others.Reference Breheret, Brecheteau, Tanguy and Laccourreye11–Reference Wineland, Menezes, Shimony, Shinawi, Hullar and Hirose13,Reference Yu, Mukherji, Carrasco, Pillsbury and Shores17 Therefore, besides aiming to treat SNHL, physicians should screen patients for any relevant genetic and molecular testing to ensure holistic management of the patients.
Though there is a strong correlation between cochlear nerve canal stenosis and semicircular canal abnormalities, the most common anomaly found accompanying the cochlear nerve canal stenosis was incomplete partition type II, which was also the most common cochlear anomaly with or without other inner ear malformations found in this study population. This finding is concordant with previous literature, which stated that incomplete partition type II is the most common cochlear malformation and accounts for more than 50 per cent of all cochlear deformities.Reference Joshi, Navlekar, Kishore, Reddy and Kumar16 Thus, it is important to identify this anomaly while reporting high-resolution CT temporal bone in cochlear implantation candidates due to its common occurrence. Our study does not include the post-cochlear implantation outcomes. Nevertheless, previous studies have demonstrated good surgical and functional outcomes in patients with incomplete partition type II.Reference Sefein, Younes, Omara, Hamada, Sami and EL Rouby18 However, post-operative performance is reported to be poor in total semicircular canal aplasia, isolated incomplete partition, cochlear hypoplasia and the common cavity, all of which predominantly affect development rather than being related to labyrinthine anatomy alone.Reference Buchman, Copeland, Yu, Brown, Carrasco and Pillsbury19
Another interesting finding in our study was that there were nine ears with semicircular canal abnormalities without cochlear nerve canal stenosis or cochlear anomalies. The most common type of semicircular canal anomaly was lateral semicircular canal aplasia. Embryologically, the otic vesicle splits into the pars superior (dorsal part) and pars inferior (ventral part) at the sixth week of foetal development.Reference Breheret, Brecheteau, Tanguy and Laccourreye11 The pars superior becomes the utricle and then the semicircular canal by week eight of foetal development and is phylogenetically older than the pars inferior. The pars inferior forms the vestibular saccules and cochlear canal and is fully formed by week nine of foetal development.Reference Satar, Mukherji and Telian6,Reference Breheret, Brecheteau, Tanguy and Laccourreye11 Based on the inner ear malformations classification established by Sennaroglu and Saatci,Reference Sennaroglu and Saatci1 deformities result from sudden arrest of development during these successive stages, which is why the lateral canal is the most frequently involved as it is the last to form among the three semicircular canals. Given the sequence of the inner ear embryogenesis, canal aplasia with a normal cochleovestibular system seems chronologically impossible, as the membranous vestibular labyrinth forms before the definitive formation of the cochlea.Reference Satar, Mukherji and Telian6,Reference Breheret, Brecheteau, Tanguy and Laccourreye11 It is postulated that there may be a more selective, probably genetic disorder of semicircular canal development or ossification in the pars superior that may be responsible for this finding and that cochlear and vestibular development may rely on independent mechanisms without interaction.Reference Satar, Mukherji and Telian6,Reference Breheret, Brecheteau, Tanguy and Laccourreye11
• Patients with sensorineural hearing loss (SNHL) are more likely to have narrowed cochlear nerve canals and there is a significant relationship between degree of hearing loss and degree of stenosis
• More severe hearing loss is correlated with cochlear nerve canal stenosis and additional inner ear anomalies
• Correlation between semicircular canal morphology and SNHL remains controversial as studies have shown conflicting results
• Cochlear nerve canal stenosis is significantly associated with semicircular canal abnormalities
• Lateral semicircular canal abnormalities are the most frequent semicircular canal abnormalities found in association with cochlear nerve canal stenosis and in isolation
• Selective, probably genetic disorders, rather than arrested development of the inner ear, may be responsible for isolated semicircular canal abnormalities in patients with severe to profound SNHL
Hearing loss that is associated with semicircular canal dysplasia without cochlear anomalies is most likely due to anomalous membranous labyrinth development, which is not radiologically detectable.Reference Yu, Mukherji, Carrasco, Pillsbury and Shores17 In addition, Sennaroglu and SaatciReference Sennaroglu and Saatci1 found that semicircular canal aplasia was never detected in the absence of other malformations, and Yu et al.Reference Yu, Mukherji, Carrasco, Pillsbury and Shores17 reported that isolated semicircular canal abnormalities always occurred in a context of congenital malformation.
One limitation of the present study is that the patient database and clinical information was obtained retrospectively without a predetermined definition about the information desired. Therefore, some relevant information may not have been recorded and thus we could not rule out the possible association of all the nine ears with isolated semicircular canal abnormalities with any clinical syndrome(s) that may not be evaluated clinically at the time of the study.
Conclusion
Cochlear nerve canal stenosis is associated with semicircular canal abnormalities in which the correlation is statistically significant, and the most frequently associated semicircular canal abnormality is lateral semicircular canal dysplasia. The most frequent accompanying anomaly for cochlear nerve canal stenosis is incomplete partition type II. Presence of these anomalies should be scrutinised when there is a stenotic cochlear nerve canal upon reviewing high-resolution CT temporal bone performed for patients with profound SNHL.
Acknowledgements
The authors would like to thank Ms Nadiah Saat for her excellence assistance in statistical analysis.
Competing interests
None declared