


Introduction
Chondrosarcoma of the larynx accounts for 2 per cent of all laryngeal neoplasms.Reference Burkey, Hoffman and Baker1 True incidences are unknown and difficult to assess, as low grade chondrosarcomas are frequently misinterpreted as chondromas.
Here, we present two cases of laryngeal chondrosarcoma which were managed conservatively by endoscopic debulking and regular follow up.
Case reports
Case one
An 80-year-old woman presented with a one-year history of hoarseness of voice, swelling in the neck and dysphagia (more for solids than liquids), and a three-month history of breathlessness on exertion.
On examination, the patient had evident stridor.
Nasal endoscopy revealed a smooth mass distorting the larynx and obscuring both vocal folds. A computed tomography (CT) scan of the neck revealed a semicystic mass in the supraglottic region, extending from the upper limit of the thyroid cartilage to the left vocal fold, with no neck lymphadenopathy (Figure 1).
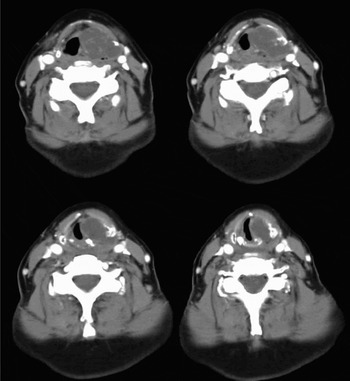
Fig. 1 Axial computed tomography scans showing a 3.5 × 3 cm, semicystic mass in the supraglottic region, extending from the upper limit of the thyroid cartilage to the left vocal fold, and involving the latter. The right vocal fold is clear.
On admission, the patient was administered steroids, and microlaryngoscopy was arranged for the following day. This revealed a smooth mass distorting the larynx and extending to the left true vocal fold, while the rest of the larynx was unremarkable. Multiple biopsies were taken which revealed features consistent with low grade chondrosarcoma (Figure 2).

Fig. 2 Fragments of chondroid tissue with mild hypercellularity, myxoid changes, occasional binucleate cells and possible areas of necrosis, but no mitosis (H&E; ×20).
A decision to proceed with endoscopic debulking was made, keeping in mind the patient's associated co-morbid conditions (angina, hypothyroidism and hypertension) and the low grade nature of the tumour. Under general anaesthesia, microlaryngoscopy was performed, which revealed a massive, supraglottic mass involving the left aryepiglottic fold, false vocal fold and pyriform fossa. A 3 × 2 × 2 cm mass was debulked by piecemeal removal and macroscopic clearance was achieved.
The patient was followed up regularly, and at the time of writing had been asymptomatic for three years.
Case two
A 69-year-old man presented with a one-year history of hoarse voice, dysphagia, choking sensation and cough.
Examination revealed pooling of saliva and an ulcerated mass in the right pyriform fossa, together with a right vocal fold palsy (in the paramedian position), but no cervical lymphadenopathy.
A barium swallow suggested a mass in the hypopharynx. A CT scan of the larynx showed a soft tissue mass in the right pyriform fossa extending anteriorly into the pre-epiglottic space. Microlaryngoscopy revealed a mass in the right pyriform fossa, with fixation of the right true vocal fold. Histological analysis revealed features consistent with a low grade chondrosarcoma.
A decision to perform endoscopic debulking was taken, for the same reasons as mentioned for the previous case.
This patient was followed up regularly for about 13 years, and at the time of writing was completely asymptomatic.
Discussion
Cartilaginous tumour of the larynx was first described by Heusinger in 1822. The incidence of laryngeal chondrosarcoma has been under-reported, as differentiation between chondroma and chondrosarcoma has been a topic of debate. Chondrosarcoma of the larynx accounts for 2 per cent of all laryngeal tumours, while chondrosarcoma of the head and neck region constitute about 10 per cent of all chondrosarcoma tumours in the body.
The age of presentation varies between the fifth to seventh decades, the average age being 66 years. The tumour is seven times more common in Caucasians, and three times more common in men compared with women.
The aetiology is unknown, but initial, disordered ossification of the laryngeal cartilage has been speculated to be responsible. Areas of ossification in hyaline cartilages show a predilection for the development of laryngeal chondrosarcomas.Reference Thompson and Gannon2
Laryngeal chondrosarcomas usually arise from the posterior lamina of the cricoid cartilage (78 per cent) or the thyroid cartilage (18 per cent), and rarely from the arytenoids and epiglottis.Reference Rinaldo, Howard and Ferlito3
Signs and symptoms depend on the location of the tumour. Lesions arising from the cricoid cartilage usually present with dyspnoea, hoarseness and dysphagia. Some authors believe that idiopathic vocal fold paralysis is an exclusive sign of cricoid chondrosarcoma and may be related to the involvement of recurrent laryngeal nerve or crico-arytenoid joint fixation. Thyroid cartilage chondrosarcomas may present as an asymptomatic neck mass.Reference Shirley4
In the larynx, chondrosarcomas typically present with slow growth, rare metastasis and low recurrence rates. Chondrosarcoma causes local destruction due to a mass effect before it invades surrounding tissues.
Radiologically, this tumour can present as a lesion of variable density, showing either endolaryngeal spread (growing inwards, confined by the outer margin of the cartilage of origin) or extralaryngeal spread (growth extending beyond the confines of the larynx into the surrounding soft tissue). On CT scanning, chondrosarcomas demonstrate fine, punctuate, stippled to coarse (‘popcorn’) calcification within the tumour.Reference Wang, Borges, Lufkin, Se Carz and Wang5
• Laryngeal chondrosarcomas are rare, cartilaginous neoplasms, accounting for 2 per cent of all laryngeal neoplasms
• The slow growth of these neoplasms can present difficulties both in diagnosis and treatment
• The definitive treatment of laryngeal chondrosarcomas is controversial. As in all laryngeal neoplasms, preservation of laryngeal function with surgical eradication of the neoplasm is the preferred option
• However, a conservative approach to management of these tumours should be considered, particularly in patients with associated co-morbid conditions
The diagnosis of chondrosarcoma is based on criteria devised by Lichtenstein and Joffe for malignant cartilaginous tumours of bony origin, published in 1943.Reference Lichtenstein and Joffe6 These criteria include the presence of: many cells with plump nuclei; more than an occasional cell with two such nuclei; and giant cartilage cells with single or multiple nuclei or with chromatin clumps.
Depending on the degree of differentiation, chondrosarcomas are classified as low, medium or high grade tumours. Most of the reported chondrosarcomas of the larynx are of a low grade, although some high grade tumours have been described,Reference Huizenga and Balogh7 as have several cases of dedifferentiated chondrosarcomas.Reference Jones8
The definitive treatment of laryngeal chondrosarcoma has been a topic of debate. Preservation of laryngeal function with surgical eradication of the neoplasm is the preferred option.Reference Finn, Geopfert and Batsakis9–Reference Lavertu and Tucker11 However, according to Thome et al., total resection of cricoid cartilage with thyrotracheal anastomosis over a stent is an alternative technique to total laryngectomy in patients with chondrosarcoma.
Conclusion
Laryngeal chondrosarcomas are rare tumours commonly occurring in men in their seventh decade. The cricoid cartilage is commonly involved. Surgery is the principal treatment modality. However, a conservative approach to management of these tumours should be borne in mind, especially in patients with associated co-morbid conditions.


