


Introduction
Asymmetrical sensorineural hearing loss (SNHL) and unilateral tinnitus can signal the presence of an acoustic neuroma or other pathology within the cerebellopontine angle. A magnetic resonance imaging (MRI) scan of the internal auditory meatus (IAM) is the diagnostic ‘gold standard’. The criteria outlining which patients should undergo MRI are well documented, although there remains debate about which screening protocol is the most sensitive.Reference Rajeev, Babur, Karakitsou and Mehta1
Within the UK, it is common practice for screening to be carried out in tertiary care by an otolaryngologist. Based on patient symptoms and/or a pre-determined set of screening criteria, an MRI is requested, and either a further out-patient clinic appointment is made to discuss the results, or the patient is contacted by telephone or post. The incidence and prevalence of any pathology being found on a screening scan can vary depending on which international screening criterion protocol is used, but quoted figures in the literature give a worldwide prevalence of 0.02–4.3 per cent and an incidence of approximately 20 million per year.Reference Rajeev, Babur, Karakitsou and Mehta1–Reference Pan, Huang, Morioka, Hathout and El-Saden7
All patients presenting with asymmetrical SNHL or unilateral tinnitus undergo a pure tone audiogram carried out by an audiologist. These key members of the multidisciplinary team are ideally placed to screen patients as a first point of contact and to order an MRI of the IAM as required. Any patients with pathology can then be seen by the otolaryngologist for further assessment. Wong and Capper have previously shown audiology-led screening of patients to be a safe practice.Reference Wong and Capper4
This study presents our practice of an audiology-led screening programme for acoustic neuroma over a four-year period. We show that such a programme is not only safe, but can result in significant departmental cost savings.
Materials and methods
Setting
The study was conducted in a 700-bedded tertiary referral centre serving a catchment population of approximately 338 800.
Methodology
Patients are referred directly to the audiology department from the general practitioner with suspected SNHL and/or tinnitus. Patients are assessed by the audiologist (which includes audiology technicians and audiological scientists) and those meeting the departmental criteria are referred for an MRI scan (non-enhanced, T2-weighted axial images for speed and cost savings). The departmental MRI scan criteria have been pre-defined and agreed across the otolaryngology, audiology and radiology departments, and are based upon nationally recognised criteria (Table 1).
Table 1. Protocol used for audiologist-led screening of patients with asymmetrical SNHL and/or tinnitus at our institution

SNHL = sensorineural hearing loss
For patients with asymmetrical SNHL, an MRI is ordered if the audiogram shows a difference in the left and right thresholds of 15 dB or greater at two or more neighbouring frequencies. Where an existing audiogram taken in the last 24 months is available, asymmetry is defined as a deterioration of 15 dB or greater in air conduction threshold readings at two or more of the following frequencies: 0.5, 1, 2 or 4 kHz. An MRI is also ordered for any patient with unilateral tinnitus or with symptoms suggestive of Ménière's disease. Exclusion criteria include patients unfit for scanning or those aged 75 years or older (who are discussed with the ENT department before proceeding).
Scan results are routinely checked by a senior otolaryngologist. If the reported findings are negative for acoustic neuroma or other pathology, a letter is sent to the patient. If pathology is found, the patient is seen in the ENT clinic to discuss further management (see Figure 1 for referral flow chart). Having a senior otolaryngologist check the scan findings minimises the risk of missing intracranial pathology in patients screened by non-medically trained practitioners. The otolaryngologist can then also decide whether patients need medical input at that point, on a case-by-case basis.

Fig. 1. Flowchart showing patient care pathway of audiologist-led acoustic neuroma screening. GP = general practitioner; MRI = magnetic resonance imaging
Ethical approval
Ethical approval was granted by the Southend University Hospital NHS Foundation Trust Hospital Local Ethics Committee.
Results
Between April 2013 and March 2017, a total of 1126 MRI scans were performed based on the screening criteria for acoustic neuroma. This resulted in 27 out of 1126 scans (2.4 per cent) that were positive for an abnormality in the cerebellopontine angle, 25 out of 1126 (2.22 per cent) of which are reported as acoustic neuroma. The acoustic neuromas ranged from 3 mm to 20 mm in diameter, were predominately right-sided (17 out of 27; 63 per cent), and mostly associated with asymmetrical SNHL (25 out of 27; 92.6 per cent). The other two lesions were meningiomas (2 out of 1126; 0.18 per cent) (Figure 2).
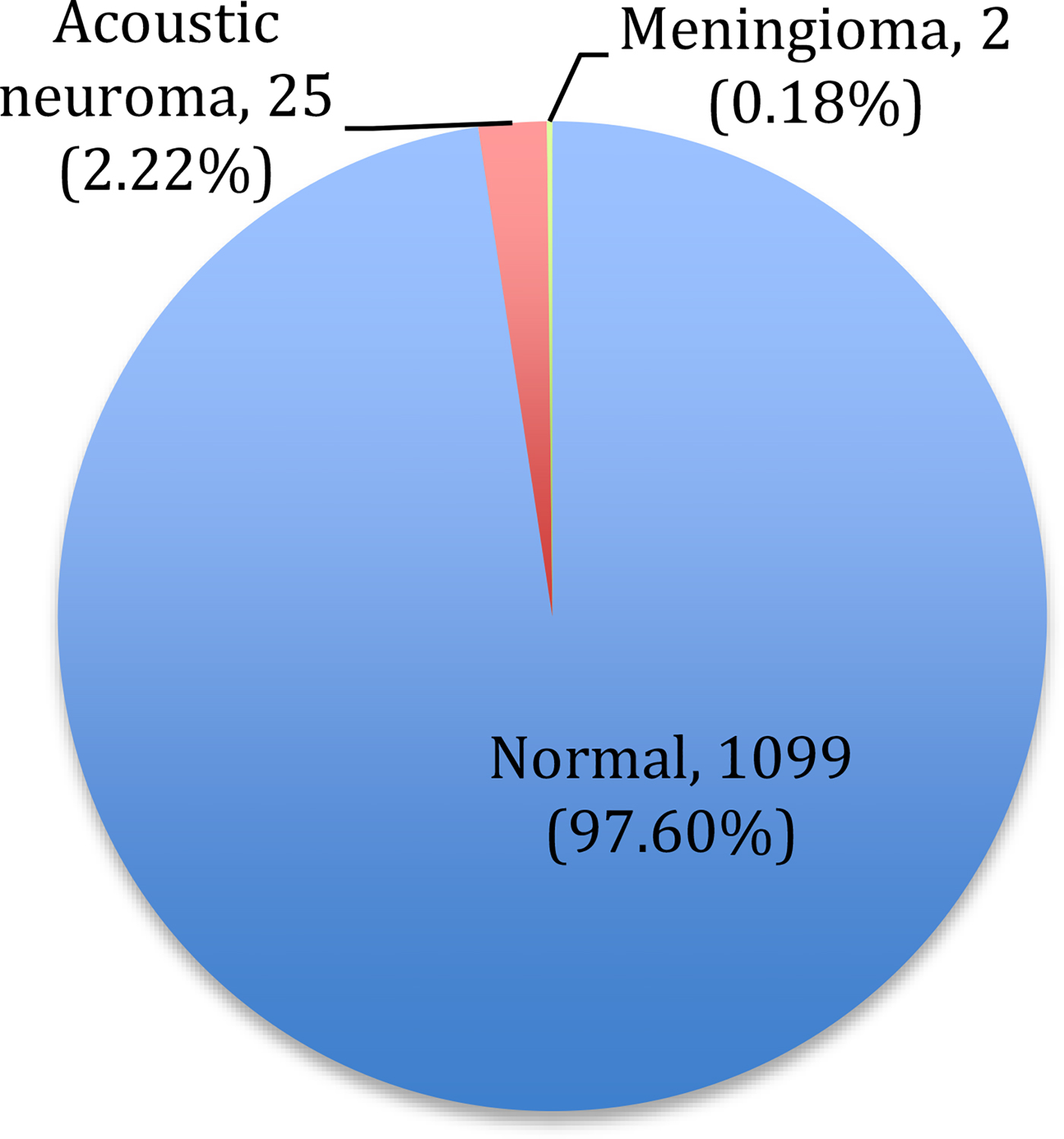
Fig. 2. Distribution of pathology found in patients screened for acoustic neuroma using magnetic resonance imaging of the internal auditory meatus.
During this period, 1099 patients (97.6 per cent) were primarily seen and discharged by the audiologist, and 27 (2.4 per cent) were referred to the otolaryngologist for further management. An audiologist appointment lasts 45 minutes, and involves a pure tone audiogram, history taking and management planning. At our hospital, this appointment results in a cost saving of £150, as the patient does not require a further consultation with an otolaryngologist. An overall saving of £164 850 (1099 × £150) was thus made over four years through the introduction of this screening programme.
Discussion
Synopsis of new findings
Based on our data, an audiology-led screening programme for acoustic neuroma provides a better use of resources. This results in similar clinical outcomes to those if screening was performed by the otolaryngologist, and cost benefits to the department.
Comparison with other studies
Cerebellopontine angle pathology as a cause of asymmetrical SNHL and/or unilateral tinnitus is rare, with acoustic neuroma being the most common cause.Reference Pan, Huang, Morioka, Hathout and El-Saden7 For those few patients found to have an acoustic neuroma, the prognosis is generally good. In a 10-year longitudinal cohort study of patients with intracanalicular acoustic neuromas, Kirchmann et al. found that tumour growth had occurred in 37 per cent and growth into the cerebellopontine angle had occurred in 23 per cent of patients, with conservative treatment failing in only 15 per cent.Reference Kirchmann, Karnov, Hansen, Dethloff, Stangerup and Caye-Thomasen8
There is ongoing debate regarding who should be screened with MRI. The reported sensitivity of audiological criteria outlined in internationally published protocols ranges between 82 and 97 per cent, and specificity is between 15 and 61 per cent.Reference Nouraei, Huys, Chatrath, Powles and Harcourt9 In one study, Obholzer et al. showed that by applying the best of seven protocols to their patient cohort, they were able to theoretically reduce the number of scans they performed in a one-year period from 392 to 168.Reference Obholzer, Rea and Harcourt3 Our protocol is based on a departmental literature review, and analysis of recent guidelines and protocols used for the screening of acoustic neuroma.Reference Obholzer, Rea and Harcourt3, 10–Reference Sheppard, Milford and Anslow12 The introduction of this protocol has yielded an acoustic neuroma prevalence of 2.22 per cent, which is in keeping with that quoted in other studies.
The financial burden of screening patients for cerebellopontine angle pathology in otolaryngological practice is substantial.Reference Daniels, Shelton and Harnsberger13 Magnetic resonance imaging has long superseded auditory brainstem response as the primary test used to screen for acoustic neuromas, given its increasing sensitivity and ever-reducing cost.Reference Fortnum, O'Neill, Taylor, Lenthall, Nikolopoulos and Lightfoot14 The need for gadolinium contrast imaging has also been found to be largely unnecessary in screening, given that non-contrast studies are equally as effective as those with contrast, further bringing costs down.Reference Daniels, Shelton and Harnsberger13, Reference Fortnum, O'Neill, Taylor, Lenthall, Nikolopoulos and Lightfoot14 Conversely, Pan et al. discuss the disparity in cost between the screening of patients for acoustic neuroma and those patients with positive findings who benefitted from intervention.Reference Pan, Huang, Morioka, Hathout and El-Saden7 They found that the estimated screening cost per patient for those who benefitted from surgery or radiation was US$ 147 030, while US federal compensation for unilateral hearing loss was US$ 44 888.Reference Pan, Huang, Morioka, Hathout and El-Saden7
• This study investigated an audiologist-led screening programme for acoustic neuroma in patients with asymmetrical sensorineural hearing loss and/or unilateral tinnitus
• The programme is safe and suitable for any otolaryngology department
• The prevalence of cerebellopontine angle pathology found on magnetic resonance imaging was similar to that published in the literature
• Such a programme can lead to significant departmental cost savings, and results in a more streamlined patient care pathway
• A pre-determined, standardised and accepted screening protocol is required, based on international guidelines
Wong and Capper have demonstrated in their prospective case series of 396 scans that an audiologist-led screening programme for acoustic neuroma is a viable and safe option.Reference Wong and Capper4 Our data, based on a much larger number of scans and over a longer timeframe, support their findings and provide figures on the potential financial saving that can be achieved.
Study strengths and weaknesses
To our knowledge, our study is only one of two that directly investigates the clinical and cost benefits of an audiologist-led screening programme for acoustic neuroma, and represents the largest cohort of its type. The study was performed prospectively, thus greatly reducing confounding errors and potential sources of bias, as opposed to if data were analysed retrospectively.
Recommendations for clinical practice
The local audiology department can act as a point of direct referral for patients with asymmetrical SNHL and/or unilateral tinnitus. It can provide sole patient care through MRI screening for acoustic neuromas and further management for those patients without pathology, negating the need for otolaryngological input. A pre-determined, standardised and accepted screening protocol based on international guidelines aids in this process. Having a senior otolaryngologist involved in the reviewing of scan results, who is available for queries from audiological staff, in addition to regular interdepartmental audit, helps to minimise clinical error and risk.
Conclusion
This study suggests that an audiology-led screening programme for acoustic neuroma using pre-determined criteria does not compromise patient care, and can lead to significant cost savings for the hospital and a more streamlined patient care pathway.
Competing interests
None declared



