



Introduction
The ratio of length between the second (index) and fourth (ring) fingers (2D:4D) is hypothesized to reflect individual differences in exposure to foetal androgens and oestrogens,Reference Manning, Scutt, Wilson and Lewis-Jones1, Reference Wilson2 and may act as a marker of the developmental origins of pathology.Reference Manning3–Reference Manning and Bundred5 2D:4D is sexually dimorphic, with males typically exhibiting lower ratios than females.Reference Hönekopp and Watson6 Low ratios are frequently reported to be associated with ‘male-typed traits’ (i.e., traits in which males typically exceed females in terms of score, propensity, or risk), whereas high ratios are frequently associated with ‘female-typed traits’ (i.e., traits in which females typically exceed males in terms of score, propensity or risk).Reference Manning3, Reference Manning4, Reference Austin, Manning, McInroy and Mathews7, Reference Voracek8 Considering the implications of being able to examine effects of the prenatal hormonal environment retrospectively, it is important to better establish the validity of proposed biomarkers such as digit ratio.
Some animal studies have shown that 2D:4D can be altered in predictable ways by manipulating foetal exposure to sex hormones under experimental conditions.Reference Saino, Rubolini, Romano and Boncoraglio9–Reference Zheng and Cohn11 However, research of this nature is impossible in humans for ethical reasons, so evidence for a link between these variables in humans comes from indirect observation. Notably, some studiesReference Brown, Hines, Fane and Breedlove12–Reference Rivas, Moreira and Santo15 have reported that females with congenital adrenal hyperplasia exhibit relatively low 2D:4D ratios, although one studyReference Buck, Williams, Hughes and Acerini16 did not observe this. Conversely, relatively high digit ratios have been reported in people with complete androgen insensitivity syndromeReference Berenbaum, Korman Bryk, Nowak, Quigley and Moffat17, Reference van Hemmen, Cohen-Kettenis, Steensma, Veltman and Bakker18 and Kleinfelter’s syndrome.Reference Manning, Kilduff and Trivers19 Autism spectrum conditions (in which elevated foetal androgens may be implicatedReference Baron-Cohen, Auyeung and Nørgaard-Pedersen20, Reference Baron-Cohen, Lutchmaya and Knickmeyer21) have been associated with low 2D:4D ratios,Reference Hönekopp22–Reference Voracek26 although it should be noted that a recent large studyReference Schieve, Tian and Dowling27 found evidence of high 2D:4D in female children with autism.
Few studies have reported on correlations between 2D:4D and foetal sex hormone levels in humans. The literature broadly suggests a negative correlation (i.e., low, masculinized digit ratios being associated with high foetal testosterone exposure), but many null findings have been reported alongside statistically significant effects.Reference Richards28 Although research has generally focussed on digit ratios for the right hand (R2D:4D) and/or left hand (L2D:4D), mean 2D:4D (i.e., the average of R2D:4D and L2D:4D) (M2D:4D) is commonly reported. Three studiesReference Hickey, Doherty and Hart29–Reference Mitsui, Araki and Goudarzi31 have examined M2D:4D in relation to androgens measured from umbilical cord blood assayed immediately after delivery. Hickey et al.Reference Hickey, Doherty and Hart29 reported no significant correlations, Mitsui et al.Reference Mitsui, Araki and Goudarzi30 observed a negative correlation between M2D:4D and insulin-like factor 3 (INSL3) in males, and Mitsui et al.Reference Mitsui, Araki and Goudarzi31 observed a negative correlation between M2D:4D and dehydroepiandrosterone (DHEA) in males (but not in females). It should however be noted that the two studies by Mitsui et al.Reference Mitsui, Araki and Goudarzi30, Reference Mitsui, Araki and Goudarzi31 reported on the same cohort, and that the statistically significant effects observed were accompanied by other null findings. Asymmetry in digit ratio (D[R–L]) (i.e., R2D:4D minus L2D:4D) is also commonly examined, with relatively low R2D:4D compared to L2D:4D being hypothesized to indicate high androgen exposure.Reference Manning3, Reference Manning, Kilduff, Cook, Crewther and Fink32 Only two studies of sex hormones measured from umbilical cord bloodReference Hickey, Doherty and Hart29, Reference Hollier, Keelan and Jamnadass33 have examined associations with D[R–L], and neither observed significant effects.
Testosterone measured from umbilical cord blood has been shown to predict later phenotypic outcomes,Reference Cohen-Bendahan, van de Beek and Berenbaum34, Reference Hollier, Keelan, Hickey, Maybery and Whitehouse35 and, although acknowledging that sex hormone levels around the time of birth are influenced by a range of obstetric and perinatal variables that should be considered when examining relationships between umbilical cord hormones and biological outcomes, a recent review by Hollier et al.Reference Hollier, Keelan, Hickey, Maybery and Whitehouse35 (p. 6) concluded that ‘cord blood is useful in providing direct measurement of late gestational androgen and estrogen concentrations’. However, testosterone measured from amniotic fluid may provide a better indication of the foetal hormonal environment during the second trimester, the time at which androgen concentrations are maximally sexually differentiated.Reference Cohen-Bendahan, van de Beek and Berenbaum34, Reference Hines36, Reference van de Beek, Thijssen, Cohen-Kettenis, van Goozen and Buitelaar37 Amniotic fluid is assayed during amniocentesis, an invasive procedure in which fluid is extracted from the amniotic sac surrounding the developing foetus. HinesReference Hines36 (p. 174) noted that ‘umbilical cord blood is not as good a measure of the early hormonal environment as is amniotic fluid because it contains a larger maternal contribution. Levels of hormones in umbilical cord blood samples, including levels of androgens, also can be influenced by the stress of labor and childbirth, further reducing their reliability as a measure of the fetal hormone environment’.
Only two studies have reported on associations between digit ratio and foetal hormones measured from amniotic fluid. Lutchmaya et al.Reference Lutchmaya, Baron-Cohen, Raggatt, Knickmeyer and Manning38 observed a significant negative correlation between the ratio of testosterone to oestradiol in amniotic fluid and R2D:4D in 2-year-old infants. However, no effect was observed for L2D:4D, and neither testosterone nor oestradiol was a significant predictor on its own. Ventura et al.Reference Ventura, Gomes, Pita, Neto and Taylor39 reported a significant negative correlation between amniotic testosterone and L2D:4D in newborn females, though a similar effect for R2D:4D was not statistically significant; there were no correlations between amniotic testosterone and right or left 2D:4D in newborn males. Neither Lutchmaya et al.Reference Lutchmaya, Baron-Cohen, Raggatt, Knickmeyer and Manning38 nor Ventura et al.Reference Ventura, Gomes, Pita, Neto and Taylor39 examined amniotic sex hormone concentrations in relation to M2D:4D or D[R–L].
Another possible method for examining foetal exposure to androgens and oestrogens is to measure maternal circulating hormones during pregnancy.Reference Cohen-Bendahan, van de Beek and Berenbaum34, Reference Manning and Fink40 Hickey et al.Reference Hickey, Doherty and Hart29 correlated maternal androstenedione (A4), dehydroepiandrosterone sulfate (DHEAS), sex hormone binding globulin (SHBG), total testosterone (TT), free testosterone (cFT) and free androgen index (FAI) measured at 18 and 34 weeks’ gestation with offspring digit ratio variables measured at 14–16 years of age. Other than weak positive correlations with A4 at 18 weeks, no effects were observed. However, Ventura et al.Reference Ventura, Gomes, Pita, Neto and Taylor39 reported a significant negative correlation between maternal plasma testosterone and offspring R2D:4D when male and female samples were combined (but not when they were analysed separately). Barona et al.Reference Barona, Kothari, Skuse and Micali41 observed a negative correlation with L2D:4D, though did not report separate analyses for males and females. The only study to examine M2D:4D and D[R-L] was Hickey et al.Reference Hickey, Doherty and Hart29; no significant effects emerged for either of these variables, although a trend was observed for M2D:4D to correlate positively with A4 at 18 weeks (r = 0.179, P = 0.052).
M2D:4D and D[R–L] are commonly reported on in the digit ratio literature, yet we do not currently know how either relate to testosterone measured from amniotic fluid, and only one study has examined them in relation to testosterone measured from maternal circulation during pregnancy. Due to ethical and practical considerations, opportunities to examine 2D:4D in relation to amniotic testosterone have been very limitedReference Baron-Cohen, Lutchmaya and Knickmeyer21, Reference Richards28). We therefore performed a secondary analysis of the dataset reported on by Ventura et al.,Reference Ventura, Gomes, Pita, Neto and Taylor39 to determine whether amniotic testosterone and/or maternal circulating testosterone (both assayed during the second trimester) correlate with M2D:4D and D[R–L] in newborn infants.
Method
The study was approved by the Hospital Centre of Central Lisbon EPE (Dona Estefânia Hospital Ethics Committee), and written informed consent was acquired for all procedures. A detailed description of the study methodology has already been published,Reference Ventura, Gomes, Pita, Neto and Taylor39 and so only a brief recap is provided here.
Participants
One hundred and eighty-seven pregnant mothers referred to Dona Estefânia Hospital, Lisbon, for karyotyping between December 2009 and June 2011 were recruited at the time of amniocentesis to take part in a previous study,Reference Ventura, Gomes and Carreira42 though six were later excluded due to foetal or maternal pathology. 106 mothers and 106 infants (54 females, 52 males) are included in the current analysis (those for whom infant digit ratios were recorded). Maternal plasma testosterone was assayed in all 106 mothers, though one participant was identified as being an extreme outlier (plasma testosterone = 6.19 nmol/L). This participant (and therefore her child) was removed from analyses of correlation between maternal plasma testosterone and offspring digit ratio (note that these participants were retained in the other analyses presented here). Amniotic testosterone was measured for 101 infants. The median age of mothers was 37.90 years [interquartile range (IQR = 3.60)], and infant digit ratio measurements were recorded approximately 1 day after birth (median = 27.18 h, IQR = 31.00).
Design and procedure
Blood samples were collected from mothers at arrival, and were immediately centrifuged. During amniocentesis, an aliquot of up to 3–4 ml of amniotic fluid that was surplus to clinical requirement was obtained. Both amniotic fluid and blood samples were stored at −80°C until assay. Total plasma testosterone was measured in duplicate aliquots at the Department of Chemistry and Biochemistry, Faculty of Sciences, University of Lisbon, by standard radio-immunoassay (RIA) using Spectria testosterone RIA® coated tubes (Orion Diagnostica, Finland). The intra- and inter-assay coefficients of variation for plasma testosterone were 4.5% and 5.1%, respectively. Testosterone in amniotic fluid was measured at King’s College London using a development of the method described by Kulle et al.Reference Kulle, Riepe, Melchior, Hiort and Holterhus43 Oasis HLB 1cc (30 μg) extraction cartridges were used for solid phase extraction of samples with isopropanol. The reconstituted samples were analysed by ultra-pressure liquid chromatography followed by mass spectrometry.
Two raters used Vernier callipers (measuring to 0.01 mm) to measure the infants’ right and left index and ring finger lengths from photocopies of the palmar surface of their hands. Ventura et al.Reference Ventura, Gomes, Pita, Neto and Taylor39 reported high reliability across raters, and so averaged the two sets of measurements to create the R2D:4D and L2D:4D values used in their analyses. We used these latter variables to calculate M2D:4D as (R2D:4D+L2D:4D)/2, and D[R–L] as R2D:4D−L2D:4D.
Statistical analysis
Statistical analyses were performed using IBM SPSS version 24. As 2D:4D is sexually dimorphic,Reference Hönekopp and Watson6 independent-samples t-tests were used to examine sex differences in newborn M2D:4D and D[R-L]. In addition, we used paired-samples t-tests to examine differences between digit ratios for the right and left hands in males and females. Pearson’s correlations were performed to explore relationships between amniotic and maternal plasma testosterone and newborn M2D:4D and D[R–L], and Fisher’s r-to-z transformation was used to determine whether the slopes observed for males differed significantly from those observed for females.
Results
Although this sample has already been described by Ventura et al.,Reference Ventura, Gomes, Pita, Neto and Taylor39 an overview of the key variables is included here to facilitate interpretation of the results. Digit ratios were lower in newborn males than in newborn females: for L2D:4D (male, n = 52, M = 0.927, SD = 0.039; female, n = 54, M = 0.950, SD = 0.042) this difference was statistically significant, t(104) = −2.950, P = 0.004; for R2D:4D the effect was not significant (male, n = 52, M = 0.945, SD = 0.043; female, n = 54, M = 0.954, SD = 0.042), t(104) = −1.031, P = 0.305). Testosterone in amniotic fluid was significantly higher in males (n = 49, M = 0.865 nmol/L, SD = 0.402) than in females (n = 51, M = 0.335 nmol/L, SD = 0.333), t(98) = 7.189, P < 0.001, though testosterone in maternal plasma did not differ when the developing foetus was male (n = 52, M = 1.584, SD = 0.667) as opposed to female (n = 53, M = 1.813, SD = 0.901), t(95.856) = −1.484, P = 0.141 (equal variances not assumed). Testosterone in maternal plasma and amniotic fluid were not correlated for offspring of either sex: males, r(47) = −0.085, P = 0.561; females, r(48) = 0.166, P = 0.250 (please note that these correlations differ from those reported by Ventura et al.Reference Ventura, Gomes, Pita, Neto and Taylor39: the reason is that the correlations reported in the initial paper relate to all the infants [n = 167] for whom amniotic and maternal circulating testosterone had been measured, and not just for those that had also been examined for 2D:4D).
The mean score for M2D:4D was lower in males (n = 52, M = 0.936, SD = 0.031) than in females (n = 54, M = 0.952, SD = 0.037), t(104) = −2.390, P = 0.019, but there was no difference for D[R–L] (male n = 52, M = 0.018, SD = 0.054; female n = 54, M = 0.004, SD = 0.040), t(104) = 1.582, P = 0.117. In males, R2D:4D was significantly higher than L2D:4D, t(51) = 2.412, P = 0.019, though there was no such difference in females, t(53) = 0.647, P = 0.520.
Pearson’s tests were conducted to examine associations between amniotic and maternal plasma testosterone levels and M2D:4D and D[R-L] in the newborn males and females (Table 1). There was a significant negative correlation between M2D:4D and amniotic testosterone in females (Fig. 1); in males, there was no significant correlation (Fig. 2). Comparison of the slopes showed that the association between amniotic testosterone and M2D:4D differed significantly between the two sexes. Amniotic testosterone was not correlated with D[R–L] in either males or females, and no statistically significant effects were observed for maternal plasma testosterone.
Table 1 Associations between amniotic and maternal testosterone and infant M2D:4D and D[R–L].

Note: T, testosterone; correlations are Pearson’s; all P values are two-tailed.

Fig. 1 Pearson’s correlation between amniotic testosterone and M2D:4D in females.
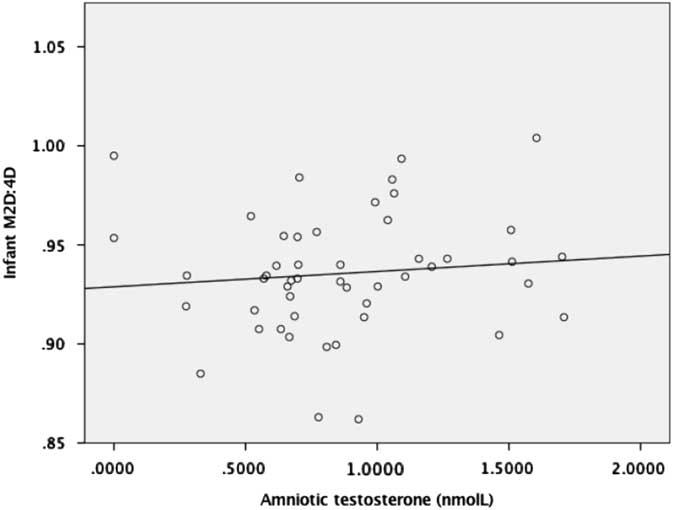
Fig. 2 Pearson’s correlation between amniotic testosterone and M2D:4D in males.
Ventura et al.Reference Ventura, Gomes, Pita, Neto and Taylor39 reported a significant negative correlation between maternal circulating testosterone levels and R2D:4D when male and female infants were analysed together. We therefore examined whether there were associations between amniotic and maternal testosterone and newborn M2D:4D and D[R–L] in the combined sample. Amniotic testosterone was negatively associated with M2D:4D, r(98) = −0.219, P = 0.029, and there was no significant correlation with D[R–L], r(98) = 0.171, P = 0.088. No significant effects were observed for maternal testosterone: M2D:4D, r(103) = −0.158, P = 0.107; D[R–L], r(103) = −0.129, P = 0.191.
Discussion
Mean digit ratio (M2D:4D) and directional asymmetry in digit ratio (D[R-L]) are frequently reported on as potential markers of prenatal androgen and oestrogen exposure. However, no previously published studies have examined whether these variables are correlated with sex hormones measured from amniotic fluid. The current study reanalysed data published by Ventura et al.,Reference Ventura, Gomes, Pita, Neto and Taylor39 and observed a negative correlation between M2D:4D and amniotic testosterone in newborn infants. The effect was statistically significant when the male and female samples were combined, and when females were examined separately. However, the correlation in males was not significant. Amniotic testosterone was not correlated with D[R–L] in the whole sample or in males or females separately. There were also no significant correlations between plasma testosterone assayed from pregnant mothers during the second trimester and subsequent M2D:4D or D[R-L] in their offspring.
The observation that amniotic testosterone was negatively correlated with M2D:4D in females should be considered in the context of the original findings presented by Ventura et al.Reference Ventura, Gomes, Pita, Neto and Taylor39 As amniotic testosterone was negatively correlated with L2D:4D (r = −0.3, P = 0.03) and R2D:4D (r = −0.24, P = 0.09), albeit the latter not significantly, the current finding is not surprising. The correlation between M2D:4D and amniotic testosterone in males presented in the current study was not significant. Although a negative correlation would be predicted,Reference Manning, Scutt, Wilson and Lewis-Jones1 Ventura et al.Reference Ventura, Gomes, Pita, Neto and Taylor39 reported that amniotic testosterone did not correlate significantly with R2D:4D (r = 0.14, P = 0.35) or L2D:4D (r = 0.004, P = 0.98) in males in this sample. Taken together, these findings suggest that L2D:4D (r = −0.3) in newborn females is approximately as strong a predictor of amniotic testosterone as is M2D:4D (r = −0.311), whereas R2D:4D is a slightly weaker predictor (r = −0.24). However, it should be reiterated that R2D:4D, L2D:4D and M2D:4D were not correlated with amniotic testosterone exposure in newborn males. This finding is more difficult to explain, as previous research indicates that negative correlations should be expected.Reference Manning, Scutt, Wilson and Lewis-Jones1
Directional asymmetry in digit ratio (D[R–L]) was not significantly associated with amniotic testosterone exposure in either male or female newborns. These findings may cast doubt on the efficacy of low D[R–L] (i.e., low R2D:4D relative to L2D:4D) as a proxy for high prenatal androgen exposure. However, an explanation for the lack of significant findings (which also applies to the analysis of M2D:4D) is that absolute testosterone concentration may be of less importance in determining digit ratio (or directional asymmetry in digit ratio) than is the ratio of testosterone to oestradiol.Reference Zheng and Cohn11, Reference Lutchmaya, Baron-Cohen, Raggatt, Knickmeyer and Manning38, Reference Manning44 It is noted that although the paper by Lutchmaya et al.Reference Lutchmaya, Baron-Cohen, Raggatt, Knickmeyer and Manning38 is widely cited as evidence for the effect of foetal testosterone on digit ratio, the only statistically significant correlation reported was between R2D:4D and the ratio of testosterone to oestradiol. Unfortunately, Ventura et al.Reference Ventura, Gomes, Pita, Neto and Taylor39 did not assay oestradiol, and so no replication attempt could be made here.
Another potential reason for the lack of association between amniotic testosterone and D[R–L] is that there is a certain amount of liability in 2D:4D after birth,Reference Knickmeyer, Woolson, Hamer, Konneker and Gilmore45–Reference Trivers, Manning and Jacobson47 and this might vary between the right and left hands. Trivers et al.Reference Trivers, Manning and Jacobson47 noted that 2D:4D in both hands increased during childhood, and that the effect for the left hand was stronger. This might be consistent with the observation that L2D:4D was significantly lower than R2D:4D in male infants in the current sample, whereas this pattern is not typically observed in adults.Reference Manning3 Further research should aim to examine associations between amniotic testosterone (and oestradiol) and digit ratio variables at later stages of development, to see whether correlations are present once digit ratios have become more stable. This research is particularly important considering that the only previously published studies of amniotic testosterone and digit ratio relate to newbornsReference Ventura, Gomes, Pita, Neto and Taylor39 and 2-year-old infants,Reference Lutchmaya, Baron-Cohen, Raggatt, Knickmeyer and Manning38 even though many studies use digit ratio to examine the effects of foetal sex hormones on adult phenotypic outcomes.
Maternal plasma testosterone was not significantly correlated with M2D:4D or D[R–L] in the current study. However, it is noted that the direction of the correlation for both M2D:4D and D[R–L] was negative for males, females, and the combined sample. This could suggest that real associations do exist between these variables, but that the analyses presented here were not powerful enough to detect them. This is consistent with the observation that Ventura et al.Reference Ventura, Gomes, Pita, Neto and Taylor39 reported maternal circulating testosterone to be negatively correlated with R2D:4D when males and females were analysed together (r = −0.2, P = 0.04), but not when each sex was examined separately. To investigate this possibility further, power analyses (using G*Power 3.1,Reference Faul, Erdfelder, Buchner and Lang48, Reference Faul, Erdfelder, Lang and Buchner49) were conducted to calculate the sample sizes required to detect significant effects (using two-tailed Pearson’s correlations) based on the effect sizes observed in the current study, 80% power, and α set at P < 0.05. For M2D:4D, the required sample sizes would be n = 179 for males, and n = 215 for females; for D[R–L], the required sample sizes would be n = 1287 (males) and n = 356 (females).
If the effects observed in the current study are representative of the true effect sizes (assuming true effects do exist) then large samples may be required when employing digit ratio as a proxy for foetal sex hormone exposure. However, there are several possible explanations for the weak and inconsistent effects observed here. For instance, it may be that digit ratio is more strongly influenced by sex hormone exposure during the first trimester, and that hormones assayed in the second trimester retain ‘echoes’ from earlier stages of development.Reference Manning and Fink40 Equally, measuring hormones at a single time-point in pregnancy likely does not adequately capture the complexities of the foetal hormonal environment. Importantly, it also remains unclear whether testosterone measured from maternal plasma or amniotic fluid can provide a good indicator of the levels present in foetal circulation.Reference Rodeck, Gill, Rosenberg and Collins50 These issues likely reduce the strength of correlation that is observable between such measures of foetal testosterone exposure and digit ratio.
There are additional limitations to the current study that should be acknowledged. First, the analyses presented here relate to a previously published datasetReference Ventura, Gomes, Pita, Neto and Taylor39 in which amniotic and maternal plasma testosterone have been examined in relation to digit ratio variables in neonates (specifically, R2D:4D and L2D:4D). Therefore, although the current study does provide new insights, it does not present information that relates to an independent sample. Second, although the sample is larger than that of the only other published studyReference Lutchmaya, Baron-Cohen, Raggatt, Knickmeyer and Manning38 that has examined amniotic testosterone in relation to digit ratio (n = 29), it is still only moderate in size. Third, though typical of studies of sex hormones measured from amniotic fluid, the relatively advanced median age of the mothers in this sample (37.90 years) may not be representative of pregnant women in the general population. Fourth, digit ratios were measured from photocopies, a method that has been shown to yield slightly lower (i.e., more masculinized) 2D:4D values compared with measures taken directly from participants’ hands.Reference Manning, Fink, Neave and Caswell51, Reference Ribeiro, Neave, Morais and Manning52 Fifth, as previously mentioned, no analysis of oestradiol was possible here. As the ratio of testosterone to oestradiol in amniotic fluidReference Lutchmaya, Baron-Cohen, Raggatt, Knickmeyer and Manning38 (but not in umbilical cord bloodReference Hollier, Keelan and Jamnadass33) has been found to predict subsequent 2D:4D, this is a considerable drawback. However, studies of amniotic fluid are scarce, and, due to recent advances in non-invasive clinical procedures, may not be replicated in future. For these reasons, it was deemed valuable to examine the possible associations between amniotic testosterone and previously overlooked digit ratio variables, despite the methodological limitations encountered.
Summary
Mean digit ratio (M2D:4D) was negatively correlated with amniotic testosterone in newborn females, although in males there was no significant effect. No correlations were observed between amniotic testosterone and directional asymmetry in digit ratio (D[R–L]). Although the findings may call into question the efficacy of using M2D:4D (in males) and D[R–L] (in males and in females) as proxies for prenatal androgen exposure, the importance of oestrogens in the development of digit ratio variables should not be overlooked. As many studies report findings from several predictor variables (e.g., R2D:4D, L2D:4D and D[R-L]), which can increase the likelihood of Type 1 errors, the findings from the current study may contribute to the debate regarding which should be prioritized in future research. Further studies should also aim to follow-up cohorts from which amniotic fluid has been collected, to better determine whether early exposure to androgens and oestrogens (and more specifically, the ratio of testosterone to oestradiol) can predict variance in digit ratio variables (R2D:4D, L2D:4D, M2D:4D and D[R-L]) at different stages of postnatal development.
Acknowledgements
We acknowledge Arium-Sistemas de Diagnóstico Lda for assuring quality control in all assays in Lisbon, Miss Olah Hakim (King’s College London) for her help in the laboratory, and Dr Ana Pita for helping to collect the newborns’ data.
Financial support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Conflicts of interest
The authors declare no conflicts of interest.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of relevant national guidelines on human experimentation set by the Hospital Centre of Central Lisbon (to which Dona Estefânia Hospital belongs), and with the Helsinki Declaration of 1975, as revised in 2008, and that the research was approved by the Dona Estefânia Hospital Ethics Committee.



