


Introduction
Birthweight (BW) has been considered an important marker of foetal growth that can influence the normal development of childrenReference Eriksson, Forsen, Tuomilehto, Osmond and Barker1,Reference Zhang, Kris-Etherton and Hartman2 . According to the classification of World Health OrganizationReference de Onis, Garza, Onyango and Rolland-Cachera3, BW is considered low when it is below 2499 g. Normal BW ranges from 3000 to <3999 g. Children born between 2500 and 2999 g are considered to have insufficient BW, while above 4000 g are having high BW. The two extremes of the BW spectrum (low and high BW) are associated with an increased risk of abdominal fat accumulation, reduced height-for-age and neuromotor disorders in childhoodReference Moura-Dos-Santos, Wellington-Barros, Brito-Almeida, Manhaes-de-Castro, Maia and Gois Leandro4–Reference Nuyt and Alexander6. In a previous study, children with low birthweight (LBW) were lighter and smaller than their pairs with reduced indices for weight-for-age and height-for-ageReference Tchamo, Moura-Dos-Santos, Dos Santos, Prista and Leandro7. These differences remained significant even after adjustment for age, gender, body size, fatness and skinfold thicknessReference Tchamo, Moura-Dos-Santos, Dos Santos, Prista and Leandro7. In addition, total breastfeeding duration and body weight gain in the first year of life showed positive significant association with childhood body mass index (BMI)Reference Lamb, Dabelea and Yin8.
During childhood, there is an additional energy cost compatible with the period of growth that can be influenced by metabolic and physiological restrictions, leading to unbalanced energy homeostasis and altering adequate growthReference Gao, Yan and Xiang9. Inherent adjustments in low- or high-energy intake can lead to restricted growth, reduction of fat-free mass (FFM), body fat accumulation and increased risk of metabolic diseasesReference Moura-Dos-Santos, Wellington-Barros, Brito-Almeida, Manhaes-de-Castro, Maia and Gois Leandro4,Reference Lazzer, Patrizi, De Col, Saezza and Sartorio10,Reference Raaijmakers, Jacobs and Rayyan11 . Variation in anthropometric parameters, such as height, weight and circumferences of head, waist and hip, resulting from an early nutritional imbalance (undernutrition or overnutrition) during perinatal life (gestation and lactation) may induce basal metabolic rate (BMR) changesReference Heymsfield, Chirachariyavej, Rhyu, Roongpisuthipong, Heo and Pietrobelli12,Reference Lazzer, Bedogni and Lafortuna13 . BMR is defined as the rate of energy metabolism of an organism at rest under postabsorptive conditions in a thermoneutral environmentReference Luciano, Bolognani, Rossi, Suzuki and Zoppi14. A previous study observed that BW adjusted for age and FFM was inversely associated with BMR (r = −0.12; P < 0.01) in adulthoodReference Sandboge, Moltchanova and Blomstedt15. Recently, it was observed that the low consumption of energy, protein and fat during the first three weeks of life can predict adult body composition and BMRReference Suikkanen, Matinolli and Eriksson16. As the main predictor of BMR is the FFM, a lower lean tissue mass may be implicated within the reduction of BMR and in body fat accumulationReference Muller, Langemann and Gehrke17. It was demonstrated that early malnourished children (9 years ± 6 months) presented lower capacities to develop force under voluntary or induced conditionsReference Paiva, Souza and Canon18. Lower BW is linked to reduced motor performance including muscle strength, muscle endurance and cardiorespiratory fitness in children and adolescentsReference Ridgway, Brage, Anderssen, Sardinha, Andersen and Ekelund19. However, a previous study showed that LBW alone cannot be considered as a biological determinant of physical growth, body composition or physical fitness in children but induces permanent deficit in muscle strength and running speed performance in childrenReference Moura-Dos-Santos, Wellington-Barros, Brito-Almeida, Manhaes-de-Castro, Maia and Gois Leandro4,Reference Moura-Dos-Santos, De Almeida, Manhaes-De-Castro, Katzmarzyk, Maia and Leandro5,Reference Dos Santos, Moura Dos Santos and Almeida20 .
The positive linear relationship between BMR and FFM is given for children, lean adolescents and lean and obese adultsReference Dulloo, Jacquet, Miles-Chan and Schutz21. However, less is known about the mediation effect of anthropometry, body composition and physical fitness on the association of BW and BMR in children. Using the model of mediation effects, we hypothesised that BW is a determinant for basal energy metabolism variation during childhood by the changes observed in anthropometry, body composition and physical fitness. Thus, the present study aimed to analyse the mediation effect of anthropometry, body composition and physical fitness on the association of BW and BMR in children aged 7–10 years.
Methods and procedures
Sample
The present study was conducted in the city of Vitória de Santo Antão, located in an economically poor rural zone of the state of Pernambuco, in the Northeast of Brazil. The sample size was estimated in Epi Info 6.04 given the following conditions: an error of ±5%, a power of 80% and a relative risk of 2.0 for events in low BW versus normal BW subjects, i.e., a ratio of 1:2. A total of 499 healthy children (254 males and 245 females), aged 7–10 years, born at term in Vitória de Santo Antão, participated in this study. Children were randomly selected from the six of the nine public schools in Vitoria de Santo Antao. Information on BW was obtained from health booklets in which this information had been recorded by nurses and/or paediatricians. Written informed consent to participate in the study was obtained from the parents or legal guardians of each child.
Anthropometry and body composition
The evaluation of children’s anthropometric parameters was performed at the same conditions (room, light and temperature at school) and at the same schedule of the day (between 8 and 9 a.m.). Measurements included: Body weight: measured to the nearest 0.1 kg with a digital scale (Filizola, São Paulo, Brazil); children were lightly dressed and barefoot. Body height: measured to the nearest 0.5 cm using a portable stadiometer (Sanny, São Paulo, Brazil) with each child’s shoes off, feet together and head in the Frankfurt horizontal plane. Head circumference: the tape was placed over the occipital protuberance and the arch of the eyebrows (values were expressed in centimeter). Waist circumference: the smallest circumference between the last rib and the iliac crest (values were expressed in centimeter). Hip circumference: held around the widest part of the trochanter (buttocks) (values were expressed in centimetre). Anthropometric evaluation followed the protocol proposed by Lohman and GoingReference Lohman and Going22.
The evaluation of body composition included: BMI calculated using the standard formula [weight (kg)/height2 (m)]; triceps and subscapular skinfolds that were measured with a Lange caliper (Lange, Santa Cruz, California, USA). The percentage of body fat (BF%), fat mass (kg) and FFM (kg) were estimated using previous studiesReference Moura-Dos-Santos, De Almeida, Manhaes-De-Castro, Katzmarzyk, Maia and Leandro5,Reference Dos Santos, Moura Dos Santos and Almeida20 considering the equations proposed by Lohman and GoingReference Lohman and Going22. Measurements of anthropometry were performed by a trained researcher prior to physical fitness tests.
Physical fitness tests
Health-related physical fitness was assessed according to the FitnessgramReference Meredith and Welk23 and Eurofit24 standardised test batteries. The chosen tests were (a) handgrip strength (measured with the right hand) using a handgrip dynamometer (Saehan, Flintville, USA); (b) sit and reach (as a measure of flexibility); (c) curl-ups (as an indicator of dynamic muscle endurance of abdominal muscles); (d) standing long jump (a measure of the explosive power of the lower limbs); (e) square test as a measure of agility (complete a weaving running course [4 × 4 m2] in the shortest possible time); and (f) a 20 m dash run (to evaluate running speed in the shortest possible time)Reference Moura-Dos-Santos, Wellington-Barros, Brito-Almeida, Manhaes-de-Castro, Maia and Gois Leandro4,Reference Moura-Dos-Santos, De Almeida, Manhaes-De-Castro, Katzmarzyk, Maia and Leandro5 .
Basal metabolic rate
The equation used to estimate the BMR was that developed by the FAO/WHO/UNU25 for children between 3 and 10 years of age.
BMR (kcal/day):
-
1. Males = 22.706 × weight (kg) + 504.3
-
2. Females = 20.315 × weight (kg) + 485.9
Statistical analysis
Data analysis was conducted using the statistical package SPSS version 23 (IBM Corp., Armonk, NY). Exploratory data analysis was used to identify potentially inaccurate information and outliers. Descriptive statistics are presented as means and standard deviations, minimum and maximum values. Potential interaction factors (i.e., differences between sex and ages) were evaluated using the Kruskal-Wallis and Mann-Whitney tests. Spearman correlation was used to test the association between BW and the anthropometric measures and body composition and physical fitness variables (selection of mediators). To explore our hypothesis, a single-mediator analysis (SMA) to each variable and a multi-mediator analysis (MMA) were tested using HayesReference Hayes26 PROCESS macro for SPSS. This method rigorously tests simultaneous estimates for direct, indirect and total effects with a bootstrap approach (5000 samples) to obtaining 95% confidence intervals. The mediation occurs if the previously significant relationship between BW (X) and BMR (Y), represented by total effect, is no longer significant with the addition of the mediator (Fig. 1). In addition, the mediation was considered significant when the coefficients of the indirect effect were significant (p < 0.05). An MMA was constructed using backward elimination, starting with all mediators that were significant in the SMA (model 1). Then, the selected mediators that were not significant in the MMA were eliminated in order to find a model to better explain the data (model 2). The MMA allows assessing the effect among multiple mediators selected in the relation between BW and BMR in a single model, where each mediator will be accounted considering the effect of the other mediator. Percent mediation (PM) was used to calculate the effect size. The PM can be interpreted as the ratio of the indirect effect to the totalReference Preacher and Kelley27.
 $${\rm{PM}} = {{ab} \over {ab + c'}} = {{ab} \over c}$$
$${\rm{PM}} = {{ab} \over {ab + c'}} = {{ab} \over c}$$
where a is the slope linking X to m, b is the conditional slope linking m to Y, c is the total effect of X on Y and c’ is the conditional slope linking X to YReference Preacher and Kelley27.
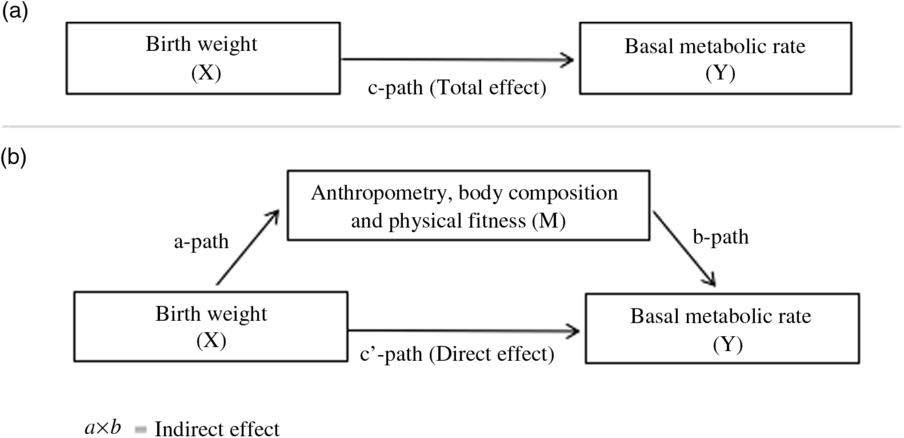
Fig. 1. Schematic demonstration of mediation effect.
Results
The descriptive information of the studied population related to anthropometry, body composition, physical fitness and BW split by genders are presented in Table 1. There were no differences between boys and girls (BW, p = 0.452 and BMR, p = 0.965). From the spearman correlation, BW was positively correlated with body height, head circumference, waist and hip circumferences and handgrip strength and negatively correlated with running speed for boys (Table 2). For girls, only body height (p = 0.041), hip circumference (p = 0.032) and handgrip strength (p = 0.049) were correlated with BW. Those variables were selected as probable mediators, due to their significant relation with BW (Table 2).
Table 1. Sample descriptive characteristics (N = 499)
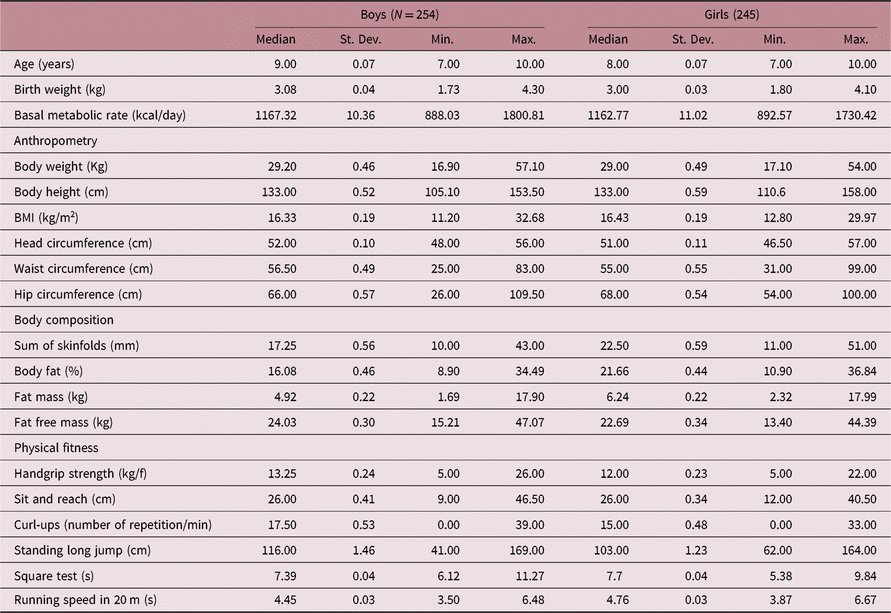
Table 2. Spearman correlations between birthweight, anthropometric, body composition, and physical fitness variables.

Significant results (p < 0.05) are in bold.
The mediation analyses were conducted by isolating each proposed mediator (model 1) and by a simultaneous analysis of multiple mediators (model 2) observing the direct, indirect, total effects and PM. Results from the mediation model predicting boys and girls BMR by BW are summarised in Table 3. Consistent with our hypothesis, results indicated that there were significant indirect effects in children’s anthropometry, body composition and physical fitness on BW and BMR relationship. The mediation of variables can be observed because indirect effects were statistically significant in the mediation models. In SMA, for boys, there were significant indirect effects for height, head circumference, waist circumference, hip circumference and handgrip strength. The height accounted for 85% of the mediation of BW on BMR. The handgrip strength and waist circumference accounted for approximately 70% of the mediation of BW on BMR. The hip circumference and head circumference accounted approximately 50%–60% of the mediation of BW on BMR. There was no significant indirect effect of running speed in BW and BMR relationship for boys.
Table 3. Single- and multi-mediation coefficients, indirect effect and 95% bias-corrected confidence interval predicting effects of birth weight on basal metabolic rate.

*p < 0.05; **p < 0.001.
aDifferent sample size: 1—Single-mediation Model; 2—Multi-mediation model.
For girls, there were significant indirect effects for height, hip circumference and handgrip strength. The hip circumference accounted for 72.82% of the mediation of BW on BMR. The height and handgrip strength accounted for approximately 50%–60% of the mediation of BW on BMR. In MMA for girls, there were significant indirect effects for the model with height, hip circumference and handgrip strength. The model accounted for 79.08% of the mediation of BW on BMR. The main contribution to the model was hip circumference with 56.72% of mediation, followed by height with 16.23%, and the lowest contribution to the model was handgrip strength with 6.13% of mediation.
In MMA for boys, indirect effects were significant for total, height, head circumference and waist circumference; however, the results suggest that the effect of the multiple mediators (total) was considered a suppressor or an inconsistent mediatorReference Nitzl, Roldan and Cepeda28,Reference MacKinnon, Krull and Lockwood29 . An inconsistent mediation can be observed when the specific mediated effects have opposing signs, for example, direct effect presented negative coefficient (−4.10, 95% CI: −16.83 –13.80) and indirect effect (44.04, 95% CI: 13.84–74.36), and when the total effect is smaller than the indirect effect; consequently, a PM above 100% (110% for the present model) is also indicative of inconsistent mediationReference Nitzl, Roldan and Cepeda28,Reference MacKinnon, Krull and Lockwood29 .
Given these inconsistence, a confounding factor identification was performed by backward elimination in model 2 in the MMA. Height was identified as a suppressor variable, once excluded from model 2, the head and waist circumferences mediation had indirect (33.50, 95% CI: 6.36–60.97) and direct effects (6, 43, 95% CI: −12.47 – 25.34) and PM was less than 100% (83.87%). The main contribution to the model was waist circumference with 63.97% of mediation, followed by head circumference with 19.90% of mediation.
Discussion
The current investigation examined the mediation effect of anthropometry, body composition and physical fitness on the association between BW and BMR for boys and girls aged 7–10 years. In the present study, the anthropometric variables associated with BW were body height, head, hip and waist circumferences for boys and body height and hip circumference for girls. These findings corroborate with previous studiesReference Moura-Dos-Santos, Wellington-Barros, Brito-Almeida, Manhaes-de-Castro, Maia and Gois Leandro4,Reference Moura-Dos-Santos, De Almeida, Manhaes-De-Castro, Katzmarzyk, Maia and Leandro5,Reference Dos Santos, Moura Dos Santos and Almeida20,Reference Sachdev, Fall and Osmond30 , which showed a relationship of BW with anthropometric variables, confirming their importance as predictors. On the other hand, we showed that body composition variables (BF% and sum of skinfolds) did not present a significant relationship with BW. Our data corroborate with a previous study that investigated the early influences of BW on later risk factors for cardiovascular disease in adolescents aged 13–16 years, where BW was associated with lean mass, but not with fat massReference Zhang, Kris-Etherton and Hartman2. In the current study, gender differences were observed in terms of correlation between BW and body height, head, hip and waist circumferences for boys. For girls, only body height and hip circumference were correlated with BW. Accordingly, a previous study in Mozambique has shown that boys (7–10 years old) born with low BW presented lower body height and circumferences than their normal BW pairsReference Tchamo, Moura-Dos-Santos, Dos Santos, Prista and Leandro7. In addition, taking account of predictors of BMI such as BW, it has also been suggested that boys are more likely to have higher BMI or be more obese than girlsReference Gomes, Katzmarzyk, dos Santos, Souza, Pereira and Maia31.
In the present study, after the identification of the probable mediators in the direct effects, the mediation analysis indicated that handgrip strength played this role for both genders. The relationship between BW and energy metabolism, expressed by the total effect, has already been well documented in previous studiesReference Sandboge, Moltchanova and Blomstedt15,Reference Matinolli, Hovi and Levalahti32,Reference Matinolli, Hovi and Mannisto33 Accordingly, a previous study found a negative correlation between BW and BMR expressed per unit of FFM (r = −0.158; p < 0.001)Reference Eriksson, Forsen, Tuomilehto, Osmond and Barker1. Sandboge, MoltchanovaReference Sandboge, Moltchanova and Blomstedt15 found a positive correlation between BW and BMR, but after adjustment for FFM in women, there was a negative linear association. In the same study, men born with either low or high body weights had the highest BMR even after the adjustment for FFM and fat mass. These results show the influence of FFM on the relationship between BW and energy metabolism. In the present study, a reduced coefficient (less than 30) in the total effect after the inclusion of mediators (direct effect) was found in the analysis. Likewise, the mediating role of each variable is given by the parallel relationship between BW and BMR, configuring the indirect effect of those variables in the mediation.
Our data showed that body height was an important mediator of BMR for both genders. Body height has been used to estimate energy metabolism in previous studies that considered the energy metabolism of childrenReference Sachdev, Fall and Osmond30,Reference Joint34 . In Jamaican 7–8-year-old children, it was shown that a short-stature group had a reduced BMR when compared to a normal-stature groupReference Wren, Blume, Mazariegos, Solomons, Alvarez and Goran35. A hypothesis reported by Heymsfield, ChirachariyavejReference Heymsfield, Chirachariyavej, Rhyu, Roongpisuthipong, Heo and Pietrobelli12 indicates that relative to body weight and height, individuals differ in their proportions of heat-producing tissues, such as skeletal muscle and brain mass, an important determinant for BMRReference Heymsfield, Chirachariyavej, Rhyu, Roongpisuthipong, Heo and Pietrobelli12,Reference Heymsfield and Pietrobelli36 .
In the present study, we identify head, waist and hip circumferences as mediators of BMR for boys. For girls, only height and hip circumference were mediators for BMR. The high metabolic cost of the brain supports the identification of head circumference as an important mediator of BMR. Head circumference is commonly used as an indirect measure of brain volume, neural development and cognition development in childrenReference Treit, Zhou and Chudley37. The brain presents one of the highest specific metabolic rates (240 kcal/kg/d), and additional brain mass explained a 2% increase of the variance to the prediction of BMRReference Javed, He and Davidson38. The relationship among waist and hip circumferences, fat distribution and BMR has been demonstrated. Nielsen, HensrudReference Nielsen, Hensrud, Romanski, Levine, Burguera and Jensen39 suggested that a variation of ~3.4 kcal/kg/day of BMR can occur due to body fatness. However, their study demonstrated that these values could be twice higher, suggesting that there are additional metabolic effects of adipose tissue on the increase of BMRReference Treit, Zhou and Chudley37.
Physical fitness and motor coordination are an integral part of children’s normal health and neural developmentReference Moura-Dos-Santos, De Almeida, Manhaes-De-Castro, Katzmarzyk, Maia and Leandro5. In order to evaluate the body’s abilities related to health and sports performance, a battery of physical fitness tests is requiredReference Beunen, Ostyn and Simons40. Physical fitness is often related to components such as cardiorespiratory fitness, muscular strength, muscular endurance, body composition and agility and flexibilityReference Beunen, Ostyn and Simons40. A permanent deficit in handgrip strength and running speed was associated with LBW, and these deficits could be associated with the limited metabolic capacity of skeletal muscles (smaller muscle size, low proportion of fast-twitch muscle fibres and an impairment in the biomechanical properties of skeletal muscle) as seen in LBW childrenReference Moura-Dos-Santos, Wellington-Barros, Brito-Almeida, Manhaes-de-Castro, Maia and Gois Leandro4. Considering that more specific aspects associated with skeletal muscles were not evaluated in the present study, we suggest that the indirect effect of the variables on mediation may be related to the metabolic capacity of the skeletal muscle. In the present study, although handgrip strength and running speed are correlated with FFM, only handgrip strength mediated the relation between BW and BMR. Byrne and WilmoreReference Byrne and Wilmore41 showed that an increase in the FFM in highly adult trained subjects promoted an increase in BMR. In children, the literature remains divergent about the growth rate of FFM and changes in the BMR. Thus, studies are needed to elucidate the divergent issues regarding physical exercise and the differential contributions of FFM, since it is the main determinant of BMR and energy metabolism in children.
Each variable presented an isolated contribution to the relationship between BW and BMR; however, under natural conditions, the mediators influenced together the outcomes instead of in isolation (as suggested by the SMA). In MMA, it was observed that the variables (together) mediated 80% of the relationship between BW and BMR. The mediating effect of anthropometric variables and physical fitness on the relationship between BW and BMR is plausible, since nutrient supply during the critical period of development is determinant for the adequate growth of different organs and systemsReference Harding42. Some hypotheses have addressed to the study of variation in the size of organ and the growth of a tissue in detriment of anotherReference Aiello and Wheeler43,Reference Navarrete, van Schaik and Isler44 . Aiello and WheelerReference Aiello and Wheeler43 suggest that the metabolic requirements of relatively large brains are offset by a corresponding reduction of the gut. Nonetheless, Navarrete et al. Reference Navarrete, van Schaik and Isler44 attribute this increase to the reduced adipose depots. These changes in the relative size of organs contribute to the energy balance of an individualReference Aiello and Wells45. The different contribution of tissues to total BMR is the basis of studies that try to explain some evolutionary changes in body proportionsReference Navarrete, van Schaik and Isler44,Reference Aiello and Wells45 . Indeed, the predictive effect of the BW on the development of body structures could explain an energetic rearrangement compatible with changes in BMR.
The suppressor effect, found in boys MMA, is present when the direct effect and the indirect effect presented contrast signsReference MacKinnon, Krull and Lockwood29. Although height had a mediation effect when evaluated in SMA, the MMA model accounting for height generated a negative relationship between BW and BMR (direct effect), assuming an inconsistent featureReference MacKinnon, Krull and Lockwood29,Reference O’Rourke and MacKinnon46 . The height played a suppressing role in the effects of mediation, and one hypothesis for this effect is the collinearity among model variables.
The limitations of the present study related to BW are the lack of information about the period of gestational age and lactation that could best characterise the conditions that determine different body weights at birth. In addition, lack of information about nutritional habits or food intake could be important for the calculation of BMR. Although the use of indirect calorimetry for determination of the BMR is the most precise method to evaluate the energy metabolism, we used the prediction equation as suggested by previous studies and Food and Agriculture Organization of the United Nations (FAO, 2004), addressing the BMR across all age groups and various living conditions. From these, an equation was developed for specific BMR estimates for infant population. In addition, the study included the measurement of FFM, an important determinant of BMR.
Conclusion
The current study showed that changes in the BMR are related to BW and also can be explained by changes in height, head, waist and hip circumferences and muscle strength (handgrip strength), important markers of child development. These findings appear to be the bridge connecting early-life events and the long-term consequences (later risks of metabolic disease). From a public health perspective, given the associations between physical exercise and increased energy metabolism, our findings suggest the importance of physical activity for school children, especially for populations with higher prevalence of perinatal malnutrition in order to minimise the effects of LBW on growth and development.
Acknowledgments
We thank all children and their families for participating in this study. The authors have stated that they had no interests that might be perceived as posing a conflict or bias. The English text of this paper has been revised by Sidney Pratt, Canadian, MAT (The Johns Hopkins University), RSAdip – TESL (Cambridge University).
Financial support
This study was received financial support by the National Council for Scientific and Technological Development (CNPq), Coordination for the Improvement of Higher Level (or Education) Personnel (CAPES-COFECUB 797-14) and State of Pernambuco Science and Technology Support Foundation (FACEPE).
Author’s contribution
The contributions of each author are as follows: Isabele Goes Nobre: Analysis and interpretation of data, wrote the article; Marcos Andre Moura-dos-Santos, Isabela Ribeiro, Tafnes Oliveira and Eveline Fonseca: Acquisition of data, analysis and interpretation of data; Gabriela Goes Nobre, Gabriela Carvalho and Ravi Marinho: Acquisition of data; Wylla Tatiana Ferreira e Silva and Julie-Anne Nazare: Final revision and substantial to analysis and interpretation of the data, final revision of the article; Carol Gois Leandro: Conception, design and intellectual content of the article. Final revision.
Conflicts of interest
Authors declare no conflict of interest.
Ethical standards
This study was approved by the ethics committee of the Centre of Health Science, Federal University of Pernambuco (protocol number 0175.0.172.000–09) in accordance with the ethical standards of the 1964 Helsinki Declaration.




