Introduction
Birth outcomes were critical infant health measures and predictive indicators of infant growth and development. Reference Gluckman, Hanson, Cooper and Thornburg1 Adverse birth outcomes severely affected the physical and mental health of maternal and child. Reference Hauspurg, Ying, Hubel, Michos and Ouyang2,Reference Lawn, Blencowe and Oza3 Infants with low birth weight not only had higher neonatal mortality and morbidity than those of normal birth weight Reference Iliodromiti, Mackay and Smith4,Reference Zeng, Cheng and Dang5 but also could be small for gestational age (SGA). Reference Lawn, Blencowe and Oza3,Reference Ray, Park and Fell6,Reference Lee, Katz and Blencowe7 In addition, medical resources and antenatal care providers were restricted for the infants with an adverse birth outcome in developing and populous countries, particularly in China. Therefore, it was imperative to identify risk factors for adverse birth outcomes. Previous research reports indicated that the altitude of residence was independently associated with an increased birth weight reduction and had a general effect on all births. Reference Jensen and Moore8,Reference Yip9 However, to date, the majority of researches focused on the effect of high altitude on infant birth outcomes. Reference Jensen and Moore8–Reference Dang, Yan and Yamamoto16 The U.S. natality files reported that infants born at higher altitudes (>2000 m) had a twofold to threefold increase in low birth weight rate compared with those at sea level. Reference Yip9 A retrospective cohort study also reported a significant difference in birth weight across low (0–1999 m), moderate (2000–2900 m), and high (3000–4340 m) altitudes in Peru. Reference Levine, Gonzales and Tapia13 And a study showed that children above 3500 m had 2–6 times the risk of stunting compared with those at 3000 m in Tibet of China. Reference Dang, Yan and Yamamoto16 As described above, the high altitude was an important environmental factor influencing adverse birth outcomes. However, most people in the world resided in areas with low-to-medium altitudes. Fewer studies evaluated the association of low-to-medium altitude with infant birth outcomes (birth weight, gestational age, and SGA) in China. Reference Mi, Lin, Liu, Zhang and Cao17 Furthermore, the dose–response relationship between low-to-medium altitude and birth outcomes was less common. Given that the majority of worldwide population lived at the low-to-medium altitude areas, especially in China, assessing the association of altitude with birth outcomes was considered important for identifying any potential health risks arising from living at low-to-medium altitudes and informing health policies to reduce these risks.
Therefore, the present study aimed to explore the association of low-to-medium altitude with birth outcomes (birth weight, gestational age, and SGA) and the dose–response relationship between low-to-medium altitude and birth outcomes using the data from a large population-based cross-sectional survey in Northwest China.
Methods
Study design and participants
A population-based cross-sectional epidemiological survey with the purpose to investigate the risk factors for birth outcomes was conducted between August and December 2013 in Shaanxi province of Northwest China. Infants born during 2010–2013 and their mothers were recruited using a stratified multistage random sampling method that had been described elsewhere previously. Reference Li, Liu and Zhang18–Reference Yang, Dang and Cheng20 Briefly, according to the proportion of distribution between rural and urban residents and the fertility level in the population of the whole province of Shaanxi, China, 20 counties and 10 districts were sampled randomly. In each sampled county, six villages each from six townships were selected randomly, and in each sampled district, six communities each from three streets were selected randomly. Then, 30 and 60 participants were selected randomly in each sampled village and community, respectively. Of 32 400 pregnant women invited, 30 027 completed the questionnaire in this survey (response rate: 92.7%). Fig. 1 showed the flow chart with the exclusion criteria in this study. Women were required to provide written informed consent before being allowed to participate in this survey, and the research protocol was approved by the Human Research Ethics Committee of Xi’an Jiaotong University Health Science Center (No. 2012008).

Fig. 1. Study flow chart with exclusion criteria.
Ascertainment of altitude
Shaanxi province is located in Northwest China. It has an average altitude of 1127 m, and 90% of the area is between 500 and 2000 m above the sea level. Geographically, the terrain of Shaanxi area is higher in the north and south but lower in the middle. The population distribution of Shaanxi province is concentrated in the middle but sparse in the north and south. 21 It provided an opportunity to investigate the association of birth outcomes with low-to-medium altitude. Altitude measured with an altimeter (Garmin eTrex 20, version 20.0; Garmin, USA) was determined in meters (accurate to 0.1 m) at the village/community clinics or village/community committee house around which most of the mothers lived. The altitude of the mother’s living places in this survey ranged from 187 to 1538 m above the sea level. According to the altitude distribution map of Shaanxi province in the White Paper on Shaanxi Geographical Situation issued by Shaanxi Bureau of Surveying, residential altitude was categorized into three comparison groups in our analysis (<500, 500–999, and 1000–1538 m).
Ascertainment of birth outcomes
Focused birth outcomes in the present study were birth weight, gestational age, and SGA. Birth weight was abstracted from a review of Medical Certificate of Birth, and it was measured with a baby scale with precision to the nearest 10 g within 1 h after delivery. Gestational age (in weeks) was calculated from the interval between the first day of the last normal menstrual period and the date of birth, Reference Li, Ye, Zhang, Li, Liu and Ren22 and SGA was defined as the infant whose birth weight <10th percentile based on the gestational age–gender-specific Chinese reference for fetal growth. Reference Zhu, Zhang and Zhang23
Assessment of covariates
The basic information regarding participants was obtained via retrospective in-person interviews using standardized questionnaires. Lots of factors could confound the association between altitude and birth outcomes. Based on a comprehensive consideration of previous literature and significant differences across altitude levels in our analysis, Reference Zeng, Cheng and Dang5,Reference Levine, Gonzales and Tapia13,Reference Huang, Wu, Zhao, Hu, Yang and Chen24–Reference Kang, Dang and Zeng28 demographic and socioeconomic status, healthcare characteristics, maternal health, and dietary nutrition during pregnancy should be considered to adjust. Potential confounding variables included residence (urban and rural), maternal age (<25, 25–29, 30–34, and ≥35), maternal educational status (uneducated , primary, secondary, high school, college, and above), household wealth index (poor, medium, and rich), nulliparity (yes or no), Kessner index (inadequate, intermediate, and adequate), pregnancy-induced hypertension during pregnancy (yes or no), smoking (yes or no), folic acid supplement during pregnancy (yes or no), iron supplement during pregnancy (yes or no), multi-micronutrient use during pregnancy (yes or no), gender (male or female), and gestational age (in weeks). Smoking involved active and passive smoke during pregnancy; active smoking was defined as at least one cigarette per week and continuous or cumulative for 3 months or more, and passive smoking was defined as being exposed to smoker tobacco for more than 15 min/d. Gestational age was adjusted as continuous variables as it showed a linear relationship on birth weight. Reference Zhu, Zhang and Zhang23 Infant age and sex were not included in the confounder list because they had been accounted for when we defined SGA. The household wealth index was established by principal component analysis according to the variables of the family economic level (monthly income, monthly expenditure, housing condition, and vehicle), and then the index was divided into trisection indicating poor, medium, and rich household. Reference Filmer and Pritchett29 Kessner index was synthesized to reflect the availability of prenatal health services, which was classified as inadequate, intermediate, and adequate according to a fixed combination of values on the trimester of prenatal care start, the total number of prenatal visits, and the gestational age at delivery. Reference Huang, Wu, Zhao, Hu, Yang and Chen24,Reference Bloch, Dawley and Suplee30 In brief, women whose prenatal care started in the third trimester or whose number of prenatal visits was less than recommended visit of infant gestational week at delivery were classified into the inadequate prenatal care category. Accordingly, women who started in the first trimester and the number of visits she received was coinciding with the recommended visit of infant gestational week at delivery were classified into the adequate prenatal care category. Women with any other combinations of values concerning relevant variables were assigned to the intermediate category.
Statistical analysis
The statistical analysis followed logically three steps. First, we compared sociodemographic characteristics, risk factors, and birth outcome data across the three groups of altitude. The characteristics of participants were described as the mean ± SD or median (interquartile range, IQR) for the quantitative variable, and as number (percentage) for the categorical variable. χ2 test for categorical variables and one-way analysis of variance (ANOVA) for continuous variables were performed in univariate analysis. Second, the generalized linear models with identity-link function were set up in which birth weight or gestational age was used as the dependent variables and altitude used as the independent variable (continuous for every 100-m increase or three altitude categories). And the generalized linear model with the logit-link function was established to investigate the association of altitude with SGA (continuous for every 100-m increase or three altitude categories). Two kinds of models were established. Model 1 was unadjusted one, and model 2 was adjusted for potential confounders as sociodemographic characteristics and risk factors including residence, maternal age, maternal educational status, household wealth index, nulliparity, Kessner index, smoking, pregnancy-induced hypertension during pregnancy, folic acid supplement, iron supplement, multi-micronutrient use, gender, and gestational age. Concomitantly, a test for linear trend was performed by incorporating the altitude levels as a linear predictor using the median value in each regression model. Third, to graphically characterize the dose–response relationship between altitude (in m) and birth outcomes, restricted cubic spline (RCS) function with three knots located at the 5th, 50th, and 95th percentiles of the altitude distribution was further used while setting the median as the reference value. Adequate models selection based on the Akaike information criterion (AIC) values were calculated according to the −2Log(L) + 2n formula in which L delegated the maximum likelihood value and n was the number of parameters of each model (including the intercept). The better fitted model was determined as lower AIC. In the RCS model adjusted for potential confounders above, significantly statistical test for overall association meant that altitude was significantly associated with birth outcome whatever the shape of the association. Meanwhile, if the test for the nonlinear association was also significant statistically, it indicated that the nonlinear association between altitude and birth outcome existed. RCS function with three knots included two splines, S 0 and S 1, with their respective estimates, and testing the nonlinear association between altitude and birth outcome was equivalent to testing the null hypothesis that the value of the estimate of the S 1 spline equaled 031. To further test the robustness of the association between altitude (in 100 m) and birth outcomes, we further conducted the subgroup analysis by gender, residence, maternal age (<35 or ≥35 years), maternal educational status (≤9 or >9 years), and household wealth index after adjusting for potential confounders above except for subgroup variable. Besides, no adjustment for multiple tests had been performed for the larger sample size, and the results were to be interpreted as exploratorily.
Database was established using Epidata 3.1 (version 3.1; CDC, Atlanta, GA, USA) and duplication was adopted for data entry. All statistical analyses were performed using SAS software (version 9.4; SAS Institute Inc., Cary, NC, USA). A two-tailed P value of less than 0.05 was considered statistically significant.
Results
Population characteristics
Totally 27 801 women and their infants were included in our analysis, 34.2% (n = 9505), 40.5% (n = 11 248), and 25.4% (n = 7048) resided at <500, 500–999, and 1000–1538 m altitudes, respectively (Fig. 1). As presented in Table 1, the maternal characteristics across three groups of residential altitude. Residence, maternal age, maternal educational status, household wealth index, nulliparity, Kessner index, smoking, pregnancy-induced hypertension, folic acid supplement, iron supplement, and multi-micronutrient use were significantly different among the three groups of residential altitude. Table 1 and Fig. 2 display birth outcomes across the three groups of residential altitude. The mean birth weight was 3268 ± 459 g and the mean gestational age was 39.6 ± 1.3 weeks, while the prevalence of SGA was 14.3%. The mean birth weight (3309 ± 458, 3256 ± 456 3230 ± 460, P trend < 0.001), mean gestational age (39.6 ± 1.3, 39.7 ± 1.3, 39.7 ± 1.2, P trend < 0.001), and SGA (11.4%, 14.7%, and 17.6%, P trend < 0.001) were significantly different across the three groups of altitude.
Table 1. Maternal characteristics at residential altitude in Northwest China during 2010–2013

Values are mean ± SD or n (%).
P values shown for the differences among groups were derived from χ 2 tests for categorical variables, and one-way ANOVA for continuous variables.
Values for some characteristics may not be equal to 100 because of rounding.

Fig. 2. Differences of infant birth weight, gestational age, and prevalence of SGA at various residential altitudes in Northwest China during 2010 to 2013. SGA, small for gestational age. P trend was calculated using the median value of each altitude levels as continuous variables.
Residential altitude and birth outcomes
Table 2 displays the association of altitude with birth outcomes. The median residential altitude was 640 (IQR 556) m and 416.0 (IQR 43.2) m, 691.0 (IQR 267.0) m, and 1156.0 (IQR 163.2) m in three groups of altitude, respectively. After adjustment for potential confounders, each 100-m increase in altitude was associated with reduced birth weight (difference −6.4, 95% CI −8.1, −4.6 g), a slight increase of gestational age (difference 0.015, 95% CI 0.010, 0.020 week), and an increased risk of SGA birth (odds ratio (OR) 1.03, 95% CI 1.02, 1.04). Similarly, compared with those born to mothers living at altitude <500 m, the birth weight of newborns at an altitude of 500–999 m was reduced by 25 g (adjusted mean difference −25.0, 95% CI−37.5, −12.5 g) and 50.7 g for the newborns at an altitude of 1000–1538 m (adjusted mean difference −50.7, 95% CI−65.4, −36.1 g). The women living at an altitude of 1000–1538 m had a slight longer gestational age (adjusted mean difference 0.083, 95% CI 0.041, 0.125 week) compared with those living at an altitude <500 m. By comparison with those at an altitude <500 m, the newborns at 500–999 m had 10% risk of being SGA (adjusted OR 1.10, 95% CI 1.01, 1.20), and this figure was about 28% for those at an altitude of 1000–1538 m (adjusted OR 1.28, 95% CI 1.17, 1.41).
Table 2. The association of residential altitude with birth outcomes (differences, odds ratios and 95 % confidence intervals)

Ref., referent values.
Model 1 was crude difference or crude OR.
For birth weight, model 2 was adjusted for residence, maternal age, maternal education, nulliparity, Kessner index, household wealth index, smoking, pregnancy-induced hypertension, folic acid supplement, iron supplement, multi-micronutrient use, gender, and gestational age (in weeks).
For gestational age, model 2 was adjusted for residence, maternal age, maternal education, nulliparity, Kessner index, household wealth index, smoking, pregnancy-induced hypertension, folic acid supplement, iron supplement, multi-micronutrient use, and gender.
For small for gestational age, model 2 was adjusted for residence, maternal age, maternal education, nulliparity, Kessner index, household wealth index, smoking, pregnancy-induced hypertension, folic acid supplement, iron supplement, and multi-micronutrient use.
P trend across altitudes was evaluated using the median of each altitude group as a continuous variable in each adjusted regression model.
As presented in Fig. 3, dose–response relationships between residential altitude and birth weight, gestational age, and SGA were performed, respectively, using RCS functions. In Fig. 3a, there was an inversely linear relationship between residential altitude and birth weight (P for overall association < 0.001 and P for nonlinear association = 0.312). However, a nonlinear relationship was observed between residential altitude and gestational age in Fig. 3b (P for overall association < 0.001 and P for nonlinear association = 0.010). In Fig. 3c, there was a positive linear relationship between residential altitude and SGA (P for overall association < 0.001 and P for nonlinear association = 0.194). The curve of the dose–response relationship between altitude and birth outcomes suggested that the risk of reduced birth weight and increased SGA would be elevated significantly to some extent when the altitude was approximately more than 700 m. Although the increased gestational age was found statistically when the altitude was more than 700 m, such very small increment should be intercepted cautiously in clinical practice.

Fig. 3. Dose–response relationships between residential altitudes (in m) and birth weight, gestational age, and small for gestational age. (a) Association between birth weight and altitude using RCS with three knots. (b) Association between gestational age and altitude using RCS with three knots. (c) Association between small for gestational age and altitude using RCS with three knots. For birth weight, restricted cubic spline functions were used after adjusting for residence, maternal age, maternal education, nulliparity, Kessner index, household wealth index, smoking, pregnancy-induced hypertension, folic acid supplement, iron supplement, multi-micronutrient use, gender, and gestational age (in weeks). For gestational age, restricted cubic spline functions were used after adjusting for residence, maternal age, maternal education, nulliparity, Kessner index, household wealth index, smoking, pregnancy-induced hypertension, folic acid supplement, iron supplement, multi-micronutrient use, and gender. For small for gestational age, restricted cubic spline functions were used after adjusting for residence, maternal age, maternal education, nulliparity, Kessner index, household wealth index, smoking, pregnancy-induced hypertension, folic acid supplement, iron supplement, and multi-micronutrient use. Restricted cubic spline function with three knots located at the 5th, 50th, and 95th percentiles of the altitude distribution was used while setting the median as the reference value. Dashed lines represent the 95% CIs, and knots were represented by dots. The horizontal dashed green line represents that the Y-coordinate of the line was 0 when a linear regression was requested or 1 when a logistic model was requested.
Subgroup analysis
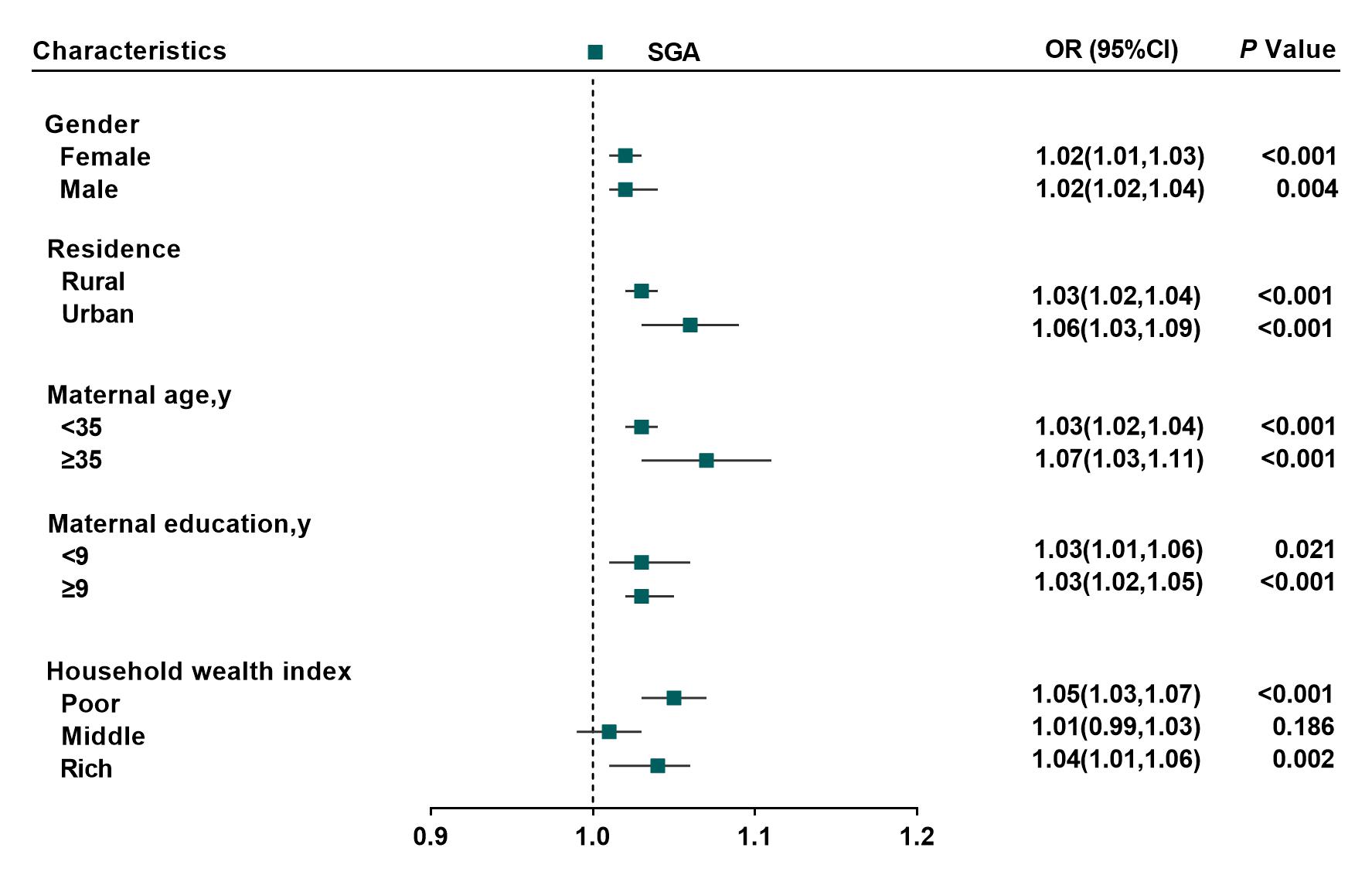
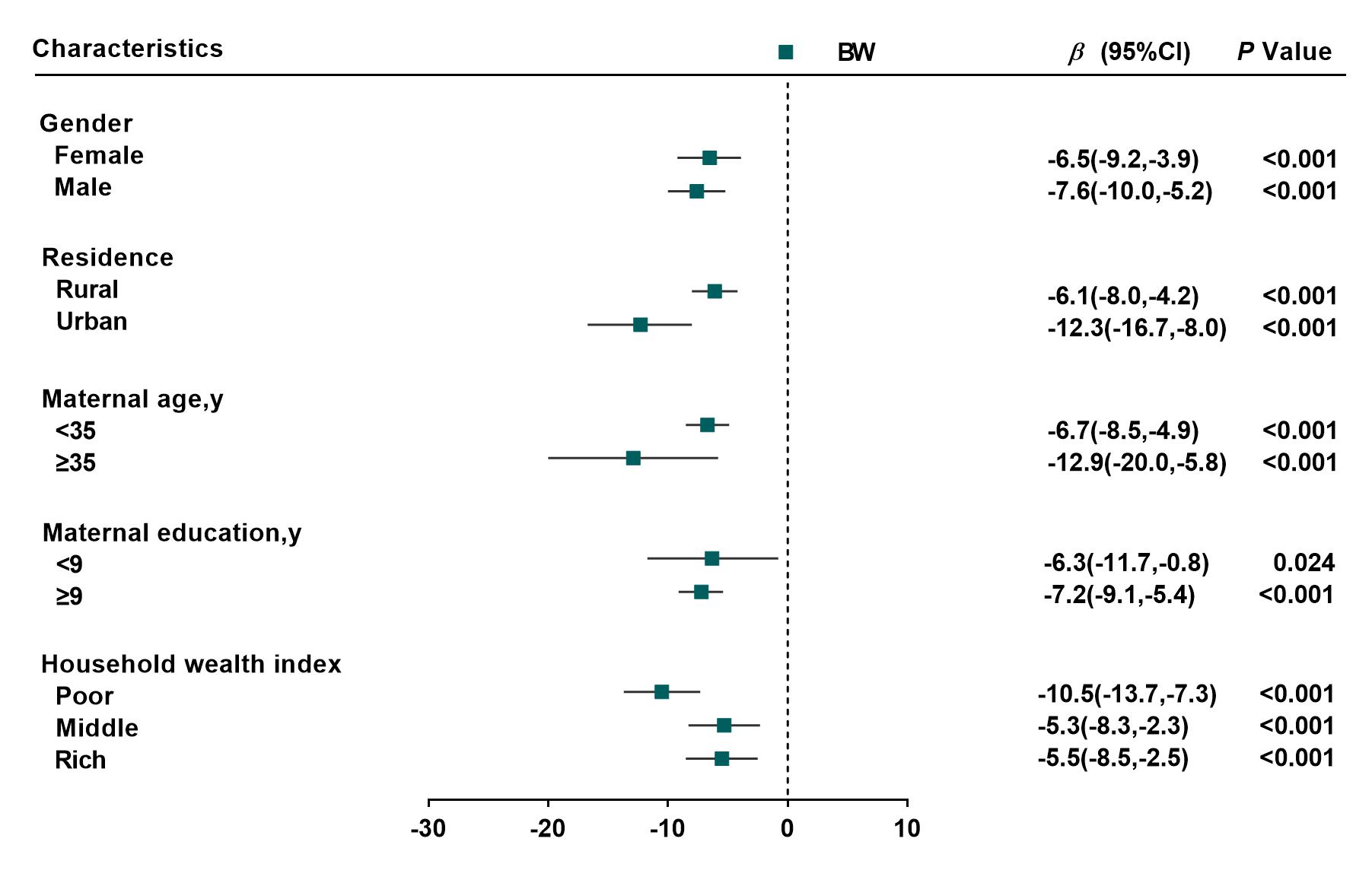
Consistent with main analysis above, the subgroup analysis also indicated the robust of the association between altitude and birth outcomes, regardless of gender, residence, maternal age, maternal educational status, or household wealth index (Supplementary Fig. S1a–c).
Discussion
The present study suggested that the increasing altitude was associated with reduced birth weight, a slight increased gestational age, and an increased risk of SGA birth in the region with low-to-medium altitude of China. Compared with those born to mothers living at an altitude <500 m, the birth weight of newborns at an altitude of 1000–1538 m was reduced by 50.7 g, and gestational age was increased slightly by 0.083 week. Also there were 10%–28% increased risk of SGA birth from 500 to 1538 m compared with an altitude <500 m. A significant dose–response relationship between altitude and birth weight and SGA was observed.
Currently published studies mainly focused on two different altitude levels as high altitude levels (2000–4500 m) and low-to-medium altitude (<2000 m). Reference Jensen and Moore8,Reference Yip9 And the research results showed that high altitude acted independently from other factors to reduce birth weight. Literature reports showed that birth weight decreased an average of 102 g per 1000-m elevation when confounding factors were considered. Reference Jensen and Moore8 A quasi-experiment indicted that every 1000-m increase in maternal altitude exposure was associated with a 75.9 g reduction in birth weight. Reference Zahran, Breunig, Link, Snodgrass and Weiler11 Altitude ranges from 2000 to 4500 m, and birth weight declined at an average of 65 g for every additional 500-m altitude. Reference Mortola, Frappell, Aguero and Armstrong32 In summary, studies reported birth weight decreased 50–200 g with 1000-m altitude increases above 1000 or 2000 m. Reference Jensen and Moore8,Reference Yip9,Reference Zahran, Breunig, Link, Snodgrass and Weiler11,Reference Mortola, Frappell, Aguero and Armstrong32,Reference Waldhoer and Klebermass-Schrehof33 Although our study was conducted in the region with low-to-medium altitude, we still observed that average birth weight decreased by 6.4 g with every 100-m increase in altitude, which was comparable to those previous literature estimates. Additionally, our results suggested that the risk of SGA increased by 3% for every 100-m increase in altitude, and the risk of SGA increased by 10% and 28% at altitudes above 500–900 and 1000–1538 m compared with less than 500 m. This increasing was in correspondence with prior studies suggesting this risk. Reference Levine, Gonzales and Tapia13,Reference Gonzales, Steenland and Tapia34 Moreover, our study also found obvious dose–response relationship between low-to-medium altitude and birth weight and SGA, which implied that the altitude of approximately more than 700 m could result in a significant adverse effect on Chinese newborns. It was noteworthy that a 0.015-week increment in gestational age with a 100-m increase in altitude was found in the present study. Previous one study suggested that gestational age was higher for newborns of mothers with Aymará genetic background in lowland due to genetic adaptation to altitude. Reference Rothhammer, Fuentes-Guajardo, Chakraborty, Lorenzo Bermejo and Dittmar35 Another study reported that gestational age at delivery at moderately high-altitude Denver (39.3 ± 0.4) was slightly higher than sea level Milan (39.2 ± 0.1), but the difference was not statistically significant for only 94 sample size. Reference Galan, Rigano and Radaelli36 However, there were some other studies which found the inverse association between altitude and gestational age. Reference Keyes, Armaza, Niermeyer, Vargas, Young and Moore37,Reference Ali Kamal38 Such slight increment of gestational age found in present study might be resulted from lager sample size, so it should be interpreted cautiously in clinical practice. Therefore, further investigation will be needed to verify the association between altitude and gestational age at low-to-medium altitude.
Adverse birth outcome was a major problem affecting maternal and child health. In addition to sociodemographic and pathophysiological factors, environmental factors should also be concerned and the altitude might be one of them. Our study found that low-to-medium altitudes were still a possible independent environmental factor affecting inversely birth outcomes. The implication was that even minor alteration in altitude might influence the birth outcomes. As the majority of the population was living at lower range altitudes, our findings might have important generalization significance, and the negative effect of altitude on birth outcomes should be paid more attention no matter what altitude women and children lived at. In view of public health, we suggested that altitude should be considered in the management of maternal and child health care even in the region with low-to-medium altitude.
The altitude-associated decrease in birth weight had been reported. However, the mechanism by which altitude retards fetal growth was not comprehensively understood. There were two plausibly biological explanations underlying the birth weight and altitude, the hypoxia pathway and glucose pathway. The first hypothesis was the inability of the maternal oxygen transport system to meet the increased demands of the intrauterine fetus at higher altitudes. Reference Moore39,Reference Julian, Galan and Wilson40 Nevertheless, this hypoxia pathway was challenged by adequate oxygen delivery to the uterus obtained by hematologic and metabolic adjustments. Reference Postigo, Heredia and Illsley41,Reference Zamudio, Torricos and Fik42 The second biological mechanism was the glucose pathway. In high-altitude area, lower glucose concentrations in the umbilical veins and arteries result in lower fetal glucose delivery and consumption. Anaerobic consumption of glucose by the placenta seemed to reduce the availability of glucose to the fetus. Therefore, hypoglycemia might explain why babies born at high altitudes were lower. Besides, a slight increase of gestational age as the altitude increase in the present study might ascribe to genetic adaptation to altitude. Reference Rothhammer, Fuentes-Guajardo, Chakraborty, Lorenzo Bermejo and Dittmar35,Reference Pizarro-Ortiz, Barra, Gajardo, Fuentes-Guajardo and Rothhammer43 The mechanism of the association between low-to-medium altitude and birth outcomes needed to further be elucidated in future research.
The main strength of our study was that this was a large population-based epidemiological study whose sample size accounting for approximately 9% of the newborn in Shaanxi province of China, and the results could be generalized to the overall province to some extent. Besides, the birth weight in our study collected from Medical Certificate of Birth, nearest to 10 g, which was relatively objective and accurate. Moreover, we further assessed accurately the dose–response relationship using RCSs between altitude and birth outcomes. However, some limitations should be addressed. First, as this study was observational, women’s characteristics were retrospectively self-reported by the mothers after delivery. Although events during pregnancy might be recalled well years later from previous studies, Reference Kvalvik, Nilsen and Skjaerven44 the recall bias could not be eliminated completely. Therefore, effective efforts were conducted to help participants recall accurately as much as possible to control the recall bias by using standard and detailed classification questionnaires with rigorously trained and professional interviewers. Second, there were some potential factors in this observational study confounding the association between altitude and birth outcomes. They should be adjusted in the model analysis accordingly. We selected some factors as potential confounders based on a comprehensive consideration of previous literature and significant differences across altitude levels in our sample including demographic and socioeconomic status, healthcare characteristics, maternal health, and dietary nutrition during pregnancy. Reference Zeng, Cheng and Dang5,Reference Levine, Gonzales and Tapia13,Reference Huang, Wu, Zhao, Hu, Yang and Chen24–Reference Kang, Dang and Zeng28 Even though we adjusted for as many confounders as possible to reduce bias, we cannot rule out effects of all unobserved biases. Third, the observational study cannot demonstrate causality, and consequently, the results should be interpreted cautiously. Future research with favorable study design, therefore, was needed to validate the present study.
Conclusions
The present study suggests that the risk of adverse birth outcomes is increased with increasing altitude even in the areas with low-to-medium altitude. Therefore, the effect of low-to-medium altitude on birth outcomes might warrant consideration from the view of maternal and child health care.
Supplementary materials
For supplementary material for this article, please visit https://doi.org/10.1017/S204017442000063X.
Acknowledgments
We are grateful to the many individuals and organizations that have contributed to this effort, including all the women and their newborn who participated in the survey. We specifically acknowledge the support of local government, the local education bureau, and the dedication and hard work of the field team and data manager in the Department of Epidemiology and Biostatistics, School of Public Health, Xi’an Jiaotong University Health Science Center.
Financial support
This work was supported by National Natural Science Foundation of China (Yan, grant number 81230016), Shaanxi Health and Family Planning Commission (Dang, grant number sxwsjswzfcght2016-013), and National Key R&D Program of China (Yan, grant numbers 2017YFC0907200 and 2017YFC0907201).
Conflicts of interest
The authors declare no conflict of interest.
Ethical standards
The study complied with the Declaration of Helsinki and was approved by the Ethical Committee of Health Science Center, Xi’an Jiaotong University (No. 20120008). The written informed consent obtained from all participants prior to their enrollment.