


Aboriginal and Torres Strait Islander People
A brief history
Australia’s First Peoples, known as the Aboriginal and Torres Strait Islander People (herein respectfully referred to as ‘Aboriginal Australians’ with acknowledgement of the vast cultural diversity that exists within this population), have inhabited the Australian continent for around 65,000 years, where they lived as semi-nomadic hunter-gatherers.Reference Malaspinas, Westaway and Muller 1 , Reference Clarkson, Jacobs and Marwick 2 Since British colonization in 1788, Aboriginal Australians have been marginalized in all aspects of life. Among many other wrong-doings, Aboriginal families have been Systematically excluded from the positive health and education transitions that occurred as a result of primary civic infrastructure, introduction of welfare and shifts in policy. This is known as structural violence and was mediated through legislations such as the 1893 Amendments to the Elementary Education Act, the 1886 Aborigines Protection Act and the 1886 Half-Caste Act, which separated the education of Aboriginal children from mainstream education and allowed for the forcible removal of Aboriginal children of ‘racial mix’ from their families. 3 The process of removing ‘mixed race’ Aboriginal children from their families and into the care of Church missions and white Australian families continued until as recently as the 1970s. These children are known as the Stolen Generations.
The negative impacts of colonization, structural violence and the Stolen Generations on Aboriginal health and wellbeing are very much evident in today’s society. 3 Historical trauma permeates the Aboriginal experience and is evident in the inherent mistrust of Western policies and people perceived to be in a position of power, such as doctors. Although concerted efforts have been made to address the disadvantage experienced by Aboriginal people, much remains to be done.
Current demographics
According to the 2011 National Census, there are approximately 670,000 people in Australia who identify as being of Aboriginal or Torres Strait Islander descent, representing 3% of the Australian population. 4 The majority of Aboriginal people live in urban and regional East Coast towns and cities, but there are also significant proportions (22%) living in remote and very remote regions compared to non-Aboriginal Australians (2%) (Fig. 1), where remoteness is a measure of relative access to services according to the accessibility and remoteness index of Australia (ARIA). 5 This is important because Aboriginal Australians living an urban, mainstream lifestyle have far better health and social outcomes than those in rural and remote regions. 6 The average life-expectancy of an Aboriginal person is 10 years less than that of a non-Aboriginal person, and in some regions, children and adolescents represent almost 50% of the Aboriginal population. 6 , 7 This results in a demographic where there is a high proportion of children and adolescents and comparatively few adults and elders to support, nurture and guide this younger generation.

Fig. 1 Distribution of Australia’s population by remoteness and Indigenous status. (Colour Online) A high proportion of Aboriginal Australians live in remote (8%) and very remote (14%) regions of Australia compared to non-Aboriginal Australians, who live mostly in major cities and inner regional areas, with only 2% living in remote or very remote regions. Reprinted from: SCRGSP. Overcoming Indigenous Disadvantage: Key Indicators 2014. Canberra: Productivity Commission; 2014: p8.
Despite living in a developed high-income country, Aboriginal Australians arguably experience rates of socioeconomic and health disadvantage similar to that seen in developing countries. Compared to non-Aboriginal Australians, they have significantly higher rates of disease and hospitalization,Reference Zhao, You, Wright, Guthridge and Lee 8 and are more likely to be less educated,Reference Anderson, Robson and Connolly 9 unemployed, 10 incarcerated 11 or victims of domestic violence. 12 Aboriginal mothers have a higher prevalence of smoking and alcohol consumption during pregnancy, malnutrition and poor food security, psychological stress, teenage pregnancy and multi-parity, compounded by inadequate access to antenatal care. This results in excessive rates of low birth weight (LBW), prematurity and perinatal and infant mortality.Reference Panaretto, Lee and Mitchell 13 – Reference McEwen, Guthridge, He, McKenzie, Boulton and Smith 15 Sadly, these patterns of health, social and economic disadvantage are characteristic of many minority and Indigenous populations around the world.Reference Anderson, Robson and Connolly 9 , Reference Shah, Zao, Al-Wassia and Shah 16 Given these similarities, the findings from this review are relevant not only to Aboriginal Australians but also to many other minority populations who live in high-income countries and experience disproportionate socioeconomic and health disadvantage.
Closing the Gap
In 2008, Australia’s Prime Minister made a formal apology to the Aboriginal People for the ‘profound grief, suffering and loss’ caused by colonization and for the wrong-doings of past governments, especially in respect to the Stolen Generations. A commitment was made to reduce Indigenous disadvantage by Closing the Gap. 17 To guide and monitor the progress of the Closing the Gap Policy, the Council of Australian Governments (COAG) agreed to six measurable targets to be reported on biennially: 5
∙ Life expectancy
∙ Early childhood mortality
∙ Early childhood education
∙ Reading, writing and numeracy
∙ High school completion
∙ Employment
Apparent improvements have been reported in terms of life expectancy, childhood mortality and high school completion. Although this represents a step in the right direction, overall improvements may not reflect the status of rural and remote Aboriginal communities, especially those in Central and Northern Australia. According to Boulton in Aboriginal Children, Health and History: Beyond Social Determinants: ‘The divergence of health and wellbeing between the two demographics [urban and rural] accounts for the paradox of an improvement in selected measures of health and wellbeing at a national level, yet the opposite in remote districts.’ 3 Furthermore, no progress has been made towards Closing The Gap in early childhood education and proficiency in reading, writing and numeracy. 5 Currently, education and community services do not meet the needs of these Aboriginal children and adolescents – many are disengaged with the schooling system and many in rural and remote locations have low literacy levels. 18 , 19 This is concerning, as early life development and academic engagement are important determinants of human capital.Reference Janus and Duku 20 , Reference Sum, Khatiwada, McLaughlin and Palma 21
A better understanding of the determinants of perinatal health, childhood development and education outcomes in the Aboriginal population could potentially guide policies towards achieving the critical targets set out by COAGs. Given the excessive rates of LBWs and prematurity, there may be a role for the DOHaD hypothesis in developing an understanding of the perpetuation and intergenerational transmission of disadvantage.
The Developmental Origins of Health and Disease
The DOHaD hypothesis advocates that a sub-optimal intrauterine environment during critical periods of foetal development has the potential to alter the risk of non-communicable disease in the offspring.Reference Gluckman, Hanson and Buklijas 22 While the DOHaD field had focused predominantly on the risk of chronic cardiovascular and metabolic disease in adulthood, there is increasing evidence from epidemiological and clinical studies that subtle changes in birth weight (BW) and foetal growth also have implications throughout childhood and adolescence in terms of physical and mental health, neurocognitive and behavioural outcomes during infancy, childhood and adolescence.
The thrifty phenotype hypothesis, proposed by Barker and Hale in 1992, suggests that a foetus is able to adapt to the stress of nutrient and oxygen deprivation in utero by epigenetically altering its phenotype to conserve, or become thrifty, with the available nutrients.Reference Wadhwa, Buss, Entringer and Swanson 23 In addition to conferring immediate benefit to the foetus, these epigenetic changes also result in predictive adaptive responses that provide a fitness advantage in stressful and nutrient-poor extra-uterine environments.Reference Hales and Barker 24 However, when there is a mismatch between the predicted and actual environment these changes become maladaptive in the offspring. This process is outlined in Fig. 2.
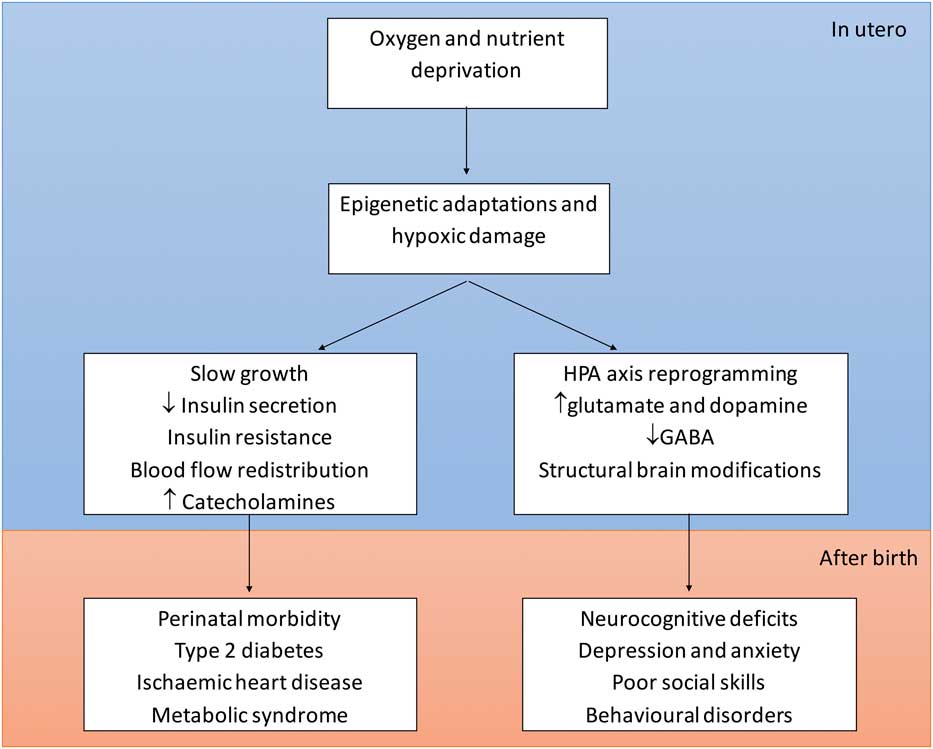
Fig. 2 The Developmental Origins of Health and Disease. (Colour Online) Oxygen and nutrient deprivation in utero are thought to cause a number of epigenetic and hypoxic changes, which alter the regulation of foetal metabolic and hormonal pathways, and brain development. These alterations predispose the offspring to a spectrum of adverse outcomes in both the short- and long-term.
Perhaps to its detriment the DOHaD hypothesis is often understood and investigated using a model of LBW or growth restriction and indeed this is where most of the evidence exists. This tends to bias the model towards one of teratogenicity, although the effects of developmental programming likely extend across the entire range of BW.Reference Gluckman, Hanson and Buklijas 22 Current research describes a continuous relationship between both birth weight percentile (BWP) and perinatal mortality, and BWP and childhood education, with optimum outcomes occurring consistently above the 50th percentile – risk was not confined to the extremes of BW.Reference McEwen, Guthridge, He, McKenzie, Boulton and Smith 15 , Reference Francis, Permezel and Davey 25 , Reference Vasak, Koenen and Koster 26 The mechanism of this association in foetuses without growth restriction has not been elucidated. However, these studies support the hypothesis that DOHaD is a manifestation of a normal process, whereby a foetus is able to draw information from its environment and, through epigenetic mechanisms, adjust its developmental trajectory to suit the environment into which it is predicted to be born.
The DOHaD hypothesis is potentially very important in explaining disease and disadvantage in Aboriginal Australians. The babies of Aboriginal mothers face many intrauterine stressors as the result of poor foetal growth, maternal malnutrition and poor food security (particularly for those living in remote locations), maternal psychological stress (especially in teenage mothers), smoking and alcohol use during pregnancy. These stressors result in epigenetic changes that are argued to predispose to poor physical and neurocognitive health in the offspring and so maternal disadvantage is potentially passed on to the next generation through a sub-optimal intrauterine environment.
BW and foetal growth
BW, as a putative indicator of the quality of the intrauterine environment, is a strong and independent predictor of both immediate and future health and developmental outcomes (Fig. 3). Foetuses with a predicted BW below the 10th percentile of the population distribution for gestational age (small for gestational age, SGA) have traditionally been the clinical focus for increased surveillance and obstetric intervention, with strong evidence to support this centile as posing the greatest risk of perinatal and life-long complications.Reference Vashevnik, Walker and Permezel 27 – 30 However, the vast majority of BWs fall between the 10th and 90th percentiles and small variation, particularly in long-term outcomes within this large grouping, is argued to be more important on a population level than larger variations in babies born <10th percentile.Reference Raznahan, Greenstein, Lee, Clasen and Giedd 31 , Reference Matte, Bresnahan, Begg and Susser 32

Fig. 3 The long-term metabolic, neurocognitive and developmental problems associated with intrauterine growth restriction. (Colour Online) Being born small predisposes to a myriad of outcomes that have the potential to adversely affect the offspring throughout its entire life-course. IQ: intelligence quotient. IHD: ischaemic heart disease. DMT2: type 2 diabetes mellitus. HTN: hypertension.
The ‘gap’ in BW distribution
In 2012, the mean BW in Australia for live-born, non-Aboriginal singletons was 3373 g. This was 162 g heavier than the mean BW of 3211 g in Aboriginal singletons.Reference Hilder, Zhichao, Parker, Jahan and Chambers 14 Similar figures were reported in a nationwide study in 1999,Reference Roberts and Lancaster 33 suggesting that the gap in BW distribution is not closing. Aboriginal babies are also twice as likely to be born under 2500 g compared to the Australian average (12% v. 6%, Fig. 4).Reference Hilder, Zhichao, Parker, Jahan and Chambers 14 In fact the entire distribution of BWs is shifted towards lower values in Aboriginal babies, with a significantly greater proportion born under the 50th percentile of BW for gestational age compared to non-Aboriginal babies.Reference McEwen, Guthridge, He, McKenzie, Boulton and Smith 15

Fig. 4 Distribution of birth weights in the total Australian population and the Aboriginal population. (Colour Online) 6% of the Australian population is born with a BW under 2500 g compared to 12% of the Aboriginal population. Adapted from: Hilder L, Zhichao Z, Parker M, Jahan S, Chambers GM. Australia’s mothers and babies 2012. Perinatal statistics series no 30. Canberra: AIHW; 2014.
Aboriginal and non-Aboriginal foetuses exhibit similar growth patterns until the 34th week of gestation, at which point a significant discrepancy in foetal growth and BW appears and continues to widen to produce an eventual disparity of up to 200 g in full-term foetuses.Reference Coory 34 Current evidence strongly suggests that this disparity is attributable to poverty, racism and both proximal and transgenerational environmental influences, such as malnutrition which limit growth towards the end of pregnancy when the nutritional demands of the foetus are greatest.Reference Jasienska 35
Although maternal Aboriginal status has a clear association with LBW (defined as BW <2500 g),Reference Hilder, Zhichao, Parker, Jahan and Chambers 14 , Reference Mohsin, Wong, Bauman and Bai 36 the observed association is likely to be explained largely by the high prevalence of other risk factors in Aboriginal mothers and indeed by intergenerational malnutrition.Reference Kramer, Ananth, Platt and Joseph 37 From an intergenerational perspective, Currie and Moretti found that women who were born LBW were 50% more likely to have a LBW baby.Reference Currie and Moretti 38 This intergenerational transmission of LBW was shown to be more profound in women from poorer socioeconomic and educational backgrounds, which is important in understanding the potential role of BW in the transgenerational perpetuation of disadvantage, particularly in populations with high rates of impaired foetal growth, such as Aboriginal Australians.
Health during the perinatal period
The reduction of perinatal, infant and early childhood mortality are key health goals for the United Nations, World Health Organisation and the COAGs as one of the major targets for reducing poverty and disadvantage worldwide. 5 , 39 , 40 Health during the perinatal period is a predictor of life-long health and wellbeing. Poor health during the perinatal period is one of the earliest tangible manifestation of the detrimental effects of DOHaD in Aboriginal Australians. Understanding the role of foetal growth (as a proxy for the quality of the intrauterine environment) as a determinant of perinatal health is an important step towards halting the seemingly self-perpetuating cycle of disadvantage.
Defining perinatal outcomes
The definition of perinatal mortality varies between countries. The definition provided by the Australian Bureau of Statistics and the National Perinatal Data Collection defines perinatal death as a stillbirth or neonatal death where:
∙ Stillbirth is the birth of a foetus without signs of life, where the foetus weighs at least 400 g or has a gestational age of at least 20 weeks.
∙ Neonatal death is the death of any live-born foetus within 28 days of birth.Reference Hilder, Zhichao, Parker, Jahan and Chambers 14
In 2012, Australia’s perinatal mortality rate (PMR) was 9.6.Reference Hilder, Zhichao, Parker, Jahan and Chambers 14 The Aboriginal PMR was 15 and an Aboriginal pregnancy was almost 60% more likely to end in perinatal death than a non-Aboriginal pregnancy.Reference Hilder, Zhichao, Parker, Jahan and Chambers 14 Although worrying, this figure represents progress towards Closing the Gap, with a 32% decrease in Aboriginal stillbirths since 1995.Reference Ibiebele, Coory, Boyle, Humphrey, Vlack and Flenady 41 However, this apparent decrease is likely to be at least partly mediated by secular changes in Aboriginal identification and the disproportionate increase in urban Aboriginal populations compared to rural and remote populations. 3
BW and perinatal mortality
The aetiology of perinatal mortality is complex. There is evidence that many known risk factors mediate their effect either through a reduction in the rate of foetal growth, and hence BWP, or by a reduction in the duration of gestation, rather than by independent mechanisms.Reference Coory 34 , Reference Mohsin, Bauman and Jalaludin 42 BW is the single most important risk factor for perinatal mortality and it is argued that a reduction in stillbirths and neonatal deaths hinges on the improved prediction and prevention of LBW and SGA babies.Reference Mohsin, Bauman and Jalaludin 42 – Reference Kliewer and Stanley 44 There is a proportion of SGA infants that are considered constitutionally small, with the assumption that these infants are free from pathology.Reference Groom, Poppe, North and McCowan 45 However, because constitutional smallness is often defined using maternal characteristics, it does not account for the transgenerational nature of malnutrition and poverty. In addition, recent evidence suggests that the association between foetal growth and perinatal mortality is present across the entire spectrum of BWPs and not confined to pathologically growth restricted infants.Reference McEwen, Guthridge, He, McKenzie, Boulton and Smith 15 , Reference Francis, Permezel and Davey 25 , Reference Vasak, Koenen and Koster 26
A recent study in the Northern Territory (NT), Australia, examined the association between BWP as a continuous variable and perinatal mortality.Reference McEwen, Guthridge, He, McKenzie, Boulton and Smith 15 The authors demonstrated that although foetuses with BWs <10th percentile for gestational age had greatly increased odds of perinatal mortality, the increased risk extended well beyond this arbitrary cut-off. A curvilinear association was observed between BWP and perinatal death (P=0.000), with the lowest mortality rates at the 78th percentile in non-Aboriginal infants and the 61st percentile in Aboriginal infants. The study controlled for a number of perinatal and sociodemographic variables. A similar association was observed in both Aboriginal and non-Aboriginal Australians in a study by Kliewer in 1993.Reference Kliewer and Stanley 44
A recent study of a large Victorian cohort showed that for term births, optimal perinatal outcomes occurred in those foetuses born between the 50th and 90th percentiles of BW.Reference Francis, Permezel and Davey 25 Infants born below the 50th BWP were at significantly increased risk of perinatal death compared to those born above the 50th BWP [adjusted odds ratio (aOR) 2.10 and 1.58 for 10–25th and 25–50th centile; both P<0.0001]. These findings have been reproduced in Dutch cohort by Vasak (2015) and in a Scottish cohort by Moraitis (2014).Reference Vasak, Koenen and Koster 26 , Reference Moraitis, Wood, Fleming and Smith 46 Moraitis demonstrated that one in three stillbirths were associated with being born outside the 21–80th percentiles. It was proposed that the larger babies reflected better placental function, and conversely that a degree of placental insufficiency was present in foetuses born below the optimal range of BWP.Reference Francis, Permezel and Davey 25 Increasing BWP, up to the 90th percentile, has been shown to be associated with improved placental blood flow and reduced incidence of foetal hypoxia, which may explain improved perinatal survival with increasing BWPs.Reference Morales-Roselló, Khalil, Morlando, Papageorghiou, Bhide and Thilaganathan 47 BWs above the 97th percentile were associated with increased risk of perinatal death (compared to the referent) in all of the above studies, which assumedly reflects the prevalence of maternal obesity, diabetes and birth trauma in this category.
The ‘gap’ in perinatal outcomes
In spite of higher mortality rates for Aboriginal babies overall,Reference Ibiebele, Coory, Boyle, Humphrey, Vlack and Flenady 41 preterm Aboriginal babies experience similar survival to non-Aboriginal preterm babies.Reference Coory 34 , Reference Mohsin, Bauman and Jalaludin 42 , Reference Ruan, Abdel-Latif and Bajuk 48 In fact, there is no statistical difference in average BWP or PMR between Aboriginal and non-Aboriginal infants born between 22 and 31 completed week of gestation.Reference Ruan, Abdel-Latif and Bajuk 48 In contrast, full-term Aboriginal neonates experience significantly worse outcomes than their non-Aboriginal counterparts [adj. relative risk 2.9, 95% confidence interval (CI) 1.5–5.5].Reference Coory 34 This cross-over phenomenon, which is not well-understood, is seen in disadvantaged populations in developed countries around the world.Reference Alexander, Tompkins, Altekruse and Hornung 49 – Reference Thomson 51 If gestational age is assumed to be reasonably accurate, the increasing gap in perinatal mortality associated with term pregnancies could be explained by prolonged exposure to unfavourable intrauterine conditions and environmental insults during pregnancy, such as smoking, alcohol, psychological stress and malnutrition with longer gestations.Reference Kliewer and Stanley 44 Alternatively, failure of the Aboriginal foetus to gain as much weight during the final 5–6 weeks of pregnancy as non-Aboriginal foetuses, as a result of placental insufficiency and aging, may reduce their ability to survive the neonatal period.Reference Roberts and Lancaster 33 , Reference Coory 34 , Reference Kramer, Ananth, Platt and Joseph 37 , Reference Maiti, Sultana and Aitken 52
There is overwhelming evidence that Indigenous status itself is not an independent risk factor for adverse perinatal outcomes.Reference Coory 34 , Reference Mohsin, Bauman and Jalaludin 42 , Reference Ruan, Abdel-Latif and Bajuk 48 Mohsin (2006) demonstrated that after controlling for socioeconomic and perinatal confounders, the odds of perinatal mortality in Aboriginal babies were not higher than in non-Aboriginal babies (1.05, 95% CI 0.83–1.33).Reference Mohsin, Bauman and Jalaludin 42 This supports the notion that targeted interventions aimed at increasing foetal growth, such as better antenatal attendance, reduced smoking and improved maternal nutrition, has the potential to reduce Aboriginal perinatal mortality and help to break the cycle of disadvantage.
Early childhood development
Childhood development is a holistic concept, encompassing everything from physical wellbeing, to prosocial behaviour, emotional health, cognitive abilities, attention and visuospatial functioning.Reference Janus and Duku 20 , Reference Janus and Offord 53 , Reference Janus and Offord 54 Adequate development of these abilities during the first 5 years of life is essential, 5 and failure to do so strongly influences a child’s capacity to learn on commencing school, and impacts on educational attainment and social and emotional skills throughout life, 19 potentially resulting in life-long disadvantage. With almost 50% of Aboriginal children in Australia classed as developmentally vulnerable and inadequately prepared for school, 55 it is unsurprising that the Australian Government has identified early childhood development as one of the fundamental targets in reducing Aboriginal disadvantage. 5
The environment that shapes early life development is composed of complex interactions between biological factors, family dynamics, immediate neighbourhood characteristics and the socioeconomic, political and cultural context in which the child is raised. 19 , Reference Brinkman, Gregory, Harris, Hart, Blackmore and Janus 56 A deeper, population-specific understanding of the relationship between intrauterine growth and early life development could help guide interventions towards improving the development of both Aboriginal and non-Aboriginal Australians. From a biological standpoint, prenatal life represents a critical phase in neurodevelopment and subtle insults during pregnancy have been shown to exert measurable and significant effects on cognitive function,Reference Raznahan, Greenstein, Lee, Clasen and Giedd 31 structure and function of the brain,Reference Raznahan, Greenstein, Lee, Clasen and Giedd 31 , Reference Cordova-Palomera, Fatjo-Vilas and Falcon 57 , Reference Walhovd, Fjell and Brown 58 and function of the hypothalamic–pituitary–adrenal (HPA) axis.Reference Matthews 59 – Reference Simonetta, Rourke, Owens, Robinson and McMillen 61 Intrauterine reprogramming of the foetal HPA-axis in response to stressors during pregnancy has been shown to result in stress, mental illness and behavioural problems in the offspring, and may even contribute to transgenerational poverty and disadvantage.Reference Austin and Brunner 62 Growth restriction, which is both a form of and response to intrauterine stress, may result in a similar pattern of disorder and disadvantage in the offspring, although this causal pathway has not been specifically explored. Neurological manifestations of LBW and growth restriction in animal models include altered neurotransmitter expression, decreased brain cortical surface area and volume and spatial and memory deficits.Reference Hernandez-Andrade, Cortes-Camberos and Diaz 63 – Reference Mallard, Loeliger, Copolov and Rees 66
The literature on the association between BW and early childhood development – social, emotional, behavioural and visual-motor – is vast, but the results are often contradictory and difficult to interpret due to the varying methods of measuring development and the difficulty in isolating the effect of BW from family level and socioeconomic determinants of childhood development. Additionally, research has suggested that the developmental repercussions of BW manifest differently in males and females, underpinning the problematic nature of evaluating studies where males and females have not been analysed separately.Reference Kelly, Nazroo, McMunn, Boreham and Marmot 67 , Reference Costello, Worthman, Erkanli and Angold 68 Despite these limitations, a number of studies have supported the notion that BW is a significant determinant of emotional, social and behavioural development, at least in non-Aboriginal children. Compared to their normal BW peers, LBW children appear to have higher levels of withdrawal, social problems, thought problems, attention problems, delinquent behaviour and aggressive behaviour.Reference Grunau, Whitfield and Fay 69 , Reference Liu, Sun, Neiderhiser, Uchiyama and Okawa 70 They are more likely to display symptoms of attention-deficit hyperactivity disorder (aOR 3.6, CI 1.63–7.95, P=0.002).Reference Heinonen, Raikkonen and Pesonen 71 Interestingly, BW also seems to alter the ability to cope with adversity during childhood, with females exposed to adverse childhood experiences being more likely to develop depression if they were also born LBW.Reference Costello, Worthman, Erkanli and Angold 68 This supports the foetal programming hypothesis.
Unfortunately, there is a dearth of literature on the association between perinatal factors and early childhood development in Aboriginal Australians, with only two studies identified. A study from the NT, Australia, explored the perinatal and sociodemographic predictors of early childhood development in a cohort Aboriginal and non-Aboriginal children.Reference Guthridge, Li, Silburn, Li, McKenzie and Lynch 72 Development was measured using results from the Australian Early Development Census (AEDC), which is a validated national survey completed every year by kindergarten teachers on the development of each child (aged 4–6 years) enrolled in their class. Aboriginal children were seven times as likely to be classed as developmentally vulnerable compared to non-Aboriginal children (OR 6.93, 95% CI: 5.62–8.56, P<0.001). After adjustment for perinatal and sociodemographic risk factors, these odds dropped dramatically (aOR 1.68, 95% CI: 1.21–2.32, P<0.01). Factors that were associated with developmental vulnerability included preterm birth, increased parity, male gender, English as a second language, remoteness and lower maternal education. Interestingly, LBW was not found to be a risk factor for developmental vulnerability in either Aboriginal or non-Aboriginal children (aOR 0.72, 95% CI: 0.44–1.19). With under 2000 participants, it is likely that this study was underpowered to detect the effect of BW on early developmental outcomes. Additionally, there was no exploration of the effect of larger BWs, which have been shown in other non-Aboriginal cohorts to be protective against developmental vulnerability.Reference Khambalia, Algert, Bowen, Collie and Roberts 73
A recent study by Hanly et al. examined the association between gestational age and developmental vulnerability in a cohort of Aboriginal and non-Aboriginal children from New South Wales, Australia.Reference Hanly, Falster and Chambers 74 In children born between 27 and 40 weeks’ gestation, each additional week was associated with a decrease in the risk of developmental vulnerability and this association was the same in both Aboriginal and non-Aboriginal children. Given that Aboriginal children were more likely to have been born at or before 38 weeks completed gestation, it is likely that gestational age contributed at least partially the gap in developmental outcomes observed between Aboriginal and non-Aboriginal children. However, the proportion of Aboriginal children who were developmentally vulnerable was higher than non-Aboriginal children at all gestational ages, highlighting the ‘disproportionate burden of disadvantage experienced by Aboriginal children’ in respect to other perinatal and sociodemographic factors.Reference Hanly, Falster and Chambers 74
The above studies highlight not only the importance but also the possibility of optimizing the developmental opportunities of Aboriginal and non-Aboriginal children during their most formative years by reducing the burden of modifiable adversities during the perinatal and early childhood periods. Although factors such as BW and gestational age likely account for only a small amount of variation of childhood development,Reference Sommerfelt, Andersson and Sonnander 75 additional research may more accurately define the degree of influence that various intrauterine stressors have on early childhood development in Aboriginal children. In particular, the potential for measurable intrauterine stressors to program a child’s ability to cope with adversity demands further exploration.
Education
Neurocognitive development is a multi-dimensional concept that encompasses intellectual ability, cognitive functioning and educational achievement.Reference Malacova, Li, Blair, Leonard, de Klerk and Stanley 76 Educational achievement is an important predictor of individual human capital; low performance throughout school, especially in literacy and numeracy, is associated with early school leaving, unemployment, welfare dependency, delinquent behaviour, crime and substance abuse in later life. 19 , Reference Sum, Khatiwada, McLaughlin and Palma 21 On a population level, educational achievement predicts national capital and economic growth.Reference Hanushek and Woessmann 77
In Australia, education outcomes are measured by the National Assessment Program – Literacy and Numeracy (NAPLAN) in year 3, 5, 7 and 9 (i.e. ages 9, 11, 13 and 15). It provides nationally comparable data on student performance across the domains of reading, writing, language conventions and numeracy. In 2017, only 3.1 and 2.7% of all children failed to achieve the national minimum standard (NMS) in year 3 reading and numeracy, respectively. In comparison, 15.7% of Aboriginal students failed to achieve the NMS in reading, and 15.1% did not reach the NMS in numeracy. 18 In the NT, approximately 50% of all Aboriginal students do not achieve the minimum standard required to progress to the next year level without significant difficulty, 18 and this is likely to manifest negatively in later life. These results are concerning, and demand changes to deliver services that increase the educational gains of Aboriginal children, for the sake of individuals, families, communities and the nation as a whole. A more comprehensive understanding of the determinants of educational achievement will be paramount to achieving this goal with the hope of Closing the Gap in education (Table 1). In particular, recent research suggests a possible role for sub-optimal foetal growth in perpetuating disadvantage.
Table 1 Determinants of education and cognition

A large Australian data-linkage study with 9 years of follow-up data explored the association between BWP and subsequent educational outcomes using NAPLAN results at age 8–9 in Aboriginal and non-Aboriginal children in the NT.Reference McEwen, Guthridge, He, McKenzie, Boulton and Smith 15 The study controlled for multiple perinatal and socioeconomic confounders including birth complications, maternal age and education level, socioeconomic status (SES), geographic remoteness, smoking and alcohol use in pregnancy. The study found that BWP in Aboriginal children was linearly associated with scores in reading (P<0.05) and numeracy (P<0.001) (Fig. 5). Optimal education outcomes were associated with BWs between the 50 and 97th percentiles, but unfortunately only 27% of Aboriginal children in the cohort had BWs that fell within these limits. This suggests that a substantial proportion of Aboriginal children are at risk of worse education outcomes due to sub-optimal BW.

Fig. 5 The relationship between birth weight (BW) and reading and numeracy scores is linear in Aboriginal children and quadratic in non-Aboriginal children. (Colour Online) Mean scores in reading and numeracy were calculated at 10th percentile intervals and overlaid with a line of fit graph for the association between BW percentile and (a) reading and (b) numeracy in Aboriginal and non-Aboriginal children. In non-Aboriginal children, scores were highest between the 69 and 84th percentiles, and in Aboriginal children they were highest between the 93rd and 97th percentiles. From McEwen EC, Guthridge SL, He VY, McKenzie JW, Boulton TJ, Smith R. What birthweight percentile is associated with optimal perinatal mortality and childhood education outcomes? Am J Obstet Gynecol. 2018;218:S712-S724. Reprinted with permission from Elsevier.
Guthridge et al. have also examined the relationship between year 3 NAPLAN results in Aboriginal and non-Aboriginal children and various perinatal and sociodemographic factors.Reference Guthridge, Li, Silburn, Li, McKenzie and Lynch 78 The study found that LBW Aboriginal children had greater odds of scoring below the NMS in numeracy than their normal birth weight counterparts after controlling for potential confounders (aOR 1.48, 95% CI 1.11–1.98). They found no significant association between LBW and NAPLAN outcomes in non-Aboriginal students. In another study of Aboriginal adolescents (mean age 18 years), LBW was associated with slower simple reaction time as measured by the CogState battery.Reference Pearce, Mann, Singh and Sayers 79 Working memory and choice reaction time were not different between LBW and normal BW groups. Interestingly, Aboriginal adolescents living in urban areas had significantly faster simple and choice reaction times than those in remote areas.
In non-Aboriginal children, McEwen et al. described a quadratic relationship between BWP and NAPLAN scores, with both reading and numeracy scores increasing with BWs up to the 64th and 81st percentile, respectively (Fig. 5).Reference McEwen, Guthridge, He, McKenzie, Boulton and Smith 15 Similar results were found by Malacova et al. in non-Aboriginal children in Western Australia.Reference Malacova, Li, Blair, Leonard, de Klerk and Stanley 76 , Reference Malacova, Li, Blair, Mattes, de Klerk and Stanley 80 These studies showed significant correlations between BWP and reading (β=0.24, 95% CI 0.16–0.31), writing (0.24, 95% CI 0.15–0.32) and numeracy (β=0.26, 95% CI 0.20–0.32). The author also described a curvilinear relationship, whereby extremes of BW (>2 s.d. above/below the mean) were associated with decreasing test scores. The above studies all support the existence of an optimum BW for educational achievement that is likely between the 50th and 97th percentiles.
Some authors have refuted the association between BW and education outcomes, or have argued that any observed associations are likely to be mediated by other perinatal complications or socioeconomic risk factors.Reference Low, Galbraith, Muir, Killen, Pater and Karchmar 81 – Reference Keltikangas-Jarvinen, Elovainio, Kivimaki, Raitakari, Viikari and Lehtimaki 85 Indeed confounding does present a major issue in the epidemiological study of DOHaD, particularly because the influences of poverty and transgenerational trauma often permeate the entire life-cycle and influence both BW and education outcomes. Sibling and twin studies (in non-Aboriginal children) have largely addressed these caveats and shown that BW is a significant determinant of education, independent of genetics and socioeconomic factors.Reference Matte, Bresnahan, Begg and Susser 32 , Reference Newcombe, Milne, Caspi, Poulton and Moffitt 86 – Reference Strohmaier, van Dongen and Willemsen 90 Strohmaier et al. found lower BWs to be consistently correlated with lower IQ in both monozygotic (r=0.269) and dizygotic (r=0.204) twins.Reference Strohmaier, van Dongen and Willemsen 90 Matte et al. demonstrated similar associations within same sex siblings with weight discordance (0.5 IQ points for every 100 g BW difference in male sibships).Reference Matte, Bresnahan, Begg and Susser 32 In this study, comparable results were also found when using a cohort containing only one sibling from each sibship and controlling for race, maternal education and age, SES status, and birth order. This suggests that most environmental confounding can be largely eliminated by controlling for these five variables. However, SES is notoriously hard to measure accurately and if a factor cannot be accurately measured then it cannot be adequately controlled for. And so the question remains – to what extent does size at birth mediate the association between socioeconomic disadvantage and academic outcomes, and to what extent does disadvantage confound the observed association between BW and cognitive outcomes.Reference Delisle 91
Issues also arise when looking at education in Aboriginal children from a biological perspective. First, because education is a Western construct. Second, because a child’s engagement with and feelings towards schooling has a major bearing on educational outcomes. 19 This level of engagement is much more difficult to facilitate in children from an Aboriginal background, due to different value systems and an inherent mistrust of Western institutions due to past wrong-doings. It is crucial, from this point of view, that schooling is culturally appropriate to Aboriginal students. For example, the presence of Aboriginal teachers or assistants has been shown to positively affect attendance and academic achievement in Aboriginal students. 92
The adverse effects of LBW are more profound in children from disadvantaged backgrounds
In general, children of parents with higher educational attainments tend be less developmentally vulnerable, have higher IQs and perform better throughout school – possibly because these parents place higher value on education or have higher expectations of their children. Parental education and SES play a particularly important role in the development of LBW babies because both are thought to modulate the relationship between BW and education.Reference Malacova, Li, Blair, Leonard, de Klerk and Stanley 76 , Reference Guthridge, Li, Silburn, Li, McKenzie and Lynch 78 , Reference Chaudhari, Otiv, Khairnar, Pandit, Hoge and Sayyad 93 , Reference Lin, Liu and Chou 94 The theory of ‘socioeconomic buffering’ postulates that the adverse effects associated with LBW are more profound in children from low socioeconomic backgrounds, and that sub-optimal foetal growth (as a surrogate for sub-optimal intrauterine environment) may perpetuate existing disadvantage. A Taiwanese study demonstrated that well-educated parents can offset the adverse effect of LBW on educational outcomes in full term, moderately LBW babies.Reference Lin, Liu and Chou 94 Malacova et al. similarly demonstrated that the association between birth length and numeracy scores was also more profound in the socioeconomically disadvantaged.Reference Malacova, Li, Blair, Leonard, de Klerk and Stanley 76 Thus the disadvantage of being born small is more likely to persist in babies who were born into families of lower SES, emphasizing the importance of early life experience and environment.
Biological basis for neurocognitive dysfunction in LBW children
LBW is linked with reduced brain cortical surface area (CSA),Reference Raznahan, Greenstein, Lee, Clasen and Giedd 31 , Reference Cordova-Palomera, Fatjo-Vilas and Falcon 57 , Reference Radlowski, Conrad and Lezmi 64 , Reference Mallard, Loeliger, Copolov and Rees 66 and it would appear that even subtle changes in intrauterine growth preferentially alter the surface area of the association cortices implicated in higher cognitive functions.Reference Raznahan, Greenstein, Lee, Clasen and Giedd 31 A cohort study, which used high-resolution MRI to investigate CSA in middle-aged twins, has shown that within twin pairs, there was a 7.6 mm2 reduction in CSA for every 1 g disparity in BW.Reference Cordova-Palomera, Fatjo-Vilas and Falcon 57 Animal models have found a number of structural brain changes to be associated with growth restriction, including reduced grey and white matter, reduced white matter development and connectivity, reduced hippocampal volume and neuron density, abnormal dendritic growth and neurotransmitter abnormalities.Reference Hernandez-Andrade, Cortes-Camberos and Diaz 63 – Reference Mallard, Loeliger, Copolov and Rees 66 These changes suggest a possible mechanism for the cognitive, psychiatric and behavioural dysfunction observed in children, adolescents and adults who experienced sub-optimal growth in utero. The results of animal studies need to be extrapolated with caution due to important differences in foetal growth, maternal metabolism and placental function between animals and humans.Reference Gluckman, Hanson and Buklijas 22
A recent genome-wide association study by Okbay et al. identified 74 independent loci which exhibited significant association with educational attainment.Reference Okbay, Beauchamp and Fontana 95 The candidate genes were found to be preferentially expressed in neural tissue, particularly during the prenatal period. The genes identified were those that regulate the growth and morphology of brain regions that are also affected by growth restriction (e.g. hippocampus, dendrites). It is possible that slower growth alters the expression of these genes via epigenetic mechanisms, resulting in morphological brain changes that predispose to academic difficulty throughout childhood and adolescence. Alternatively, these candidate genes could represent a common genetic pathway to both LBW and neurocognitive deficits; in which case BW itself is not a modifiable cause of poor academic performance, but merely a proxy for the underlying genes which predispose to neurocognitive dysfunction.Reference Horikoshi, Beaumont and Day 96
Conclusion
Aboriginal Australians have higher rates of perinatal death and childhood illness compared to non-Aboriginal children. They are more likely to be developmentally vulnerable, and are less likely to achieve the national standards in literacy and numeracy. Although much effort is being put towards closing these gaps, it is clear that more needs to be done. The literature suggests that in Aboriginal Australians, a lower distribution of BW may contribute to the excessive rates of adverse perinatal, developmental and education outcomes observed in this population. This supports the role of the DOHaD hypothesis in explaining the prevailing health and socioeconomic disadvantage faced not only by generations of Aboriginal Australians but also of people of African-American, First Nation and Maori descent. Based on current evidence, BW likely explains only 1% of individual variation in these childhood outcomes; however, some authors argue that from a population health perspective, small variations in the intrauterine environment during healthy pregnancies, rather than obvious insults such as growth restriction or LBW, may have more meaningful implications as they occur more frequently in the population, but are also proven to significantly predict health and neurodevelopmental outcomes. Regardless, the importance of optimizing the intrauterine environment before and during pregnancy, and addressing the modifiable risk factors that contribute to sub-optimal growth of the foetus, should not be overlooked by policy makers in their attempt to Close the Gap in Aboriginal outcomes.
Unfortunately, the paucity of evidence on the developmental origins of health and disease in the Aboriginal population makes it difficult to comprehend the exact nature and depth of this association and therefore to make more detailed recommendations based on it. There are many potential reasons for the current lack of research: first, Aboriginal people comprise only 3% of the Australian population, making it difficult to generate large representative cohorts for research; second, research is ethically more difficult when the implications of misguided or misinterpreted research can have such profoundly negative consequences on a population that is already disadvantaged; and third, the potential importance of DOHaD in explaining the gap in Aboriginal outcomes is not widely appreciated. Current knowledge can be improved by large, population studies in Aboriginal Australians, perhaps including participants across multiple generations. Adequate controlling for environmental confounding will be key, and the continued use of twin and sibling studies to this end will be especially important to furthering current knowledge.
Acknowledgements
None.
Financial support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Conflicts of interest
None.






