


Introduction
Turkey has high rates of both infant mortality and consanguineous marriage. Infant mortality level is recognized as an important development indicator pointing to the quality of health services in a country. For example, infant mortality rate, with its different dimensions, is accepted as an indicator of development by the World Bank’s ‘World Development Report’ and by the Human Development Report published by the United Nations Development Programme (UNDP) (World Bank, 2010; UNDP, 2010). In the same vein, the United Nations Millennium Development Goals adopted a reduction in infant mortality as a priority target for many countries (United Nations, 2009).
For many years Turkey registered high rates of infant mortality relative to its economic status. In the past, while adult mortality rates in Turkey did not differ much from those of other countries of similar socioeconomic status, life expectancy at birth remained low due to high rates of infant mortality. Hence, Gürsoy-Tezcan (Reference Gürsoy-Tezcan1992) coined the term Turkish Puzzle for this contradictory situation. Indeed, Turkey’s infant mortality rate remained high enough to justify this description until the mid-2000s: 163 per thousand live births in the mid-1960s, dropping to 121 per thousand live births in the early 1980s and to 66 per thousand live births in the early 1990s. Starting in the 2000s, infant and under-5 mortality rates started falling even more rapidly. The infant mortality rate, which was 29 per thousand in the mid-2000s, fell even further to 17 per thousand by the end of the decade (Koç et al., Reference Koç, Eryurt, Adalı and Çağatay2010). This remarkable fall was a response to socioeconomic changes and the extensive implementation of maternal and child health programmes from the 1980s. Thus Turkey has made great strides towards solving the Turkish Puzzle. The United Nations Children’s Fund (UNICEF) stated that Turkey had attained the second highest reduction in under-5 mortality rate among all OECD countries (UNICEF, 2009). However, Turkey presently has an infant mortality rate four times greater than that of the European Union, which shows that Turkey still has progress to make on the issue. Figures obtained from the TDHS-2008 show that infant deaths in Turkey totalled 22,000 annually, with 17,000 in the neonatal and 5000 in the post-neonatal period.
Consanguineous marriages are still common in Turkey. According to the findings of the 1968 Survey on Family Structure and Population Problems in Turkey, which presented the first data set for this area, 27% of married women had a consanguineous marriage (Timur, Reference Timur1972). Subsequent demographic surveys carried out every 5 years showed that the ratio of consanguineous marriages stabilized at around 22–24%, resisting further reductions (Koç, Reference Koç2007). According to TDHS-2008, 24% of women were in consanguineous marriages. It also showed that 26% of babies born within the five years preceding the survey were from consanguineous marriages and 68% of these were from first-cousin marriages.
The main objective of this study was to explain the causal effect of consanguineous marriages, particularly those of first degree, on infant mortality while controlling other factors. In addition, the study aimed to explore other factors affecting infant deaths, and inform policy priorities on the basis of the relationship between consanguineous marriages and infant mortality.
Literature review
The majority of studies conducted over the last 10 years that have addressed the relationship between consanguineous marriage and infant mortality using multivariate analysis have found a statistically significant relationship. Bittles and Black (Reference Bittles and Black2010) found that for children born to parents with consanguinity to the first degree, neonatal mortality was higher by 10% and infant mortality by 15%. In their study conducted in Tunisia, Jamai et al. (2007) found that consanguineous marriage was significantly associated with mortality, not only in the neonatal and post-neonatal periods, but throughout childhood. In their study on India, Reddy et al. (Reference Reddy, Reddy and Reddy2007) demonstrated the effect of consanguineous marriage in increasing infant deaths. Benner and Hussain (Reference Benner and Hussain2006) found that in Qatar the incidence of genetic diseases, and consequently infant deaths, among children born to consanguineous marriages was higher than in children born to other parents. In a study in countries where consanguineous marriages are more common, Bittles (Reference Bittles2003, Reference Bittles2008) showed that consanguineous marriage is one of the major variables affecting child health in terms of diseases and mortality. In their study on Muslim population groups in India and Pakistan, Hussain et al. (Reference Hussain, Bittles and Sullivan2001) found that consanguineous marriages increase infant mortality by 22% when other factors were controlled.
In Turkey, on the other hand, studies on the issue are rather few. Ulusoy and Tunçbilek (Reference Ulusoy and Tunçbilek1987), Tunçbilek and Koç (Reference Tunçbilek and Koç1994) and Hancıoğlu and Tunçbilek (Reference Hancıoğlu and Tunçbilek1998) addressed the relationship between consanguineous marriages and infant mortality in a descriptive way and found that consanguineous marriage has the effect of increasing infant deaths. However, given the fact that these were descriptive studies that did not control other factors, the relationship they found could not be described as a causal one. In a study in Acıpayam-Denizli, Keskin et al. (Reference Keskin, Bozkurt and Keskin2011) addressed the relationship between infant deaths, miscarriage and consanguineous marriage, controlling for number of children, woman’s educational status and age at marriage. They found that consanguineous marriage increased infant deaths and miscarriages by 67%. However, the outcomes of this study should be taken with caution as it was limited to one administrative district and based on a small number of observations; the analysis included miscarriages together with infant deaths; consanguineous marriages were taken as a whole, without considering sub-groups (i.e. first degree, second degree, distant relative etc.); and, more importantly, bias was introduced by infants not yet completing their risk of death. Thus, the present study is the first in Turkey to address the causal relationship between consanguineous marriages and infant mortality at the national level.
Methods
Data
Data were from the last four Turkish Demographic and Health Surveys (TDHSs) conducted by the Hacettepe University Institute of Population Studies in 1993, 1998, 2003 and 2008, unlike earlier studies which used a single set of data. This pooling of data increased the number of observations and the reliability of estimations. In addition to infant birth and death histories, the database contained a rich set of variables related to marriage histories, characteristics of established marriages and the factors listed above.
Weighted, multi-stage and stratified cluster sampling was performed accompanied by unified questionnaires (differences in questions were negligible). The large set of data obtained by pooling the four surveys offers two important advantages. Firstly, since more observations were included in analyses, confidence intervals become narrower and estimates become closer to point estimates. Secondly, it facilitates the analysis of infant deaths, which are essentially rare events, by using information from a large number of observations.
The TDHS surveys collected data at national level, with rural–urban distinction and at regional level. Information about consanguineous marriages was collected on the basis of marriage histories and information on infant mortality on the basis of birth histories. Detailed information on all other control variables came from the relevant modules of the survey household and individual questionnaires.
While the sample designs and questionnaires of the four surveys were the same, their sample sizes differed. Hence, the number of women interviewed and the number of children whose information was collected through birth histories were different. Hence, in order to avoid possible biases in the analyses stemming from the different number of observations in different surveys, weighting factors obtained from the equation 1/(a×n c/n T) were used (Marriot et al., 2007), where a is the number of surveys, n c is the number of respondents for survey c, and n T is the total number of respondents for all surveys.
Variables
The dependent variable was child survival. Infant mortality rate was divided into neonatal (first month in life) and post-neonatal (1–11 months), as causes of death in these two periods may be different, and thus the effects of consanguineous marriage may differ in the two different periods.
Consanguineous marriage is the main independent variable, classified as first-degree (first cousin), second-degree (second cousin) and distant consanguinity (further than second cousin). However, since there was not a sufficient number of observations for the second-degree, and especially for the distant relative categories, in both the descriptive and multivariate analyses marriages were classified as ‘non-consanguineous’, ‘consanguineous to the first degree’ and ‘other relatives’. Control variables other than those related to the time dimension included: household wealth level, mother’s education, father’s education, mother’s employment status, father’s employment status, mother’s age at birth, mother’s native language, father’s native language, form of marriage ceremony (whether religious ceremony was performed), arrangement of marriage (how marriage decision was taken), bride payment, health insurance status of family, child’s sex, birth order, birth interval, region where the mother was socialized, mother’s childhood place of residence, source of drinking water, type of toilet and number of persons per sleeping room in the dwelling. The Mosley & Chen framework (Mosley & Chen, Reference Mosley and Chen1984), which is commonly used when studying the relationship between infant mortality and socio-demographic factors, was used to identify these variables. The rationale of this framework is that infant deaths constitute a multi-dimensional phenomenon (affected by mother and infant characteristics and cultural, environmental and socioeconomic factors) that is not susceptible to explanation by referring to a few variables. Table 1 shows the explanatory/control variables identified on the basis of this framework.
Table 1 Explanatory/control variables used in the study

Statistical method
In order to single out the effect of consanguineous marriages on infant mortality, the method of survival analysis, also known as ‘event history’ or ‘duration’ analysis, was used. Event history analysis assesses the occurrence and timing of an event and gives due account to the time dimension while exposing causal relationships (Allison, Reference Allison1984; Blossfeld & Rohwer, Reference Blossfeld and Rohwer2002).
The incomplete nature of data from cross-sectional studies can cause the observation process to be subjected to right- and left-censoring, which creates a significant problem in analyses. In this case, some infants, as units of analysis, had yet not completed the period of 1 year of observation at the time of interview. Classical regression techniques cannot cope with this. The life-table technique, widely used in demography, can cope with the problem of censoring, but fails to account for the simultaneous effects of other factors while measuring the effect of any given factor. By combining the classical regression and life-table techniques, survival analysis techniques can cope with the problem of right-censoring and expose the net effect of any given factor while controlling for the effects of others. In the analysis, the piecewise constant Proportional Hazard Regression model, which is a parametric method of analysis, was used. Parametric methods are better than non-parametric methods in that they allow analysis for fewer observations and for many other reasons (Blossfeld et al., Reference Blossfeld, Golsch and Rohwer2007). Parametric survival analysis methods use a fixed baseline for the risk of an event taking place and assume different names depending on the form of this baseline. This study used a piecewise constant function model, which is especially useful when the form of the time dependence of the social process under study is not clear. The time factor is divided into pre-defined segments and it is assumed that the rate between segments changes while it remains constant within segments.
The event studied in the analysis is infant mortality. The process time starts with the birth of the baby and ends when the event takes place – that is, the date when the baby dies. The period of observation is one year. It may be that this period of observation ends with the death of the infant or it may end at the date of interview for infants who have yet not completed their first year of life. The baseline hazard, which is important in terms of event history, is the period of time elapsed since the birth of the baby and is measured in months. The baseline hazard is the dependent variable in the analysis. Independent variables used in the analysis consisted of a broad set in a way to control for characteristics related to the environment and household, socioeconomic characteristics of mother and father, cultural characteristics of the mother and bio-demographic factors.
Limitations
The 1993, 1998, 2003 and 2008 TDHS surveys encompass many, but not all, variables that impact on infant deaths as a multi-dimensional phenomenon. These household-based field surveys could not cover such issues as cause of death of the infant, infantile diseases and genetic factors causing death. Hence, the analyses in this study were limited to variables appearing in the pooled data set. Also, information related to antenatal care, birth attendants, form of delivery, place of delivery, child immunization and nutrition was only collected for children born within the last five years. Since the study set out to use information collected for all children that a woman had in her lifetime, such information collected only for children born within the last five years was inevitably excluded. Nevertheless, the exclusion of these variables should not have a significant bias on the outcomes of the study since antenatal and postnatal service coverage had already climbed to over 90%, and variables such as woman’s educational status, household wealth level and status of health insurance, which control whether these services are received or not, already exist in the data set used.
Results
Descriptive analysis
Infant mortality
The infant mortality rate was 275 per 1000 live births in the mid-1940s, and declined steadily to 163 in the mid-1960s, to 121 in the early 1980s and to 66 in the early 1990s. In the 2000s it started to drop faster: to 29 in 1000 live births in the mid-2000s and then to 17 at the end of the decade (Fig. 1). Behind this remarkable decline, which occurred at a time of rapid socioeconomic development, were the maternal and child health programmes that were intensively implemented in Turkey starting from the 1980s. Although Turkey has covered a significant distance in a relatively short period of time, the infant mortality rate in Turkey is still four times higher than in EU countries.
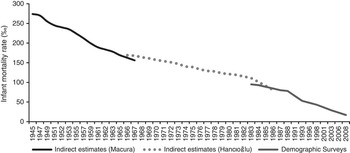
Fig. 1 Trend in infant mortality rate in Turkey, 1945–2008. Source: Koç et al. (Reference Koç, Eryurt, Adalı and Çağatay2010).
Neonatal and post-neonatal mortality rates, which together make up the infant mortality rate, are also changing rapidly in Turkey. Until the 1990s, post-neonatal deaths accounted for the majority of infant deaths; from 1993, however, neonatal deaths came to the fore as making up a larger share of infant deaths. The TDHS-2008 showed that 76% of infant deaths occurred in the neonatal period (Fig. 2). Since 86% of neonatal deaths are early neonatal deaths, it is clear that the short-term policy priority for Turkey should be further strengthening neonatal programmes that are being, or plan to be, implemented.
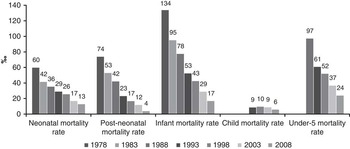
Fig. 2 Trends in neonatal, post-neonatal and infant mortality rates in Turkey, 1978–2008. Source: Koç et al. (Reference Koç, Eryurt, Adalı and Çağatay2010).
The rate of infant mortality in Turkey varies significantly by region. As can be seen in Fig. 3, it has declined rapidly in all regions over the last 30 years. According to TDHS-2008, the infant mortality rates in the West, Central and North regions are below the country average, but above average in the South and particularly East regions. Although the infant mortality rate declined by 63% in East in the period 2003–2008, the rate in this region was still 1.5 times higher than the country average and 2.6 times higher than the average for West region (Fig. 3). This large gap in early infant mortality between the East and the rest of the country must be eliminated by altering policy priorities.
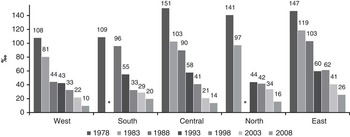
Fig. 3 Trend in infant mortality rates by region in Turkey, 1978–2008. Source: Koç et al. (Reference Koç, Eryurt, Adalı and Çağatay2010).
Consanguineous marriages
The first statistical information on consanguineous marriages in Turkey came from a 1968 survey entitled Survey on Family Structure and Population Problems in Turkey (Timur, Reference Timur1972), which showed that about 27% of women were engaged in consanguineous marriage. Subsequent studies suggest that this rate has not fallen significantly, varying from 22 to 24% (Table 2). Demographic surveys conducted in the period 1993–2008 showed that the rate of consanguineous marriages was highest in the East and lowest in the West, and much more common in rural than in urban settlements.
Table 2 Trend in consanguineous marriages in Turkey by region, urban/rural residence and survey date

Consanguineous marriage rates calculated from demographic surveys are somewhat contaminated since the unit of analysis used was all ever-married women regardless of their marriage cohort. Due to this ‘contamination’ of information, changes in consanguineous marriages over time cannot be determined with such analysis. Hence, this study conducted analysis over generations of marriages in order to present changes in consanguineous marriages over time. According to the analyses presented in Table 3, the rate of consanguineous marriages for women marrying in 1978 or earlier was 36%. The rate declined to 31% in the period 1979–1983, 27% in 1989–1993, 21% in 1999–2003 and dropped to 19% in the period 2004–2008. Another development appearing as a result of these analyses is the decrease in the share of women engaged in first-degree consanguineous marriage. While in 1978 and earlier about 60% of consanguineous marriages were between first-degree relatives (i.e. first cousins of either parents) this dropped to 48% in the period 2004–2008. This suggests that there has been an overall decline in consanguineous marriages in Turkey with a shrinking share of first-degree consanguineous marriages accompanied by an increasing share of second-degree and other consanguineous marriages (Table 3).
Table 3 Trend in consanguineous marriages in Turkey by marriage cohort, TDHS-2008

Consanguineous marriages and infant mortality
Looking at the relationship between consanguineous marriages and infant mortality by marriage cohorts (Table 4), it can be seen that infant mortality rates have in general declined, following the overall trend in the country, for all mothers regardless of consanguineous marriage status. However, the infant mortality rate for the children of mothers with consanguineous marriages is still higher than that for Turkey as a whole, and for the children of mothers with non-consanguineous marriage, for all marriage cohorts. However, the basic distinction is between the infant mortality rate of women with first-degree consanguineous marriages and those of any consanguineous marriage. For the period 2004–2008, the most recent one, the infant mortality rate for women with first-degree consanguineous marriages was 54% higher than that for women with any consanguineous marriage (25.1 per 1000 live births and 16.3 per 1000 live births, respectively).
Table 4 Infant mortality rates by marriage cohort and consanguinous marriages, TDHS-2008

a The number of observations for these cohorts was insufficient.
Multivariate analysis
Multivariate analysis with seven models was conducted using the ‘event history’ method to examine the causal effect of consanguineous marriage on infant deaths. The objective of the modelling, where variables are added from one model to the next, was to discern the additional contribution of control variables other than consanguineous marriage itself to infant mortality (the dependent variable). The first model (the Basic Model) is the baseline hazard from birth obtained by taking into account the period from birth, showing whether the infant was alive in the first month of life (neonatal period) and in the ensuing 11 months (post-neonatal period); the periodic variable obtained by considering the birth date of the infant was included in the model. The second model (Consanguineous Marriage Model) assesses the effect of consanguineous marriage on infant deaths controlling for other variables. Under the third model (Parental Characteristics Model) the effect of consanguineous marriage on infant deaths was investigated by adding the variables education and employment status of parents and age of the mother when giving birth. In the fourth model (Cultural Factors Model) the form of marriage ceremony, bride payment, how the marriage decision was taken (arrangement of marriage) and native languages of parents were controlled for. In the fifth model (Environmental Factors Model) the effect of consanguineous marriage on infant deaths was checked by controlling for the source of drinking water used in the house, toilet type and number of persons per sleeping room. The sixth model (Bio-demographic Factors Model) added the sex of the child, whether single or multiple birth, birth order and birth interval. The seventh and last model was the General Factors Model, which included the settlement place and region of the mother, household wealth status and health insurance coverage (Table 5).
Table 5 Multivariate analysis of the causal relationship between consanguineous marriages and infant mortality rate, Turkey

a The other controlling variables used in each model are given in Table 1.
Ref., reference category; ns, not significant.
The Basic Model
Looking exclusively at the relationship between the baseline hazard (duration since birth and child’s date of birth) and infant mortality, it is seen that the infant mortality rate during the first month in life, that is in the neonatal period, was about 2 times that in the post-neonatal period (p<0.01) (Table 5). By periods on the basis of the birthday of the child, the likelihood of infant death has decreased significantly over time. If the likelihood of the death of infants born at dates closest to the TDHS-2008 (i.e. 2004–2008) is taken as the reference category, the likelihood of death of infants born in the period 1994–1998 is 20.6 times higher, and 135.2 times higher for infants born in 1973 and earlier (p<0.01). According to calculations made on the basis of the relationship between initial likelihood and model likelihood, the Basic Model explains 17% of the variation in infant mortality. This shows that the baseline hazard – the time effect – is quite important in accounting for changes in infant mortality.
The Consanguineous Marriage Model
This showed that the likelihood of death for infants born to first-degree consanguineous marriage was 2.12 times higher than that for infants born to non-consanguineous marriage (p<0.01). Further, the likelihood of infant death in other (second-degree and further) consanguineous marriages was 1.62 times higher than that in marriages without any consanguinity (p<0.01). Outcomes from this show that the effect of the baseline hazard on infant deaths was sustained when the consanguineous marriage variable was included.Variables in this model explained 18% of the variation in infant mortality. The fact that this model had an additional contribution over the first can be interpreted as consanguineous marriage contributing to variations in infant mortality (Table 5).
The Parental Characteristics Model
This examined the effect of consanguineous marriage on infant mortality while controlling for the baseline hazard and variables related to parental characteristics (parents’ education level, employment status and age of the mother when giving birth). The outcomes of this model suggest that first-degree consanguineous marriage increases the likelihood of infant death 1.51 times in comparison to marriages with no consanguinity and other consanguineous marriages by 1.31 times (p>0.01). The baseline hazard maintains its effect on infant deaths in this model too. The parental characteristics variables were observed to be important in explaining infant deaths, with the exception of parents’ employment status. For example, the likelihood of death for infants born to mothers with lower than primary education was 4.57 times higher than that of infants born to mothers with secondary and higher education (p<0.01). Further, giving birth while the mother was under the age of 20 increased the likelihood of infant death 3.27 times compared with giving birth aged 20–34. The finding that this model explains 28% of variation in infant mortality indicates that the parental characteristics were quite important in explaining infant deaths (Table 5).
The Cultural Factors Model
When variables related to cultural factors (form of marriage ceremony, bride payment, arrangement of marriage, native language of parents) were included in the model, the explanatory effect of consanguineous marriage on infant deaths persisted. Relative to infants born to parents without consanguinity, the likelihood of death of infants born to first-degree consanguineous marriage mothers was 1.49 times higher (p<0.01), and 1.23 times higher (p<0.05) for other types of consanguineous marriage (Table 5). The parental variables and baseline hazard maintained their effect in this model. The likelihood of death of children born to mothers for whom bride payment was paid was 1.37 times higher than that of children born to mothers for whom no such payment was made (p<0.01). Although the likelihood of death of infants whose parents’ native language was Kurdish was found to be higher than that of infants with Turkish-speaking parents, the difference was not statistically significant. As for the other cultural factors, they had no explanatory effect on infant deaths. This model adds to the earlier one by explaining 30% of variation in infant mortality.
The Environmental Factors Model
When variables related to environmental factors (i.e. quality of drinking water used by households, connection of toilets to a piped sewer system, number of household members per sleeping room) were included in the model, the explanatory effect of first-degree consanguineous marriages on infant deaths was still valid, while that of other consanguineous marriages disappeared, although still having the effect of increasing infant deaths. Compared with infants born to non-consanguineous marriages, the likelihood of death of infants born to first-degree consanguineous marriages was 1.49 times higher (p<0.01), and 1.22 times higher (p<0.05) for infants born to second-degree and other consanguineous marriages. In this model too, the effects of baseline hazard, parental characteristics and cultural factors persisted. The variables related to environmental factors were found to have an explanatory effect on infant deaths. The likelihood of infant deaths was 1.25 times higher (p<0.01) in households without safe drinking water and 1.16 times higher (p<0.05) in households using toilets not connected to the sewage system. As the number of persons per sleeping room increased, that is as the household becomes more crowded, so does the likelihood of infant death, and when it was four and over, the likelihood of infant death was 2.19 times higher (p<0.01) than when there was only one person per sleeping room. Relative to the earlier model, this model explained 32% of the variation in infant mortality (Table 5).
The Bio-Demographic Factors Model
This model added bio-demographic factors (i.e. sex of the child, single or multiple birth, birth order and birth interval). After controlling for all variables included in this model, it was found that the likelihood of death for infants born to first-degree consanguineous marriages was 1.51 times (p<0.01) higher than that of infants born to non-consanguineous marriages (Table 5). In addition, under this model the likelihood of infant death did not differ for mothers in non-consanguineous marriage and others with second-degree and more distant consanguineous marriages (p>0.05). The variables that contributed to explaining infant deaths in the earlier models persistently in this model. The only exception was the variable related to whether the toilet was connected to the sewage system, which was statistically insignificant when bio-demographic factors were included in the model. At this stage, all bio-demographic factors except child’s sex contributed to the variation in infant mortality. The likelihood of infant death in multiple births was 7.13 times higher (p<0.01) than in single births. In addition, the likelihood of infant death for first births was 5.30 times higher than for second births (p<0.01); and the likelihoods of infant death in short (<24 months) and medium (24–36 months) birth intervals were, respectively, 4.72 (p<0.01) and 2.46 (p<0.01) times higher than in long birth intervals (>36 months). This model contributed 38% of the total variation in infant mortality.
The General Factors Model
This model encompassed variables such as the environment where the mother experienced her childhood, household wealth status and whether the mother was covered by a health insurance scheme. In this model, the likelihood of infant death among children born to first-degree consanguineous marriage was higher by 44% than that among children born to non-consanguineous marriages (p<0.01). Again, the statistically significant infant mortality effect of variables included in earlier models persisted. Taking the variable ‘mother’s region of socialization (mother’s childhood region)’, it was found that the likelihood of infant death among children whose mothers spent their childhood in the East was 1.99 times higher (p<0.01) than that for children born to mothers who spent their childhood in the West. The likelihoods of infant death were 1.73 (p<0.01) and 1.51 (p<0.01) times higher in North and Central regions, respectively, compared with the West. There was no difference in the likelihood of infant death for mothers from West and South regions (p>0.05). Although the likelihood of infant death was higher in rural areas, it does not seem to have any effect on infant mortality due to the fact that the difference is statistically insignificant (p>0.05). The likelihood of infant death increased as household wealth status decreased, and was 1.85 times higher for children born to households at the lowest level of welfare compared with those born to households with the highest level of wealth (p<0.01). Similarly, the likelihoods of infant death for children born to households of high and medium wealth status were, respectively, 1.45 and 1.38 times higher (p<0.01) than that for children born to households with the highest wealth status (p<0.01). There was no difference in the likelihood of infant death for mothers who were covered by health insurance and those who were not (p>0.05). However, the likelihood of infant death for children born to Green Card holder mothers was about 2 times higher than that for children born to mothers with health insurance (p<0.01). Contributing an additional 3 percentage points, this model lifted the explained variation by up to 41% (Table 5).
Findings on the basis of place of residence
The final model for Turkey nationwide, with an explanatory level of 41%, was re-analysed by urban/rural settlement as the consanguineous marriage dynamics differ for urban and rural areas (Table 6). Consanguineous marriage was found to be an important factor in explaining infant deaths in both urban and rural areas, even other variables were controlled for. Taking the likelihood of infant death in children born to mothers whose marriages were not consanguineous as reference, it was observed that the likelihood of infant death for urban children was 1.57 (p<0.01) times higher and that for rural children was 1.39 times higher (p<0.01). The likelihood of infant death for children born to second-degree or more distant consanguineous marriages was not different from the likelihood of infant death for children born to non-consanguineous marriages. Furthermore, the likelihood of infant death of children born in rural areas in 1973 and earlier was 192 times higher than that of children born in 2004–2008, and this difference was 77 times for urban areas. This shows that the rate of decline in rural infant mortality was higher. Some variables that were important in explaining infant deaths in the models for Turkey as a whole and for urban settlements (i.e. father’s education and payment of bride payment) lost this effect in rural areas. This situation is associated with the fact that divergence/variance on the basis of these two variables was not significant in rural areas.
Table 6 Multivariate analysis of the causal relationship between consanguineous marriage and infant mortality rate in Turkey, by place of residence

a The other controlling variables used in each model are given in Table 1.
Ref., reference category; ns, not significant.
Discussion
The principal aim of the study was to answer the question: ‘Do consanguineous marriages, particularly those to the first degree, have the effect of increasing infant mortality?’ Although 20 years have passed since the coining of the term Turkish Puzzle by Gürsoy-Tezcan (Reference Gürsoy-Tezcan1992) to describe Turkey’s high infant mortality in contrast to its level of economic development, the puzzle has not yet been resolved. Behar et al. (Reference Behar, Courbauge and Gürsoy1999) drew attention to this when pointing out that Turkey’s infant mortality rate in the 1990s was higher than that of nearby countries with much lower per capita incomes. Similar emphases were made later by Riddle (Reference Riddle1998), Eryurt and Koç (Reference Eryurt and Koç2009) and Yüksel and Koç (Reference Yüksel and Koç2010).
Over the last two decades Turkey has undergone significant transformations that would be expected to bring down its infant mortality rate. The proportion of fully immunized infants rose from 40% to 81%, the proportion of infants with malnutrition decreased from 40% to 10%, and the proportion of women receiving antenatal care and delivering in a health facility and attended by qualified health personnel reached over 90%. In the same period there were also significant improvements in the proportion of women and infants receiving postnatal care and services related to birth registration. Again, in the same period, there was a rapid increase in per capita income (Koç et al., Reference Koç, Eryurt, Adalı and Çağatay2010). Despite significant reductions in infant mortality, these were not at levels commensurate with the changes taking place in the nation’s health and economy. Hence, compared with countries with similar health and economic indicators, Turkey remains among those countries with high infant mortality rates. For instance, while Turkey has per capita incomes higher than Romania, Albania, Bulgaria, Georgia, Moldova, Bosnia and Herzegovina, Macedonia, Syria, Ukraine, Hungary, Poland and Croatia, all these countries have infant mortality rates lower than, or very close to, that of Turkey. Spain, Portugal, Republic of Southern Cyprus and Greece have per capita income figures similar to that of Turkey, but their infant mortality rates are lower, at around 4–5 in 1000 live births (World Bank, 2013). This situation points to other factors, such as consanguineous marriages for example, which are resistant to improvements in health and economic indicators, affecting infant mortality in Turkey. Hence, the present study sought to single out the effect of consanguineous marriages – one of the most persistent social institutions in Turkey – on infant deaths while controlling economic, social, biological, environmental and other factors.
Examining the outcomes of the multivariate analyses, it was found that first-degree consanguinity increased infant mortalty rates to some extent in all models. In the second model, which just covered duration variables and consanguinity, first-degree consanguineous marriages increased the likelihood of infant death by 2.12 times (p<0.01), while other types of consanguineous marriage increased it by 1.62 times (p<0.01). The model including parental characteristics such as parents’ education, employment status and mother’s age at birth showed that first-degree consanguineous marriages increased infant deaths by 1.52 times (p<0.01) and other consanguineous marriages increased it by 1.31 times (p<0.01). This situation suggests those in consanguineous marriages essentially differ by parental characteristics. Even in the last models, which included all variables, first-degree consanguinity enhanced infant deaths by 1.44 times (p<0.01) while other marriage types increased it by 1.12 times. In the last model, however, the effect of consanguineous marriages other than first degree ceased to be statistically significant.
Examining the outcomes by urban–rural area, assuming that determinants of infant deaths may have different effects in rural and urban settlements, it was found that infant deaths in urban settings were concentrated more in the neonatal period. Though infant mortality rates were higher in rural areas, their decline over time has been faster. The effect of consanguineous marriages on infant deaths is more pronounced in urban areas given their higher level of socioeconomic and demographic diversification. In sum, the multivariate analyses show that, in Turkey, first-degree consanguinity has increased infant mortality by 45% overall, and by 57% in urban and 39% in rural areas, controlling for other socio-demographic covariates.
The close relationship between consanguinity, especially first-degree, and early-age mortality, is not special to Turkey. Many studies have demonstrated a relationship between first-degree consanguinity and early-age mortality in different social context. Shami et al. (Reference Shami, Schmitt and Bittles1989) and Grant and Bittles (Reference Grant and Bittles1997) found that, in Pakistan, there was a highly significant relationship between consanguinity and early-age mortality, controlling for a number of socioeconomic and demographic determinants, such as maternal age, maternal education, sex of child, birth order and birth interval. Another study by Hussain et al. (Reference Hussain, Bittles and Sullivan2001), which covered the neighbouring countries of Pakistan and India, measured the impact of first-cousin consanguinity on early-age mortality. They showed a highly significant risk among the children of first-cousin consanguinity unions during the neonatal, post-neonatal and infancy period using both bivariate and multivariate analyses. A study conducted by Joseph (Reference Joseph2007) in the Bekaa Valley/Lebanon, controlling for selected demographic and socioeconomic factors, found a negative impact of first-cousin unions on infant mortality rates, but not on child mortality rates. El-Hazmi et al. (Reference El–Hazmi, Al-Swailem, Warsy, al-Swailem, Sulaimani and al-Meshari1995) also indicated a close relationship between first-degree consanguinity and early-age mortality in Saudi Arabia. The study of Khoury and Massad (Reference Khoury and Massad2000) in Jordan also showed an increasing impact of consanguinity on infant mortality rates. Another study covering selected Arab countries has also pointed out that consanguinity, particularly first-degree consanguinity, has had an escalating impact on the rate of infant mortality (Abuqamar et al., Reference Abuqamar, Coomans and Louckx2011). Another recent study by Charafeddine et al. (Reference Charafeddine, Ammous, Kobeissi, De Ver Dye, Matar, Faddous Khalife and Yunis2012) in Lebanon established that consanguinity was a significant determinant of mortality in the infancy period after controlling for a crowding index, maternal age and education, prenatal care, mode of delivery, sex of children and birth weight. Jemai et al. (Reference Jemai, Messaoudi, Chaouch and Kerkeni2007), on the other hand, showed that there was a positive correlation between first-cousin marriages and rates of neonatal and post-neonatal mortality in Tunisia. Hosseini-Chavoshi et al. (Reference Hosseini-Chavoshi, Abbasi-Shavazi and Bittles2014), in their descriptive study in Iran, pointed out that the mean postnatal mortality in the country was higher in the progeny of consanguineous parents, and the percentage of deaths was greater among first-cousin than second-cousin offspring. The studies conducted by Mokhtar and Abdel-Fattah (Reference Mokhtar and Abdel-Fattah2001), Hammami et al. (Reference Hammami, Chalbi, Ben Abdallah and Elgazzeh2005) and Khayat and Saxena (Reference Khayat and Saxena2007) in Egypt found similar results by presenting the linkages between first-degree consanguinity and early-age mortality rates. These findings, and those of other studies in different geographic contexts (Hussain, Reference Hussain1999; Pedersen, Reference Pedersen2002; Jurdi & Saxena, Reference Jurdi and Saxena2003; Weinreb, Reference Weinreb2008), are consistent with the present study in their finding of a significant positive relationship between first-degree consanguineous marriage and infant mortality.
There are two practical implications of the findings of this study. First, the findings point out the need for comprehensive research on consanguineous marriage and its determinants in Turkey. Secondly, they draw attention to the need to strengthen genetic counselling services in Turkey. Infant deaths from environmental causes have been considerably reduced by immunization campaigns and improvements in maternal and child health. Now infant deaths are largely concentrated in the neonatal period, and these are known to be associated essentially with genetic factors. Consanguineous marriages facilitate the transfer of genetic disorders to the next generation. Factors such as shrinking family size, spread of urbanization, rising education level and the labour force participation of women will, in the course of time, further reduce the incidence of consanguineous marriage. However, to minimize the negative effect of such marriages on infant mortality and child health, families at high risk of carrying genetic diseases should be identified and genetic counselling services offered (WHO, 2006).









