



Introduction
Obesity is widely known to be a global pandemic problem (Popkin et al. , Reference Popkin, Adair and Ng2012), and is largely caused by the continuing nutrition transition (Morris, Reference Morris2010). Low- and middle-income countries are now facing a faster transition than high-income countries, caused by high urbanization rates that involve rapid short-term adaptive strategies that are potentially obesogenic (Olszowy et al., Reference Olszowy, Pomer, Dancause, Sun, Silverman and Lee2015; Downey, Reference Downey2016). Indeed, the nutrition transition is characterized by changing dietary habits and sedentary lifestyles within on-going urbanization, exposing populations to obesity and cardio-metabolic diseases (Delpeuch, Reference Delpeuch2013). In sub-Saharan African populations, the level of obesity continues to increase more aggressively than in high-income countries (Connor Gorber et al., Reference Connor Gorber, Tremblay, Moher and Gorber2007; Stevens et al., Reference Stevens, Singh, Lu, Danaei, Lin, Finucane and Bahalim2012; Steyn & Mchiza, Reference Steyn and Mchiza2014). In addition, the prevalences of diet-related non-communicable diseases (NCDs) such as hypertension and type 2 diabetes are increasing in these settings (Ebrahim et al., Reference Ebrahim, Pearce, Smeeth, Casas, Jaffar and Piot2013).
Table 1 Composition of the urban focus groups

a When applicable the work of each young participant is mentioned. In general, female participants did not work and all highly educated participants were students.
b For older women without an occupation the occupational status of their husband is given.
P: Participant; F: Father; M: Mother; H: Husband.
Table 2 Composition of the rural focus groups

a In the rural area most fathers were farmers and/or artisans (carpenters, masons etc.) and most mothers were farmers and at home.
b When applicable the work of each young participant is mentioned.
c For older women without an occupation the occupational status of their husband is given.
P: Participant; F: Father; M: Mother; H: Husband.
In the context of urbanization in Africa, which is characterized by a rural exodus and intensification of internal migration, new migrants are progressively exposed to NCDs (Oyebode et al., Reference Oyebode, Pape, Laverty, Lee, Bhan and Millett2015). Nevertheless, their traditional preference for stoutness (overweight/obesity) seems to remain in these obesogenic areas, as observed in Ghana, Cameroon and Nigeria (Appiah et al., Reference Appiah, Otoo and Steiner-Asiedu2016; Akindele et al., Reference Akindele, Phillips, Igumbor and Useh2017; Cohen et al., Reference Cohen, Amougou, Ponty, Loinger-Beck, Nkuintchua and Monteillet2017). Indeed, the propensity towards stoutness is strengthened during the internal migration, particularly as this paradigm is viewed as a sign of successful integration into the modern urban lifestyle associated with abundance. In comparison, if the social valorization of stoutness is established in the rural setting, where food insecurity is higher, this appreciation is moderate due to the high physical strength necessary for manual labour (De Garine, Reference De Garine1962; Sear & Marlowe, Reference Sear and Marlowe2009). Thus, in urban obesogenic settings, this sociocultural phenomenon becomes pronounced as migrants from rural settings still believe in increasing fat stores to lower the risk of extreme undernutrition during times of seasonal adversity.
Urban migrants are therefore proud to flaunt their larger body size (Brown & Konner, Reference Brown and Konner1987; De Garine, Reference De Garine1990; Agyemang et al., Reference Agyemang, Addo, Bhopal, Ade and Stronks2009). Accordingly, a social valorization of high body fat (Mvo et al., Reference Mvo, Dick and Steyn1999; Blocker & Freudenberg, Reference Blocker and Freudenberg2001) seems to be spreading in African populations and is becoming a risk factor for excess fat accumulation, as observed in urban Cameroon (Cohen et al., Reference Cohen, Boetsch, Palstra and Pasquet2013). This valorization of stoutness usually involves high-calorie food consumption (Ndoye & Diop, Reference Ndoye and Diop2001; Bricas, Reference Bricas and Chiffoleau2008) and deliberate low physical activity (Rguibi & Belahsen, Reference Rguibi and Belahsen2006; Warnier, Reference Warnier2009) to gain weight. Therefore, this factor could be considered as a biocultural determinant of the obesity pandemic (Brewis, Reference Brewis2011), especially in African populations and the African diaspora (Flynn & Fitzgibbon, Reference Flynn and Fitzgibbon1998; Krauss et al., Reference Krauss, Powell and Wada2012).
The present study focuses on Senegal, where little previous research has been conducted on the biocultural determinants of overweight/obesity, such as body weight perceptions. The Senegalese region is experiencing a nutrition transition (Maire et al., Reference Maire, Delpeuch, Cornu, Tchinbindat, Simondon, Massamba, Salem and Chevassus-Agnès1992; Abubakari et al., Reference Abubakari, Lauder, Agyemang, Jones, Kirk and Bhopal2008), which has intensified the urbanization associated with a rural exodus (Duboz et al., Reference Duboz, Macia, Chapuis‐Lucciani, Boëtsch and Gueye2012). Thus, overweight has become prevalent in urban areas, where the physical environment has become obesogenic as a consequence of economic development (Macia et al., Reference Macia, Duboz and Gueye2010), increasing sedentary behaviours and the consumption of cheap processed foods accessible to the working class in poor urban neighbourhoods (Sobal & Stunkard, Reference Sobal and Stunkard1989; Drewnowski, Reference Drewnowski2009; Temple & Steyn, Reference Temple and Steyn2011).
Nevertheless, for women living in the peripheral neighbourhoods of Dakar, this obesogenic physical environment could be compounded by the sociocultural environment since these women value stoutness and want to deliberately gain weight (Holdsworth et al., Reference Holdsworth, Gartner, Landais, Maire and Delpeuch2004; Gning et al., Reference Gning, Thiam, Fall, Ba-Fall, Mbaye and Fourcade2007). Indeed, traditional views of body size in Senegal promote stoutness in women as a symbol of a peaceful and wealthy household (Ndiaye, Reference Ndiaye2006), and this trend persists with the current rural exodus (Duboz et al., Reference Duboz, Macia, Gueye, Boëtsch and Chapuis-Lucciani2011), with a valorization of processed and high-calorie food in populations of lower socioeconomic status (SES) in Dakar (Ndoye & Diop, Reference Ndoye and Diop2001; Bricas, Reference Bricas and Chiffoleau2008).
Senegalese urban areas present both ecological and sociocultural obesogenic components, i.e. a physical and sociocultural environment that facilitates obesity (Macia et al., Reference Macia, Cohen, Gueye, Boetsch and Duboz2017), as observed in other African countries (Cohen et al., Reference Cohen, Amougou, Ponty, Loinger-Beck, Nkuintchua and Monteillet2017). This dynamic social–ecological context (Saarloos et al., Reference Saarloos, Kim and Timmermans2009) has its own anthropological specificities involving a complex, unique and potentially obesogenic lifestyle (Ulijaszek & Lofink, Reference Ulijaszek and Lofink2006). Nevertheless, the impact of the social valorization of stoutness on weight gain is uncertain and has rarely been studied.
The literature identifies many factors that play a major role in the development of obesity, both hereditable and environmental, i.e. social–ecological (Popkin & Gordon-Larsen, Reference Popkin and Gordon-Larsen2004). Nevertheless, each human population could be exposed simultaneously to several determinants of obesity. The interaction between the heritable and environmental determinants obesity in different contexts has been relatively little studied, with the exception of holistic anthropology (Parkin & Ulijaszek, Reference Parkin and Ulijaszek2007). An anthropological global investigation using an integrative approach is appropriate to understand a complex human interdisciplinary phenomenon such as obesity (Dufour, Reference Dufour2006), and was used in this study to identify how the ecological and sociocultural environments within the urbanization process interact with each other to expose the population to overweight, obesity and hypertension in Senegal (Saarloos et al., Reference Saarloos, Kim and Timmermans2009). Therefore, this study’s aims were to (1) determine the joint influence of biocultural factors (body weight perceptions, eating behaviours, physical activity) on the nutritional status of Senegalese migrating from a rural to urban/suburban area in Dakar, and (2) to provide a holistic understanding of the Senegalese nutrition transition to identify which stage is being experienced by the country.
Methods
The study included: (i) a qualitative study to identify the biocultural determinants of overweight/obesity, including body weight norms, physical activity and diet practices; (ii) a quantitative study to assess the respective effects of these determinants using specific African photographic stimuli (Body Size Scale, BSS) associated with a Body Image Assessment Guide (BIAG) and a questionnaire assessing diet and physical activity, and (iii) anthropometric measurements.
Two areas of Senegal were studied for the purposes of comparison: the agglomeration of Dakar city centre and suburb and a rural area of the Wolof region, including three villages in the Kaolack region: Diamaguene, Keur Ndary Ndiaye and Gandiaye, where the socioeconomic conditions of the inhabitants are among the lowest in the country (AG/GRN-GTZ, 2004).
Qualitative study
Study process
The aim of the qualitative analysis was to define the biocultural determinants of overweight/obesity by: (i) describing the different vernacular conceptions associated with body weight: fertility, power, well-being, good health and beauty (Mvo et al., Reference Mvo, Dick and Steyn1999), (ii) identifying the different culinary local practices that characterize the Senegalese diet, (iii) analysing their relationship with physical activity, and (iv) detecting whether acculturation is occurring. This process was integral to the quantitative study, since the variables tested by the measurement tools (BSS, BIAG and questionnaire) cannot be isolated from their sociocultural context. The results of the qualitative study were important to identify the local norms of body weight, diet and physical activity, and to interpret the results of the quantitative study. Indeed, the qualitative data on diet, physical activity and body weight norms were used to test for causal links between these aspects and weight gain, which would have been impossible to establish based on quantitative data only.
Data sampling and processing
Focus group discussions were used to explore in-depth local representations of overweight/obesity determinants (Stewart & Shamdasani, Reference Stewart and Shamdasani1990). In 2011 and 2012, fourteen focus groups discussions were conducted, each with six participants recruited from various neighbourhoods of the two study areas according to three criteria: age (<25 years, and >45 years); sex; and educational level (<high school level: non-completion of high school, ≥high school level: completion of high school) or occupational category level (low occupational level, e.g. manual trades, small shopkeepers; high-income occupational level, e.g. senior executive level, health care professional) (Tables 1 and 2). Educational level alone could not be considered since this does not cover the total population in rural and urban areas as the percentage of highly educated people is low, especially in elders. It was replaced, when necessary, by occupational category level, the two indices being positively correlated in Dakar. Six focus group discussions were conducted in the rural study area (Kaolack region) and eight in the urban area (Dakar agglomeration) since the socioeconomic and educational gradients among rural middle-aged and elderly people were very low (ANSD-ICF, 2015).
Participants were selected inside a network of relationships by local interviewers with experience in conducting local anthropological studies. Contrary to the quantitative study, the subjects’ study participation was somewhat arbitrary as their agreement to participate in the detailed protocol may have depended on their inclusion in the study network, and the study required participants with sufficient knowledge and interest in the research. These two criteria were simultaneously assessed while screening candidates for study participation. Although the sample was selected with the aim of covering all Senegalese points of view, it was not fully representative of the population as participants (key informants) were selected via their relationship with some of the research assistants. Nevertheless, the sample presented a balanced sex ratio and all participants belonged to the Wolophone group. Focus groups discussions were performed in neighbourhoods to allow participants to express themselves in a familiar context without exterior pressure, and recorded with a hand-held recorder. The discussions (and all other methods) were conducted in Wolof, the main vernacular language of the participants, and then translated into French and transcribed. Finally, data saturation for the focus groups was reached after all participants had the opportunity to express their point of view for each discussion point.
Data analysis
Analyses were performed from thematic groupings to identify relevant emerging themes for each potential determinant of overweight/obesity (Mason, Reference Mason2002). After the identification of main themes (e.g. for social valorization of stoutness: idealization of urban abundance; for diet: urban food pleasure; and for physical activity: valorization of idleness), the main information from each theme was summarized and the social representations and practices related to these in the three area subsamples compared. NVivo 7 software (QSR International, Melbourne, Australia) was used to synthesize the main outcomes of focus group discussions.
Quantitative study
Data sample
The quantitative study sample comprised 393 adults (200 men and 193 women; 187 urban and 206 suburban subjects) from the agglomeration of Dakar (city centre and suburb) and 204 adults from the rural Kaolack region (84 men and 120 women). For both areas, a quota sampling strategy was used, according to three criteria (age, sex and neighbourhood) from the 2002 National Senegalese Census. Data for the regions investigated were provided by the Senegalese National Institute of Statistics and Demography. In the Dakar agglomeration, participants were selected from all parts of the city and its peripheral region (e.g. Sacré Coeur, Cambérène). The rural area subjects were strictly inhabitants of the three villages cited above. Pregnant women and confused elders were excluded in order to collect reliable biological and cultural data.
Perceptions of corpulence
To accurately assess body weight perceptions and identify the potential social valorization of overweight/obesity, the Body Size Scale (BSS) was used. This validated tool presents real human body size photographs of both sexes, covering the total gradient of BMI (Cohen et al., Reference Cohen, Bernard, Ponty, Ndao, Amougou, Said-Mohamed and Pasquet2015). Then, a body image assessment guide (BIAG) was built to contrast local Senegalese norms with scientific norms of body weight measured by the BSS, as employed in a previous study (Cohen & Pasquet, Reference Cohen and Pasquet2011). The BIAG consists of three questions about current body size (CBS), desired body size (DBS) and ideal body size (IBS) for oneself as well as one’s partner (for polygamous households, the first wife was included). The responses for these items were compared between participants living in urban, suburban and rural areas, to assess possible changes in corpulence norms with the urbanization process. In addition, a social valorization of overweight/obesity index was constructed from the BSS to accurately assess the desire to gain weight.
Dietary intake
To assess dietary intake, first the Dietary Diversity Score (DDS) – a qualitative 24-hour recall to assess the diversity of food group composition – was used (Savy et al., Reference Savy, Martin-Prével, Traissac, Eymard-Duvernay and Delpeuch2006). The Food and Agriculture Organization (FAO) developed the DDS, which is based on sixteen main food categories (including cereals, green vegetables, oils, meats), and have used it to assess dietary diversity in Senegal (FAO, 2011). The DDS has been observed to be a good indicator of global diet changes in the context of the nutrition transition (Oldewage-Theron & Kruger, Reference Oldewage-Theron and Kruger2008). The DDS and BMI have been found to be positively correlated in the context of staple food accessibility (Savy et al., Reference Savy, Martin-Prével, Traissac, Eymard-Duvernay and Delpeuch2006; Karimbeiki et al., Reference Karimbeiki, Pourmasoumi, Feizi, Abbasi, Hadi, Rafie and Safavi2018). Secondly, whether urbanization in Senegal involves obesogenic eating practices was also evaluated by assessing: (1) the frequency of snacking in the last 24 hours through the question: ‘Did you snack yesterday? If so, how often?’; (2) the daily frequency of snacking – the snacking average perceived by subjects – through this question: ‘How many times do you snack a day: less than once (1), once (2), twice (3), three times (4), continuously (5)?’; and (3) the desire to adopt a high-calorie diet through this last question: ‘What does it mean to you to “eat well?”.
Physical activity
To assess the duration of physical activity, four items from the International Physical Activity Questionnaire (IPAQ) were used (Craig et al., Reference Craig, Marshall, Sjoström, Bauman, Booth and Ainsworth2003). The daily averages (in hours) of intensive physical activity (digging, carrying heavy loads, intense effort, etc...), moderate physical activity (wearing light loads, gentle cycling, etc...), and walking and sedentary behaviour levels were calculated from the number of days and the duration of physical activity in the last 7 days prior to completing the questionnaire.
Health status perception
Using the BSS, a body self-satisfaction index was calculated to identify subjects as either satisfied with their body weight or wanting to gain or lose weight. This BSS index was compared with BMI categories to assess the body self-satisfaction of participants according to their body weight status.
Anthropometry
A set of anthropometric measurements was taken by trained fieldworkers using standardized procedures (Weiner & Lourie, Reference Weiner and Lourie1981). Height was measured to the nearest millimetre using a portable stadiometer (Siber Hegner, Zurich, Switzerland). Weight was measured with participants in very light clothing, to the nearest 100 g, using a digital beam scale (Tanita, Tokyo, Japan). Overweight was defined as BMI ≥25 and <30 kg/m2 and obesity by a BMI ≥30 kg/m2. Hip circumference and waist circumference were measured to the nearest millimetre in a standing position using a non-stretchable tape-measure, according to standard procedures. The waist-to-hip ratio (WHR) was calculated to assess body fat distribution (WHO, 2000). Skinfold thickness measurements (mm) were taken at four sites: biceps, triceps, suprailiac and subscapular using a Harpenden skinfold caliper (Holtain Ltd, Crymych, UK). Fat mass (body fat %) was derived from the sum of the four skinfold measures (Durnin & Womersley, Reference Durnin and Womersley1974).
In addition, two diastolic and systolic blood pressure (BP) measurements (mmHg) were taken with an electronic tensiometer (Omron France, Rosny-sous-Bois, France) from each arm, with the subjects in a seated position and after 15 minutes rest. Means of the two systolic and diastolic BPs taken from each arm were calculated. The systolic and diastolic BP means were defined as: (diastolic BP+1/3) × (systolic BP−diastolic BP). Hypertension was defined as: diastolic BP ≥90 mmHg and/or systolic BP ≥140 mmHg. This biometric protocol allowed the respondents’ nutritional status and its association with hypertension to be assessed.
Data analysis
Analysis of variance and covariance (ANOVA/ANCOVA) and t-tests (post-hoc analyses) were used to assess the anthropometric characteristics and body size standards; χ 2 and Fisher’s exact tests were used to assess the prevalence of overweight/obesity and hypertension. The average comparisons between CBS and DBS/IBS were implemented by paired t-test. Two Principal Component Analyses (PCA) and one multiple Factorial Correspondence Analysis (FCA) were used to respectively construct proxy socioeconomic and high-calorie diet indices and analyse food consumption. Finally, a binary logistic regression model was carried out to assess the risk factors for overweight/obesity using the following variables.
Socioeconomic status was determined from a proxy index of household wealth constructed using a PCA from a set of variables: e.g. owner/tenant, type of house, car/truck, mobile phone, electricity. In the total sample, the first principal component explained 40.1% of the variance with an eigenvalue of 19.7 (5.3 for the second principal component). Households were classified into three distinct groups: low, middle and high SES according to tertiles of the calculated variable from the first principal component. The migration status of subjects was deduced through the creation of a variable ‘duration of residence in urban/suburban areas’ coded into six categories: 0 years; 1–10 years; 11–20 years; 21–30 years; 31–40 years; and >40 years. Body image was assessed using the BSS, which was treated as a metric value with each human picture ranging from 1 to 9 according to increasing BMI categories. The social valorization of overweight/obesity index was constructed as 4 minus DBS, since the fifth silhouette on the scale corresponds to overweight. Then, the body self-satisfaction index was calculated by subtracting the CBS and DBS (CBS−DBS) (Williamson et al., Reference Williamson, Gleaves, Watkins and Schlundt1993). Dietary diversity was coded by: lower DDS (<7 different categories of food groups); or higher DDS (≥7 different categories of food groups). Snacking frequency was coded as: lower snacking (<3 times/day) or higher snacking (≥3 times/day). The item on the desire to adopt a high-calorie diet was coded as ‘higher-calorie diet’ for modalities suggesting an obesogenic diet (e.g. eating filling food, eating at irregular times, eating high-calorie food) and as ‘lower-calorie diet’ for the other modalities (e.g. eating a balanced diet, eating at regular hours, eating fruit and vegetables, etc.). A multiple FCA of the different items of dietary intake allowed the analysis of food consumption in the context of urbanization. In addition, a proxy high-calorie diet index was constructed using a PCA from the different items of questionnaire suggesting obesogenic dietary intake (high DDS, snacking in the last 24 hours, daily snacking and craze for high-calorie foods). The first principal component explained 31.9% of the variance with an eigenvalue of 1.3 (1.0 for the second principal component). Diet calorie level was classified into three groups (low, middle and high calorie intake) from the first principal component, which synthesized snacking practices. A physical activity index was constructed for moderate- and high-intensity physical activity as defined in the IPAQ. Physical activity was coded as: lower physical activity (0 days of moderate and intensive physical activity practised during the last week); and higher physical activity (≥1 days of moderate and/or intensive physical activity practised during the last week).
The relationships (adjusted odds ratios (OR), 95% confidence intervals (CI)) between overweight/obesity and their plausible determinants (sex, age, area living, proxy index of household income, level of education, dietary intake, social valorization of overweight/obesity index, high intensity physical activity) were assessed with a binary logistic regression model. Statistica 13 software (Statsoft Inc, Tulsa, OK, USA) was used to conduct the descriptive statistics and PCA and FCA; and MyStat 12 software (Systat Software Inc, San Jose, CA, USA) was used for the logistic regression.
Results
Qualitative study
Three major themes emerged from the focus group discussions.
Social valorization of stoutness
The development of urban areas in Senegal has created an idealization of urban abundance – an idealized conception of modern lifestyle where success is seen as possible for rural and migrant populations who idealize Western culture. Integrating into an urban lifestyle is associated with weight gain, which is scarce in the village setting, as a symbol of integration into the city, taking advantage of its abundance. But in rural areas, only a limited corpulence is valued, since high fatness is not adapted to rural labour. Hence, this social valorization of stoutness increases alongside the emerging modern lifestyle, and is seen as a symbol of wealth and prosperity. For example, one participant explained:
According to my vision of the two eras, everyone knows that at present, women intentionally overeat high-calorie food and use medication [corticosteroids]; especially for us, women…, it differs from the grandparents’ eras when they spoke of am yaram [have weight]. If you’re too rey [stout] in the village, you will not be able to work or cultivate; it’s not valued ... But women today in the city, no one knows they are taking medications [corticosteroids] that increase their overweight. (Older urban woman, high SES)
The improvement in SES that accompanies urbanization can result in weight gain, especially in middle-aged and elderly married women living in the low-SES suburbs of Dakar as they are less receptive to modern representations of body size. They generally maintain regular contact with the rural world through traditional celebrations (such as weddings), where it is important to present a ‘beautiful body’: corpulent and dressed in smart, traditional loose clothes. The experiences of younger people are different, as illustrated by this young man:
People in villages are ignorant. If you are am yaram [have weight], automatically they think that you are in good health but it is not always true! If you come back to the village after urban living, people will say: “You eat your money!” People in the regions do not see like Dakar people, they all want to come in Dakar. For them, if you migrate to Dakar, you have no more worries, you have everything you want; whereas in Dakar, firstly we do not always eat well, secondly, times get tough. Thus, a woman who returned to the village am yaram [have weight] and khess [thinning skin], people said that Dakar is prosperous for you! (Younger urban man, low educational level)
Diet perceptions and practices
Inter-generational conflict has emerged between parents and youths on culinary practices, with a devaluation of traditional food among young people. Parents condemn the use of modern foods based on rice, oil, cube-maggi, meat and fast-food, whereas Westernized youths no longer appreciate traditional diets based mainly on millet and vegetables. This is illustrated by the following participant:
…. in the current situation in many homes, if you cook ngourban [millet seeds boiled and ground], children will not eat that. They will not even touch it because times are not the same. Children hardly know this diet. What they know is that you cook now to eat, and this is what causes endless damage to us. What would be safer for us are alternatives, but cooking with oil as we do for ceebu jën [rice with fish], that’s not good. With that, we cannot expect to have a healthy body. (Older rural man)
The urbanization process is perceived as the era of comfort and pleasure – ‘urban food pleasure’. Therefore, it is not possible for Westernized youth to accept eating ‘simple food’ just to meet basic living needs, for example:
Many people flock to Dakar because there is the atmosphere there. The diet is different. In Dakar, the food is tasty, there are sandwiches, burgers, chawarmas. Here you can go six months without eating burgers or something like that. Here you eat couscous of millet and foõdé [millet porridge with grains], that’s all. Therefore many people prefer to go to Dakar for that. They flee the food here and also the hard work in the fields. (Younger rural man)
Physical activity
A valorization of idleness in older women emerged from the focus group discussions. The social value of overweight also involves a desire to decrease daily physical activity, i.e. the practice of idleness, based on reclusion at home, regular sleep and moreover achieving ‘peace of mind’: the avoidance of worries and social pressures. During marriage, the obsession to ostentatiously demonstrate household economic success in poor urban neighbourhoods, through wives’ weight gain, involves a real change in lifestyle to become fat: the search for a simple life without stress, unnecessary actions and the desire to gain an ‘authentic weight’:
During the day I closed my door and I quietly and sufficiently slept. That’s how I gained weight. The aim, it is above all to be xel mu dal [have peace of mind]. If you take the most appropriate diet to gain weight while you are not xel mu dal, it does not work. You have to be comfortable in your head ... Sleeping the day, it’s also great to gain weight. At a certain point, all I could not have, I did not care anymore. I was trying not to break my head. Everything that could give me peace of mind, I did. (Older urban woman, high SES)
However, young people exposed to Western media and medical discourse valued physical activity, especially sport e.g. jogging or bodybuilding for men. The most Westernized young people wanted to exercise regularly to avoid weight gain:
Modern clothes require a thin body! From 6 pm, young people are at the beach doing sport to fight against the phenomenon of weight gain. Young people, especially in Dakar, tend to not want to gain weight, even for a wedding. It is old-fashioned. (Younger urban man, high educational level)
Quantitative study
Perceptions of corpulence
In all areas, men overestimated their body size (Table 3; Fig. 1), and perceived themselves to be in the normal weight category. Those living in urban and rural regions showed a significantly greater desire than those living in suburban region to increase their body weight and become overweight (CBS vs DBS: p<0.01 and p<0.001, respectively). Further, participants from all regions selected a DBS and IBS in the normal weight category, while the suburban group had the lowest DBS and IBS averages and the highest CBS average. In the urban and rural groups IBS was significantly higher than CBS (p<0.001), but not in the suburban group.
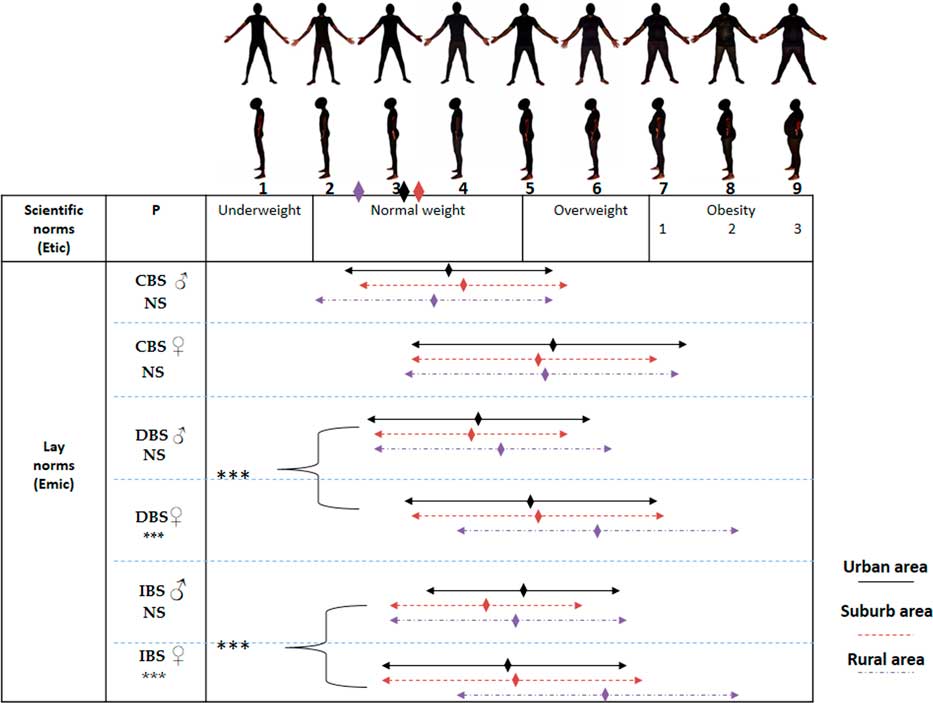
Figure 1 Perceptions of body size on the male Body Size Scale by sex and area of residence. The diamonds just below the silhouettes correspond to the BMI averages of the three areas (see Table 2). CBS: Current Body Size; DBS: Desired Body Size; IBS: Ideal Body Size.
Table 3 Current, desired and ideal body size by area of residence

Analysis of variance between the three areas: *p<0.05; **p<0.01; ***p<0.001.
Post-hoc analyses between the three samples: a<0.05; b<0.01; c<0.001.
CBS: current body size; DBS: desired body size; IDS: ideal body size; SD: standard deviation; NS: not significant.
All women perceived their partners to be in the overweight category (Table 3; Fig. 1); however, only rural women indicated that they wanted them to gain weight to be overweight (p<0.01). Both urban and suburban women showed a slight preference for their partner to lose weight. Rural women preferred both DBS and IBS in the overweight category, whereas urban/suburban women had a preference for DBS and IBS in the normal weight category (p<0.001). The male IBS of the urban women group was significantly lower than the CBS for their partner (p<0.05) and lower, but not significantly so, in the suburban group. Conversely, male IBS was significantly higher than the CBS for the partner of rural women (p<0.001). Finally, the DBS and IBS of men for themselves were significantly lower than those of women for men (p<0.001).
Concerning women’s perceptions (Table 3; Fig. 2), only suburban and rural groups overestimated their own weight. Women in the urban and suburban groups perceived themselves to be in the overweight category, whereas rural women perceived themselves to be in the normal weight category (p<0.001), and wanted to gain weight (p<0.001). The DBS and IBS of men for themselves were similar to those of women for men: in the overweight category, except for rural women, who clearly preferred the overweight category (p<0.001). In addition, rural women had an IBS that was significantly higher than their DBS (p<0.05) and CBS (p<0.001).
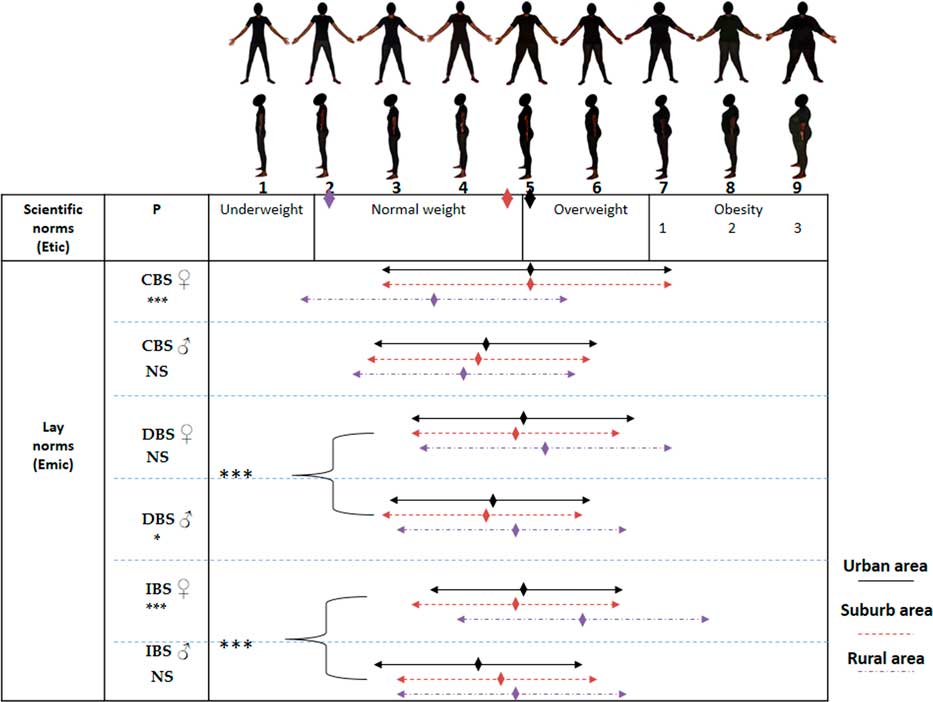
Figure 2 Perceptions of body size on the female Body Size Scale by sex and area of residence. The diamonds just below the silhouettes correspond to the BMI averages of the three populations (see Table 2). CBS: Current Body Size; DBS: Desired Body Size; IBS: Ideal Body Size.
All men perceived women to be in the normal weight category (Table 3; Fig. 2), and rural men desired their partner to gain weight (p<0.001). The IBS for women was the lowest in the urban men’s group and the highest in the rural men’s group. Rural men had a preference for a female IBS significantly higher than their partner’s CBS (p<0.01), whereas IBS and CBS were not significantly different in urban/suburban groups. Finally, the DBS and IBS of women for themselves were significantly higher than those of men for women (p<0.001).
Dietary intake
The multiple Factorial Correspondence Analysis (FCA 1, Fig. 3) of the relationship between dietary intake (high DDS, high snacking level, desire for high-calorie foods) and risk of overweight/obesity showed that middle-aged and elderly subjects adopted a lower-calorie diet than young Senegalese, even though they had a higher DDS; no dietary intake pattern was observed in this second group (p<0.001; n=597). Indeed, no point cloud demonstrating associations between youth and dietary intake variables was graphically observable. No dietary intake pattern was found with either nutritional status or region.

Figure 3 Obesogenic dietary intake by age. The FCA is between diet consumption and risk of overweight and age (young ≤25 years; others >25 years). The variables in italics followed by the sign – means a low risk while those followed by the sign + means a high risk. Dimensions 1 and 2 were retained since they captured the highest variance of the model (dimension 1: 28.8% of inertia: dimension 2: 21.7% of inertia). Dimension 1 shows a clear dietary intake pattern in older subjects (>25 years) whereas dimension 2 shows no specific dietary pattern with the variables selected.
The analyses showed a significant association between lower DDS and a rural lifestyle (49.5% vs 27.2% in urban/suburban areas, respectively, p<0.001). Adjusting for age, significant mean differences in DDS were found between urban/suburban and rural areas (8.7±1.8 in urban area, 8.6±1.8 in suburban area and 7.5±1.8 in rural area, p<0.001). In addition, a significant association was found between higher daily snacking and urban/suburban lifestyle (28.0% urban/suburban area vs 16.2% in rural area, p<0.01) and younger age (39.0% in younger subjects vs 17.7% in older subjects, >25 years; p<0.001). However, higher daily snacking was not associated with overweight/obesity among young subjects (≤25 years). Finally, higher daily snacking was associated with young (48.6% vs 20.0% in older subjects, ≤25 years) and young/middle-aged subjects (34.8% vs 0.07% in older subjects, ≤45 years) living in both urban and suburban areas (p<0.001 for both groups).
Physical activity
Durations of moderate and high-intensity physical activities were lower in suburban than in rural areas (Table 4, p<0.001). Moderate physical activity was higher in rural than urban area (p<0.001), and high-intensity physical activity was higher in urban than suburban area (p<0.05), and close to the level of the rural average. The level of sedentary behaviour was highest in the urban area and lowest in the rural area (p<0.001). There was no significant difference in walking averages. Univariate analyses showed a significant association between younger age (≤25 years) and regular moderate and/or intensive physical activity (p<0.01) in both urban and suburban areas. The same pattern of results was found in young and middle-aged subjects (≤45 years; p<0.001) since 61.1% of them practised regular moderate and/or intensive physical activity against 30.9% in older subjects (>45 years) living in urban/suburban areas.
Table 4 Physical activity levels by area of residence

Age adjusted by covariance analyses.
ANCOVA between the three samples: *p<0.05; **p<0.01; ***p<0.001.
Post-hoc analyses between the three samples: a<0.05; b<0.01; c<0.001; x: no significant (NS) for each side-by-side comparison.
Anthropometry
In urban/suburban areas, women were fatter and had lower mean BP values than men (Table 5). In both sexes, groups from both urban and suburban areas had higher anthropometric indices than those from rural areas, except for mean BP in both sexes. Hip circumference was significantly higher in men living in suburban areas compared with those living in urban settings. Similar trends were found for BMI and waist circumference, but these were not significant. No significant differences were found for mean BP between areas in both sexes.
Table 5 Anthropometric characteristics of participants (mean±SD) by area of residence

Age adjusted by covariance analyses.
ANCOVA between the three samples: *p<0.05; **p<0.01; ***p<0.001.
Post-hoc analyses between the three samples: a<0.05; b<0.01; c<0.001; x: NS for each side-by-side comparison.
SD: Standard Deviation; n=urban/suburban/rural sample sizes.
The prevalences of overweight and obesity in the total sample were significantly higher in urban/suburban than rural areas: respectively 29.6 vs 8.5% for overweight (χ 2, p<0.001) and 11.8 vs 2.0% for obesity (Fisher’s exact test, p<0.001). In addition, 5.8% of young subjects (≤25 years), 23.0% of middle-aged subjects (25–45 years) and 40.5% of older subjects (χ 2, >45 years; p<0.001) were overweight/obese; and 2.9% of young subjects (≤25 years), 7.4% of middle-aged subjects (25–45 years) and 16.9% of older subjects (χ 2, >45 years; p<0.001) were obese. For hypertension, a significant difference between urban/suburban and rural areas was only found in young people (≤25 years): 15.6% vs 6.1% (Fisher’s exact test, p<0.05). Finally, significant associations were observed between overweight/obesity (aggregated) and hypertension (48.9% in overweight/obese vs 19.3% in underweight/normal weight subjects, χ 2, p<0.001).
Migration and nutritional status
A significant association was observed between overweight/obesity and length of residence in urban/suburban areas (χ 2, p<0.001). The percentage of overweight subjects was found to strongly increase after 30 years of urban/suburban residence (Fig. 4). No association between urban/suburban length of stay and overweight/obesity in rural Senegalese was found since none of them lived in a city.
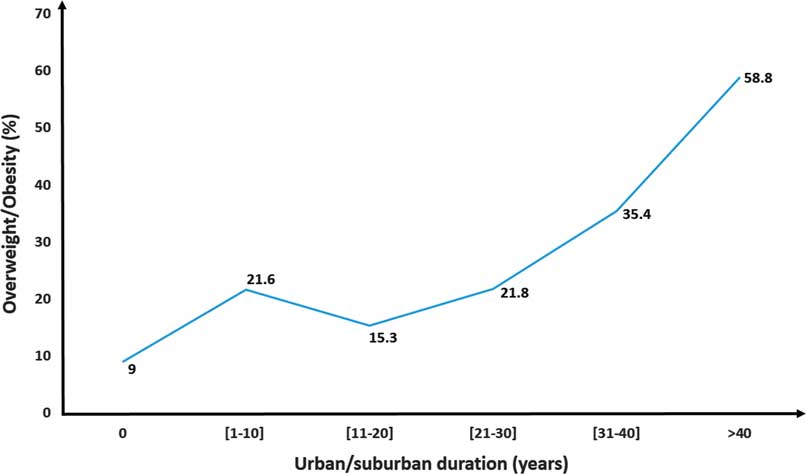
Figure 4 Prevalence of overweight/obesity and migration status. The respective count of overweight/obese subjects for each prevalence was: 9% (n=17 overweight/obese subjects), 21.6% (n=8), 15.3% (n=9), 21.8% (n=22), 35.4% (n=28) and 58.8% (n=30).
Health status perceptions
Using the body self-satisfaction index, it was observed that 52% of overweight/obese subjects were satisfied with their weight status versus 13.5% of underweight/normal weight subjects (p<0.001). The majority of subjects who wanted to gain weight were over 25 years old (62.0%; p<0.05). Using the social valorization of overweight/obesity index, it was observed that the majority of subjects who valued overweight and obesity were women (60.2%; p<0.001) and those aged over 25 years (74.1%; p<0.05). However, the difference in overweight valorization between age groups was only significant in women (younger/older women: 44.6% vs 65.5%, p<0.01; and younger/older men: 43.0% vs 42.4%).
Analysis of determinants of overweight/obesity
In the binary logistic regression model, the comparison of overweight/obese (BMI ≥25 kg/m2) with non-overweight (BMI <25 kg/m2) subjects revealed an independent negative effect of a calorific diet, and independent positive effects of sex, age, area of residence and the social valorization of overweight/obesity (Table 6). The risk of being overweight/obese was 3.6 times higher in women than in men (p<0.001). Overweight/obesity increased with age (p<0.001) and urbanization (p<0.001). Indeed, the risk of being overweight/obese was 6.5 times higher in both urban/suburban areas than in the rural area. Overweight/obesity increased with the social valorization of overweight/obesity (p<0.05): the risk of being overweight/obese was 1.7 times higher among subjects who valued overweight/obesity than those who did not. Finally, univariate analyses showed that high SES was more likely to be associated with being overweight/obese (p<0.05), and the more likely that participants participated in moderate and/or high intensity physical activity, the less likely they were to be overweight/obese (p<0.001).
Table 6 Binary logistic regression analysis of overweight and obese participants compared with subjects who are not (N=561)
Crude analysis, significant effect: *p<0.05; **p<0.01; ***p<0.001.
In bold, significant binary logit analysis effects: a p<0.05, b p<0.01, c p<0.001.
Ref.: reference category.
Discussion
This mixed-methods study investigated the biocultural determinants of overweight and obesity in Senegal to provide a holistic understanding of the physical and sociocultural (biocultural) aspects of the Senegalese nutrition transition and to clearly identify the transitional stage being experienced by the country. Overall, despite the relative low prevalence of overweight and obesity in the Dakar agglomeration, it was found that the Senegalese have experienced health consequences related to lifestyle transition. More precisely, the internal migration from rural to urban/suburban areas was found to be associated with a dynamic social-ecological obesogenic context: a higher urban/suburban prevalence of overweight/obesity and hypertension, and a valorization of stoutness, sedentary behaviours and higher SES, exposing people to overweight/obesity.
For urban/suburban Senegalese, urbanization, and other specific biocultural factors, has created higher exposure to overweight/obesity, as identified in the study’s binary logistic regression analysis. This has been observed in other populations who migrated to urban areas of low- and middle-income countries, such as Gambia and Botswana (Siervo et al., Reference Siervo, Grey, Nyan and Prentice2006; Letamo, Reference Letamo2011). In addition, the nutrition transition seems to be more evident in urban/suburban Senegalese women, who had a mean BMI of around 25 kg/m2, as found by Macia et al. (Reference Macia, Gueye and Duboz2016). The present data support the hypothesis that women in low- and middle-income countries are more sensitive to the obesogenic effects of nutrition transition in urban areas, as has been observed in other African countries, even though the Senegalese prevalence of overweight/obesity remains relatively low (Monteiro et al., Reference Monteiro, Conde, Lu and Popkin2004; Fezeu et al., Reference Fezeu, Assah, Balkau, Mbanya, Kengne, Awah and Mbanya2008).
In spite of the social valorization of stoutness in traditional Senegalese culture, as accentuated by the current lay portrayal of Dakar as an ‘El Dorado’, this appears to be decreasing in the urban and suburban areas, particularly among young women. The Senegalese population seem to adapt their body size norms to the obesogenic urban environment and modern perceptions of body size, like other African populations experiencing internal migration in South Africa and external migration to Western countries (Szabo & Allwood, Reference Szabo and Allwood2006; Renzaho et al., Reference Renzaho, McCabe and Swinburn2012). Indeed, the younger study participants devalued overweight and obesity, unlike older participants, as identified in a Cameroonian rural–urban study (Dapi et al., Reference Dapi, Omoloko, Janlert, Dahlgren and Håglin2007). Thus, in the Dakar agglomeration, both desired and ideal body size were approximately ‘overweight’, especially in middle-aged and older women, as observed in other African urban areas such as Kumasi, Ghana (Appiah et al., Reference Appiah, Otoo and Steiner-Asiedu2016); whilst the prevalences of overweight, obesity and hypertension were higher than in the rural area, as shown in South Africa (Steyn & Mchiza, Reference Steyn and Mchiza2014).
A preliminary recent Senegalese study on body image also showed a female valorization of stoutness (Cohen et al., Reference Cohen, Ndao, Faye, Ndiaye, Ndiaye and Ezan2018), but further analyses have demonstrated that women particularly valued overweight and obesity in men while most participants overestimated their weight – a trend probably linked to the traditional depreciation of thinness (Ndiaye, Reference Ndiaye2006). Hence, the binary logistic regression analysis showed the social valorization stoutness (overweight and obesity) to be an independent risk factor for overweight/obesity, as observed in previous studies conducted in Cameroon (Cohen et al., Reference Cohen, Boetsch, Palstra and Pasquet2013, Reference Cohen, Amougou, Ponty, Loinger-Beck, Nkuintchua and Monteillet2017), since the majority of overweight/obese subjects did not want to lose weight – a phenomenon already identified in urban middle-aged Senegalese women (Holdsworth et al., Reference Holdsworth, Gartner, Landais, Maire and Delpeuch2004).
Senegalese culture in the central Wolof region involves traditional culinary habits based on a low-calorie diet, essentially composed of frugal dishes of vegetables and millet, but the findings of the study’s focus group discussions suggest these culinary practices are unappreciated today, firstly by young people wanting to discover the food pleasures of the city (Ndoye & Diop, Reference Ndoye and Diop2001; Holdsworth et al., Reference Holdsworth, Delpeuch, Landais, Gartner, Eymard-Duvernay and Maire2006), and secondly by older women in suburban area intentionally over-eating and using corticosteroids to rapidly gain weight, as also observed by Rguibi and Belahsen (Reference Rguibi and Belahsen2006) in Morocco. The Dietary Diversity Score (DDS) was found to be higher in suburban and urban areas, as was the frequency of daily snacking. However, the binary logistic regression analysis found that this desire for ‘food pleasure’ was not associated with overweight and obesity among young and middle-aged subjects living in suburban and urban areas.
The DDS measure has not been found to be systematically associated with BMI (Salehi-Abargouei et al., Reference Salehi-Abargouei, Akbari, Bellissimo and Azadbakht2016). Indeed, the literature attests that DDS and BMI are positively correlated during times of guaranteed access to staple high-calorie food – which is the case in all Senegalese regions (Savy et al., Reference Savy, Martin-Prével, Traissac, Eymard-Duvernay and Delpeuch2006; Bosu, Reference Bosu2015; Karimbeiki et al., Reference Karimbeiki, Pourmasoumi, Feizi, Abbasi, Hadi, Rafie and Safavi2018). Furthermore, this result could also be explained by the ambivalent lifestyle experienced by the population. Young people exposed to a global consumer society are caught between food hedonism and the valorization of thinness (Hesse-Biber et al., Reference Hesse-Biber, Leavy, Quinn and Zoino2006), while some older people maintain a traditional diet that is not obesogenic (Ndoye & Diop, Reference Ndoye and Diop2001). Hence, the FCA showed that the dietary patterns of middle-aged and older subjects were associated with lower-calorie dietary practices, especially in rural area where daily snacking was less frequent. Moreover, the high-calorie diet index had an independent inverse association with overweight/obesity in the binary logistic regression model because snacking was mainly practised by younger people.
Moderate- and high-intensity physical activities were higher in the rural area, whilst sedentary behaviour was higher in the urban/suburban areas. Lower intensity and/or moderate physical activities were found to be associated with overweight and obesity, as also observed by Sodjinou et al. (Reference Sodjinou, Agueh, Fayomi and Delisle2008) in Cotonou, Benin. However, the association was only univariate and not significant in the binary logistic regression model. The qualitative study showed that middle-aged and older women value sedentary behaviour to ostentatiously gain weight – a symbol of peace of mind and prosperity – as observed in other studies conducted in Africa such as Morocco (Rguibi & Belahsen, Reference Rguibi and Belahsen2006; Warnier, Reference Warnier2009). Young people valued physical activity more, especially sports such as jogging. However, an urban lifestyle does not make regular physical activity easy, mainly due to office work times and the decreased need for manual agricultural activity (Besharat Pour et al., Reference Besharat Pour, Bergstrom, Bottai, Kull, Wickman, Hakansson, Wolk and Moradi2014).
As found for many African populations, the Senegalese who have migrated have a greatest risk of developing overweight/obesity (Agyemang et al., Reference Agyemang, Addo, Bhopal, Ade and Stronks2009), even if they are receptive to etic standards (scientific norms) of corpulence, and questioning of the emic (lay norms) valorization of stoutness (Morris et al., Reference Morris, Leung, Ames and Lickel1999). Urban/suburban Senegalese seem to have an increased risk for hypertension related to higher overweight/obesity prevalence (Guh et al., Reference Guh, Zhang, Bansback, Amarsi, Birmingham and Anis2009), caused by biocultural factors. The present study found two components related to the urbanization process (i) a cultural component: the social valorization of overweight/obesity involving sedentary and eating behaviours to deliberately gain weight (Puoane et al., Reference Puoane, Fourie, Shapiro, Rosling, Tshaka and Oelefse2005), and (ii) an ecological component: lower moderate and intensive physical activity, as a result of a decrease in certain daily activities (frequent walking, manual work for men; intensive housework and caring for children/elders for women) and higher-calorie dietary intake and an increase in snacking, food portion sizes and the energy density of diets (Popkin & Gordon-Larsen, Reference Popkin and Gordon-Larsen2004; Duffey & Popkin, Reference Duffey and Popkin2011).
In recent history, in high-income countries obesity mainly affects lower SES groups (Popkin et al., Reference Popkin, Adair and Ng2012), particularly those living in urban areas, but it does touch all socioeconomic groups (Drewnowski, Reference Drewnowski2009). The reasons for this are complex, but include the tendency to consume a cheaper and more monotonous high-calorie diet (Sobal & Stunkard, Reference Sobal and Stunkard1989; Drewnowski, Reference Drewnowski2009). Indeed, besides greater accessibility of this food for the working class living in poor urban neighbourhoods, there is some evidence of a cultural explanation – the phenomenon of ‘social revenge’, i.e. a desire for the working class to discover ‘the pleasures of the city’, including ‘good food’ (Corbeau, Reference Corbeau and Valceschini1995). In some ways, the present data support other studies of African populations such as Cameroonians and South Africans (Puoane et al., Reference Puoane, Fourie, Shapiro, Rosling, Tshaka and Oelefse2005; Cohen et al., Reference Cohen, Boetsch, Palstra and Pasquet2013) since it found that the valorization of overweight, especially among middle-aged and older subjects, persists in suburban and urban areas of Senegal along with the desire for daily snacking. For instance, fattening and idleness practices were observed in middle-aged and older women, with the aim of gaining weight and to symbolize peace and success in the household. These practices are not ritualistic, nor implemented in specific venues or times, as observed in rural Mauritania and Cameroon (Sylla, Reference Sylla1985; De Garine, Reference De Garine1990; Warnier, Reference Warnier2009), because these strategies to gain weight are modern and not linked to a collective rural lifestyle, to express economic success in an urban area (De Garine, Reference De Garine1962). This can be interpreted as ‘social revenge’ by new migrants who were exposed to undernutrition in their rural areas of origin (Doak et al., Reference Doak, Adair, Bentley, Monteiro and Popkin2005), and who want to discover the nutritional abundance of Dakar. Nevertheless, this phenomenon does not have the same consequences in all ages. Young people value a processed, high-calorie diet but not body fat, unlike middle-aged and elderly people. Besides, by eating an obesogenic diet, young people, unlike older age groups, tend to undertake regular moderate and/or high-intensity physical activity in order to maintain a thin body (Baller, Reference Baller and Goerg2007; Neveu Kringelbach, Reference Neveu Kringelbach2007).
The study found that Senegal is at an earlier stage of nutrition transition than other African countries such as South Africa and Gabon, there being an association between higher SES and overweight/obesity, low mean BMI, low rural dietary diversity (as measured by the DDS) and lack of association between dietary diversity and overweight/obesity. This contradicts the findings of Abrahams et al. (Reference Abrahams, Mchiza and Steyn2011), who considered Senegal to be at an advanced stage of nutrition transition. Indeed, the socioeconomic model of nutrition transition attests that during the emergence of industrialization, rural populations have low socioeconomic conditions and suffer from undernutrition, whereas urban populations improve their socioeconomic status and adopt higher-calorie diets and sedentary behaviours and therefore gain weight (Sobal & Stunkard, Reference Sobal and Stunkard1989). However, in urban/suburban areas of Senegal, higher SES was not found to be associated with overweight/obesity, implying that the current stage of nutrition transition in Senegal is not specifically associated with wealth but rather the industrialization of lifestyle and the valorization of stoutness (Ziraba et al., Reference Ziraba, Fotso and Ochako2009). Urban Senegal allows access to a more abundant, high-energy and diversified diet – essential conditions for the nutrition transition (Popkin & Gordon-Larsen, Reference Popkin and Gordon-Larsen2004), and these are less accessible in villages inside the Sahel, and can be positively perceived by rural and migrant populations as the ‘lifestyle of abundance’.
The Senegalese living in Dakar are exposed to both physical and social obesogenic pressures. Duration of urban residency has been shown to be a risk factor for overweight and obesity due to the adoption of urban obesogenic behaviours influenced by cultural values (Olszowy et al., Reference Olszowy, Pomer, Dancause, Sun, Silverman and Lee2015; Cohen et al., Reference Cohen, Amougou, Ponty, Loinger-Beck, Nkuintchua and Monteillet2017). Indeed, urban Senegalese still value inappropriate overweight, ill-adapted to the urban ecosystem, and have adopted higher-calorie diets and abandoned regular physical activity. More precisely, urban-dwelling middle-aged and older women tend to value overweight and have lower physical activity levels compared with younger people, who snack more frequently – an obesogenic dietary practice if they reduce their physical activity.
The study observed that the diet of urban middle-aged and older women has been influenced by the nutrition transition, even though the DDS only captured this dietary intake change in young adults. Other tools such as frequency food questionnaires, 24-hour recalls or food portion guidelines could better assess the changes in dietary patterns and its association with nutritional health status (Dop et al., Reference Dop, Gomis, Gourdon and Lesauvage2003; Amougou et al., Reference Amougou, Cohen, Mbala, Grosdidier, Bernard, Said-Mohamed and Pasquet2016). Although the assessment of food consumption was limited, the findings suggest that public health policies for overweight/obesity prevention need to be adapted to the specificities of migrant populations (Delavari et al., Reference Delavari, Farrelly, Renzaho, Mellor and Swinburn2013, Reference Delavari, Sonderlund, Mellor, Mohebbi and Swinburn2015). More precisely, these policies should account for the evolving biocultural determinants of overweight and obesity in different socio-ecological areas in Senegal and other African countries (Himmelgreen et al., Reference Himmelgreen, Pérez‐Escamilla, Martinez, Bretnall, Eells, Peng and Bermúdez2004; Abraido-Lanza et al., Reference Abraido-Lanza, Armbrister, Florez and Aguirre2006).
In conclusion, although the nutrition transition is currently underway in Senegal’s urban/suburban areas, this study demonstrates that migration can modify the joint influence of biocultural drivers on overweight and obesity during the shift from rural to urban areas, accelerated by the urbanization process. Comparative studies of migrants in other African countries experiencing urbanization and the nutrition transition are required to determine how generalizable this trend is. Local and global health policies need to account for the anthropological specificities of migration pathways, to identify the exposure levels of rural–urban migrants to the risk of overweight and obesity.
Acknowledgments
Emmanuel Cohen is supported by the South African DST/NRF Centre of Excellence in Human development. Particular thanks go to Luisa Michelotti and others investigators in the field.
Ethical Approval
All procedures were approved by the National Ethics Committee for Health Research of Senegal protocol SEN13/67, No. 0272. Verbal consent was obtained from subjects, after being fully informed of the study process. Participants with elevated BP were referred for further assessment.
Conflicts of Interest
The authors have no conflicts of interest to declare.
Funding
This research received no specific grant from any funding agency, commercial entity or not-for-profit organization.










