


Introduction
Attention deficit hyperactivity disorder (ADHD) is characterised by developmentally inappropriate and impairing inattention, hyperactivity and impulsivity. It often begins in childhood and frequently persists into adulthood. ADHD often co-occurs with mental health conditions (MHCs) (e.g. anxiety, depression, substance misuse, personality disorder), and other neurodevelopmental disorders (e.g. dyslexia, dyspraxia, autism spectrum disorder). The worldwide prevalence of ADHD is around 5% in children and adolescents, and 3–4% in adults (Faraone et al. Reference Faraone, Asherson, Banaschewski, Biederman, Buitelaar, Ramos-Quiroga, Rohde, Sonuga-Barke, Tannock and Franke2015). Treatment of adult ADHD is uncommon in Europe (Asherson et al. Reference Asherson, Buitelaar, Faraone and Rohde2016), yet ADHD poses a significant socio-economic burden. For instance, the lifetime cost of illness for a child born in England diagnosed with ADHD is estimated at around £102 135 (Khong, Reference Khong2014). This figure breaks down into costs associated with healthcare (£22 315), education (£45 075) and reduced earnings from employment (£34 745). This means that for every cohort of children born in England each year diagnosed with ADHD, the total mean lifetime cost of illness per annum is around £1 billion. The cost of education is clearly not far removed from the combined costs of healthcare and reduced earnings.
Under the Disability Act 2005 (Ireland) and the Equality Act 2010 (United Kingdom), ADHD is classified as a disability. These Acts stipulate that equality for disabled students, including those with ADHD, means adapting the way that institutions of higher education (HEIs) are structured by removing systemic barriers and/or providing extra support. HEIs have a legal duty to put in place ‘reasonable adjustments’, that enable disabled students to have access to everything that makes it possible to fully engage in their studies. Table 1 lists the potential range of education-related problems and reasonable adjustments for university students with ADHD. In the United Kingdom, there is no prevalence estimate for ADHD in higher education. This is not the case in Ireland where categories of disability are much broader than in the United Kingdom. For instance, in 2015, the UK Department for Business, Innovation and Skills (BiS) (2015), published an equality analysis of disabled students’ allowance. A pie-chart was used by BiS to depict percentages of disabled first year undergraduate (UG) university students in 2013/2014 (Fig. 1). This pie-chart shows that 49% of disabled students declared a specific learning difficulty (SpLD), 13% declared a MHC and 3% declared a social communication/autistic spectrum disorder (ASD). Nothing is shown for ADHD. The second pie-chart in Fig. 1, shows the percentages of students who declared a disability at 27 universities in Ireland (AHEAD, 2016). In Ireland and the United Kingdom, similar percentages of students declared a SpLD, MHC and social communication/ASD (Aspergers/autism in Ireland). However, separate percentages for dyspraxia/dysgraphia (developmental co-ordination disorder (DCD)) (3%) and attention deficit disorder (ADD)/ADHD (3.8%) are shown for university students in Ireland.
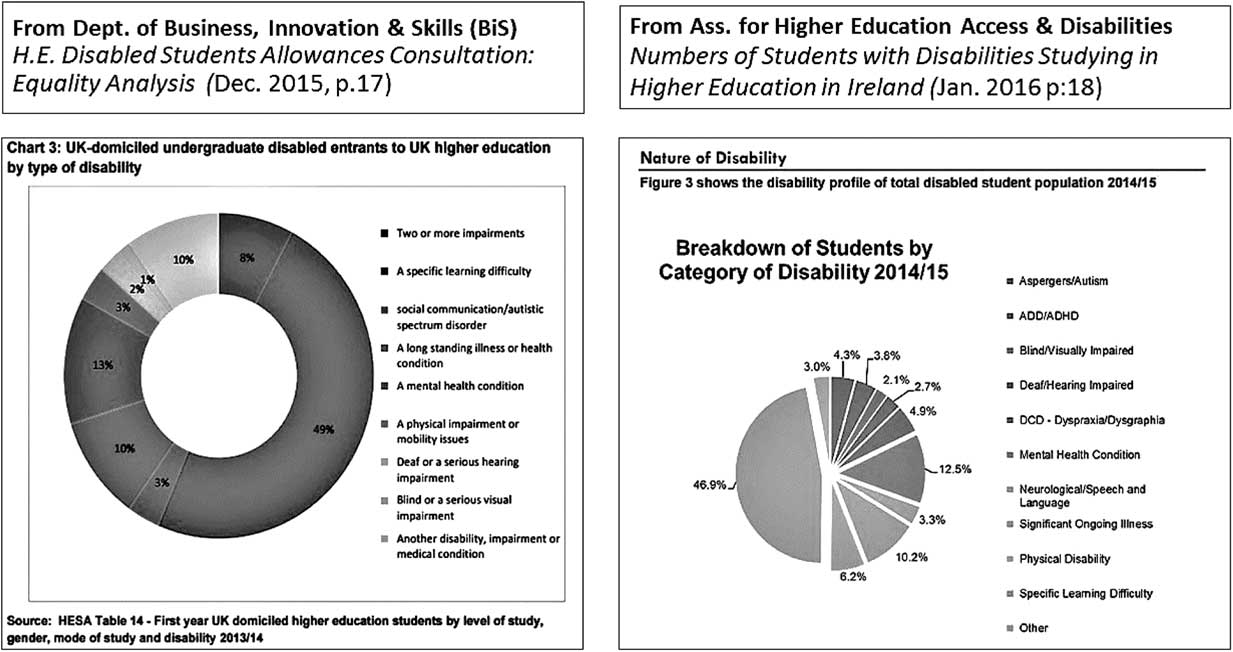
Fig. 1 Disabled university students in the United Kingdom and Ireland. ADHD, attention deficit hyperactivity disorder.
Table 1 Potential range of education-related problems and reasonable adjustments

ADHD, Attention deficit hyperactivity disorder.
The percentage of 3.8% (n=413) for ADD/ADHD among university students in Ireland, accords well with the prevalence rate of 3–4% for ADHD in adults (Faraone et al. Reference Faraone, Asherson, Banaschewski, Biederman, Buitelaar, Ramos-Quiroga, Rohde, Sonuga-Barke, Tannock and Franke2015). Research also estimates that in about 50% of cases, ADHD co-occurs with SpLDs, MHCs, DCD and ASD (Kessler et al. Reference Kessler, Adler, Barley, Biederman, Conners, Demler and Zaslavsky2006; Germanò et al. Reference Germanò, Gagliano and Curatolo2010; DuPaul et al. Reference DuPaul, Weyandt, Rossi, Vilardo, O’Dell, Carson, Verdi and Swentosky2013). In Ireland, 10 733 university students declared a disability in 2014/2015, and 7544 in total declared a SpLD, MHC, DCD or ASD (AHEAD, 2016). If the ADHD comorbidity estimate of 50% is applied to this figure, and added to the 413 recorded cases for ADHD, then a total of about 4185 university students could have had ADHD. In 2014/2015 there were a total of 113 073 university students studying in Ireland (Higher Education Authority, 2014/2015). If a 4% prevalence estimate is applied to this figure, then potentially 4548 university students could have had ADHD. This figure does not differ greatly from 4185. In the United Kingdom, 673 185 first year UG and postgraduate university students were recorded as having ‘no known disability’ in 2014/2015, while 53 795 declared a SpLD, MHC or ASD (Higher Education Statistical Agency, 2014/2015). If a prevalence estimate of 4% is applied to the figure of 673 185, and the ADHD comorbidity estimate of 50% is applied to the figure of 53 795, it is interesting that both calculations suggest about 27 000 university students could have had ADHD. This analysis, in essence, highlights that the categorisation of ADHD as a SpLD within UK HEIs maybe causing ADHD to be a hidden disability (Young et al. Reference Young, Fitzgerald and Postma2013). A possible mis-or-under diagnosis of ADHD could also be happening within HEIs in Ireland. Often this is a problem in adults with ADHD (Asherson et al. Reference Asherson, Buitelaar, Faraone and Rohde2016).
Method
A framework for scoping studies was used as a guide to identify, select, collate and review relevant publications in this topic area (Arksey & O’Malley, Reference Arksey and O’Malley2005). This framework tends to be used to rapidly map and synthesise pertinent publications in a topic area that has yet to be extensively reviewed (Mays et al. Reference Mays, Roberts and Popay2001). A combination of key words: ADHD; ADD; college students; university students; higher education; academic functioning and educational outcomes, were used to search the electronic databases PubMed, ScienceDirect and Google Scholar, for publications between 2001 and 2016. Titles and abstracts were initially screened and publications that matched the topic area were selected for review. Publications relating to assessment and diagnostic issues, school children and adolescence with ADHD, were excluded from this review. The reference lists of some publications, including anecdotal sources were also searched for additional information. Content analysis was applied to the selected publications. This method is often used to systematically retrieve meaningful data from written texts, categorise the data under core themes and produce a meaningful report of the results (Hodder, Reference Hodder1994). The search and selection strategy is shown in Fig. 2.

Fig. 2 Search and selection strategy for relevant studies.
Results
A total of 74 publications were selected for review. These publications were read, summarised and the findings were categorised under six core themes titled: academic, social and psychological functioning (ASP), giftedness, new media technologies (NMTech), treatment, substance misuse and non-medical use of stimulant prescriptions, and malingering. These six core themes represent the findings of this literature review. Each theme is outlined and critically discussed with reference to pertinent literature.
ASP (Academic, Social and Psychological)
Studies about the ASP functioning of university students with ADHD, tend to focus on academic achievement (test scores) and academic performance (final grades, length and level of educational attainment, drop-out rates), social and romantic relationships, psychological and emotional functioning. In one systematic review, Arnold et al. (Reference Arnold, Hodgkins, Kahle, Madhoo and Kewley2015), reported on a number of studies that examined academic achievement and performance among university students with ADHD. This review found that this group of students tended to do poorly in academic tests and overall performance when compared with non-ADHD peers. Their academic outcomes seemed to improve significantly with treatment, especially multi-model treatment. However, the type of treatment and educational strategies for improving the educational outcomes of university students with ADHD is an area that requires further research (Birchwood & Daley, Reference Biederman, Faraone, Spencer, Mick, Monuteaux and Aleardi2012; Rodger et al. Reference Rodger, Wilson, Roberts, Roulstone and Campbell2015).
In another study, Pope (Reference Pope2010) investigated the incidence of ADHD symptoms in full-time UG psychology students and the impact ADHD had on their academic achievement. A total of 464 students (F=362; M=102), completed the short-version CAARS (Conners’ Adult ADHD Rating Scale) and final scores were compared against their average percentage marks on completion of degree. Findings revealed that 106 students were rated as having ADHD (n=65 inattentive sub-type; n=24 hyperactivity/impulsivity sub-type; n=17 combined sub-type). None of these students had previously been diagnosed with ADHD. A total of 363 students graduated as expected, while 88 students failed to graduate for a number of reasons, including 13 students who submitted extenuating circumstances. Students rated as having ADHD inattentive sub-type were less likely to graduate, whereas hyperactivity/impulsivity sub-type did not seem to affect graduation status. Higher hyperactivity/impulsivity scores were reported more by male rather than female students. Other studies also associate ADHD inattentive sub-type with poor academic functioning (Rabiner et al. Reference Rabiner, Anastopoulos, Costello, Hoyle, McCabe and Swartzwelder2008; Weyandt & DuPaul, Reference Weyandt and DuPaul2008), but it was not clear if Pope (Reference Pope2010), observed a similar outcome for students rated as having ADHD combined sub-type. The CAARS tends to have good psychometric properties (Kooji et al. Reference Kooji, Boonstra, Swinkels, Bekker, de Noord and Buitelaar2008), but the ethnic minority status of the students in Pope’s study needed to be reported. It is an important consideration when using the CAARS, as normative studies did not report on its applicability with ethnic minority groups (Macey, Reference Macey2003).
Factors that could predict academic success in university students with ADHD, which included coping strategies for managing symptoms associated with ADHD, was investigated by Kaminski et al. (Reference Kaminski, Turnock, Rosén and Laster2006). In this study, 68 students aged between 18 and 23 years old (F=29; M=39; n=64), enrolled at one top university in the United States were recruited as participants. These students were classified as high-success (HS), or low-success (LS) academic performers, depending on their grade point average scores. Participants completed a range of standardised measures, including the Coping Resources Inventory for Stress. The findings of this study focused on strategies for coping with ADHD, obstacles to academic success and sources of motivation. The participants reported coping strategies such as: working longer and harder than others; getting social support; using good organisation, time management and study skills; exercise; a positive mental attitude; spirituality/religion or meditation; self-awareness/therapy; fidgeting; being a perfectionist; self-acceptance and manipulating others or the ‘system’. The obstacles to success were reported as: procrastination; not using organisational, time management and study skills; peer pressure to socialise instead of study; lack of time to study and being a perfectionist. Sources of motivation were reported as: to make others proud; not let others down; long-term career goals; not let myself down; prove to others (who said I would fail) that I can succeed; fear of failure; competition with peers; stress associated with procrastination and long-term financial goals.
Kaminski et al. found that a range of factors predicted academic success. Academic coaching tends to focus on similar aspects in order to enhance academic functioning (Parker et al. Reference Parker, Hoffman, Sawilowsky and Rolands2013). Interestingly, procrastination was reported as an obstacle to success. Procrastination at times, is described as a ‘students worst enemy’ and tends to be associated with poor academic performance (Rice et al. Reference Rice, Richardson and Clark2012). In Kaminski et al.’s study the ‘stress of procrastination’ was also reported as a source of motivation. This also suggests not all ‘stress’ is bad. For instance, eustress is said to be positive or beneficial stress. It refers to how an individual perceives a stressor (negative=threat v. positive=challenge) (Fevre et al. Reference Fevre, Kolt and Matheny2006). The concept of eustress can account for why the ‘stress of procrastination’ could motivate some university students to study. Another interesting finding in Kaminski et al. study, was that certain coping strategies seemed to differentiate HS and LS students. The LS students reported better physical fitness than their HS peers. Kaminski et al. surmised that LS students may have been healthier, fitter, but less academically successful, because they spent most of their free time exercising instead of studying. None of the students reported exercise as an obstacle to success, although 10 HS students in comparison to 17 LS students, said they used exercise as a coping strategy for ADHD. Physical exercise is known to have a number of physical and mental health benefits against stress, anxiety, depression, ADHD and so on (Den Heijer et al. Reference Den Heijer, Groen, Tucha, Fuermaier, Koerts, Lange, Thome and Tucha2017). It is not surprising that university students can use exercise to cope with symptoms of ADHD. While the sample size in Kaminski et al.’s study was small and all participants were recruited at a single university, these researchers did report this as a potential methodological limitation and said generalising the findings could be problematic. However, the focus of this study on coping strategies was an important one. Other studies also find a sub-set of university students with ADHD who have positive educational outcomes, and the prevailing assumption is that these students cope better with their symptoms (Wilmshurst et al. Reference Wilmshurst, Peele and Wilmshurst2011).
In relation to social and romantic relationships, university students with ADHD have reported lower levels of social adjustment, social skills and self-esteem than their non-ADHD peers (Shaw-Zirt et al. 2005). Male university students with ADHD inattentive sub-type in particular, have reported lower numbers of steady relationships, feeling less assertive and more uncomfortable in dating situations, in comparison to male peers with ADHD combined type or without ADHD (Canu & Carlson, Reference Canu and Carlson2003). In another study, UG male and female students with ADHD did not display psychological aggression in their dating and marital relationships, but they were more likely to behave physically and sexually aggression (Therialt & Homberg, Reference Therialt and Homberg2001).
Studies about the psychological or emotional functioning of university students with ADHD seem to produce inconsistent findings. For instance, Richards et al. (Reference Richards, Rosen and Ramirez1999), examined the differences in psychological functioning among university students with confirmed ADHD (n=29), ‘self-reported only’ (SRO) ADHD (n=18), and without ADHD (n=146), at one large state university in the United States. These students completed a range of standardised rating scales, including the Symptom Checklist-90-R (SCL-90-R), which assesses a range of psychological symptoms and levels of distress associated with each symptom. The findings of the study revealed that in comparison to the students without ADHD, students with confirmed ADHD and SRO ADHD, both scored significantly higher on the SCL-90-R. This suggested that poor psychological functioning was similar in both these groups of students. Inversely, Wilmshurst et al. (Reference Wilmshurst, Peele and Wilmshurst2011) examined the self-concept and psychological well-being of UG university students with ADHD (n=17), and without ADHD (n=19), at one small private university in the United States. No difference was found between these groups on measures of self-concept and psychological well-being. The only difference related to sources of emotional and academic support, with students with ADHD seeking more support from their fathers, whilst students without ADHD, sought more support from their friends. In both studies just reported, small and non-representative samples are again an issue. The inconsistency in their findings could also be an artefact of where these studies were conducted. Socio-economic status rather than just ADHD (e.g. the rich<>poor divide in American colleges), could have been responsible for the observed findings, Socioeconomic status is an established factor that influences psychological and emotional well-being (Hacker & Marcus, Reference Hacker and Marcus2015).
Giftedness
There is research which shows that the attributes and/or behaviours of intellectually gifted students can resemble the characteristics of ADHD, other learning difficulties or disabilities including ASD, or other MHCs (Beljan et al. Reference Beljan, Webb, Amend, Web, Goerss and Olenchak2006; White & Shaw, Reference White and Shaw2011; Neihart et al. Reference Neihart, Reis, Robinson and Moon2015). This research suggests that university students with ADHD can appear easily distracted, fail to finish projects that they start or shift between activities frequently, but likewise, creative individuals have a broad range of interests fleeting from one project to another (Lahey et al. Reference Lahey, Pelham, Schaughency, Atkins, Murphy, Hynd, Russo, Hartdagen and Lorys-Vernon1988; White & Shaw, Reference White and Shaw2011; Zabelina et al. Reference Zabelina, Condon and Beeman2014). The inattentiveness of ADHD observed as day-dreaming, boredom and not listening to others, is also similar to a creative person’s tendency to mull around ideas, lose interest in one idea for another, and pay attention to their own internal thoughts and visualisations (Cramond, Reference Cramond2011). The hyperactivity of ADHD is similar to the tendency of creative people to radiate with vitality and high levels of energy (Clark, Reference Clark2002). The impulsivity of ADHD is similar to the risk taking and sensation-seeking behaviour of creative people (Cramond, Reference Cramond2011). The intense and/or sensitive temperament of ADHD is similar to the ‘drama’ of creative people, who can also come across as socially awkward just like some people with ADHD (Webb, Reference Webb1993; Silverman, Reference Silverman1994). In the literature, the ‘creative gifts or giftedness’ of people with ADHD is widely documented (Cramond, Reference Cramond2011; White & Shaw, Reference White and Shaw2011; Zabelina et al. Reference Zabelina, Condon and Beeman2014; Lee & Olenchak, Reference Lee and Olenchak2015).
The phenomenon of being intellectually gifted and/or talented plus having ADHD (or another disorder) is termed ‘twice-exceptionality (2e)’. The typical characteristics of 2e students are listed in Table 2. For Brody & Mills, students with 2e ‘could be considered the most misunderstood’ (Reference Brody and Mills1997: 292). Anecdotal evidence suggests that famous people like Alan Turing, who is accredited for helping Britain win World War II by breaking the Engima Code, could have had 2e. One British Broadcasting Corporation (BBC) News article said “Turing was accustomed to being a non-conformist. At boarding school, he refused to adapt and ignored subjects that did not interest him” (BBC News, 1999). In colloquial language, 2e is referred to as the ‘Geek syndrome’ (MIT, Reference McCabe, Knight, Teter and Wechsler2003).
Table 2 Typical characteristics of students with twice-exceptionality (adapted from: National Education Association 2006, p.7)

In one study Dare & Nowicki (Reference Dare and Nowicki2015), interviewed five parents (n=4 mothers; n=1 father), about how they discovered their children had 2e and how they experienced parenting their 2e children (n=2 females; n=3 males), aged from 11 to early 20s years old. These parents described their children as having extreme strengths and weaknesses that made schooling frustrating. These parents had to seek assistance beyond the educational system, which included paying for private assessments in order to better understand the support needs of their children. They described their parenting experiences as challenging, confusing and frustrating. This study highlighted how the interplay between exceptional strengths and weaknesses in a single young person can result in inconsistencies in academic performance, and this is an important finding.
Since ADHD can produce low results on standardised tests, 2e can be missed by educational institutions that rely on high test scores in order to identify intellectual giftedness/talent (Lee & Olenchak, Reference Lee and Olenchak2015). Inversely, students who obtain good grades but still report symptoms related to ADHD are also most at risk of not getting their ADHD diagnosed/treated (Beljan et al. Reference Beljan, Webb, Amend, Web, Goerss and Olenchak2006). It can be difficult for educationalists and clinicians to differentiate ADHD from traits of giftedness like intensity, drive, perfectionism, curiosity and impatience (Webb, Reference Webb1993; Silverman, Reference Silverman1994). Educators who are successful with 2e students advocate for appropriate and supportive educational environments that allow for these students to flourish (Davis et al. 2011). Interventions for supporting 2e students have to be personalised, targeted at meeting their strengths, focussed on developing their talent(s), while also adjusting for their disabilities (Brody & Mills, Reference Brody and Mills1997; Beljan et al. Reference Beljan, Webb, Amend, Web, Goerss and Olenchak2006). As Baum et al. state, ‘if we cannot design appropriate interventions that will nurture human potential, much of the world’s best human capital will never reach its potential’ (Reference Baum, Olenchak and Owen1998: 97).
NMTech (New Media Technologies)
Young people today, like no previous generation of young people, are totally au fait with NMTech, which includes internet-based resources like social media and video gaming. NMTech is pervasive in the lives of young people. Young adults with ADHD, for example, are found to be prone to gambling addiction (Breyer et al. Reference Breyer, Botzet, Winters, Stinchfield, August and Realmuto2009), and internet addiction in the order of online gaming, chatting, down-loading, e-mailing and pornography (Yen et al. Reference Yen, Ko, Yen, Wu and Yang2007). The severity of ADHD symptoms in a sample of Turkish university students was found to predict the severity of internet addiction (Dalbudak & Eren, Reference Dalbudak and Eren2014). NMTech can be adapted for positive use in educational environments, but some researchers posit a correlation between NMTech overuse among young people and observed deficits in executive function (EF) that may account for a rise in ADHD-related behaviours (Rideout et al. Reference Rideout, Foehr and Roberts2010). ADHD is not a definitive disorder and its associated behaviours (e.g. aggression, delinquency, substance misuse) are said to exist on a continuum of ‘ADHD-related behaviours’ (Larson et al. Reference Larson, Russ, Kahn and Halfon2011).
Young people who exhibit extreme ADHD-related behaviours could have a range of problems associated with oppositional defiance disorder and conduct disorder (Pringsheim et al. Reference Pringsheim, Hirsch, Gardner and Gorman2015), as well as academic under achievement (Daley & Birchwood, Reference Daley and Birchwood2010). In one study, Nikkelen et al. (Reference Nikkelen, Vossen, Valkenburg, Velders, Windhorst, Jaddoe, Hofman, Verhulst and Tiemeier2014), examined the relationship between genetic disposition, exposure to media violence and ADHD-related behaviours. While the findings did suggest that excessive NMTech use could precipitate ADHD-related behaviours, conversely, young people who already exhibit ADHD-related behaviours could be overusing NMTech in attempts to nourish their desire for stimulation (Nikkelen et al. Reference Nikkelen, Vossen, Valkenburg, Velders, Windhorst, Jaddoe, Hofman, Verhulst and Tiemeier2014). Research on the relationship between NMTech and ADHD-related behaviours remains inconclusive. But it is still useful to consider the role of NMTech in the lives of university students with ADHD, especially when assessing their learning support and/or treatment needs.
Treatment
First-line treatment for ADHD is stimulant medication, usually methylphenidates like Ritalin. The safety and efficacy of stimulant medication in treating children with ADHD has been demonstrated (Bolea-Alamañac et al. Reference Bolea-Alamañac, Nutt, Adamou, Asherson, Bazire, Coghill, Heal, Müller, Nash, Santosh, Sayal, Sonuga-Barke and Young2014), yet diagnosis and treatment of adults with ADHD remains controversial in many European countries (Kooji et al. Reference Kooji, Bejerot, Blackwell, Caci, Casas-Brugué, Carpentier, Edvinsson, Fayaad, Foeken, Fitzgerald, Gaillac, Ginsberg, Henry, Krause, Lensing, Manor, Niederhofer, Nunes-Filipe, Ohlmeier, Oswald, Pallanti, Pehlivanidis, Ramos-Quiroga, Rastam, Ryffel-Rawak, Stes and Asherson2010). This is interesting in light of a study about the efficacy of psychiatric drugs in relation to common medical drugs, which found that ADHD medications are the most efficacious of all medical drugs (Leucht et al. Reference Leucht, Hierl, Kissling, Dold and Davis2012). Research about the efficacy of treatment in university students with ADHD is rare and the extent to which psychiatrists consider the unique demands of university life when prescribing medication regimes for students is unknown (Rabiner et al. 2009 Reference Rabiner, Anastopoulos, Costello, Hoyle, McCabe and Swartzweldera ). University students with ADHD who do take medication report improvements in their note taking, scores on quizzes, writing output and homework completion (Advokat et al. Reference Advokat, Lane and Luo2011). In one controlled, cross-sectional study that investigated the effects of medication on cognition in adults with ADHD, findings revealed that those taking medication had significantly better scores on IQ tests when compared with adults with ADHD who were not being treated (Biederman et al. Reference Birchwood and Daley2012).
Shire Pharmaceuticals conducted the first randomised controlled trial to test the efficacy of Vyvanse (lisdexamfetamine dimesylate), with a sample of 24 university students diagnosed with ADHD (DuPaul et al. Reference DuPaul, Gormley and Laracy2012). The drug was administered to these students over a 5-week period and large reductions in ADHD symptoms were observed, with subsequent improvements in task management, planning, organisation, use of study skills and working memory. While the short duration of this study did preclude an assessment of longer-term outcomes in academic functioning, in other studies university students with ADHD who take stimulant medication reported that it helps them academically (Advokat et al. Reference Advokat, Lane and Luo2011). However, a substantial number of these students also do not take their medication as prescribed (Rabiner et al. 2009 Reference Rabiner, Anastopoulos, Costello, Hoyle, McCabe and Swartzweldera ). One reason for this is when and how much medication is taken by a student with ADHD, seems dependent on what academic tasks need to be completed at a particular time (DeSaints et al. Reference DeSaints, Webb and Noar2008). This may also imply that additional investigations of “pro-re-nata” (PRN) use of stimulant medication amongst university students with ADHD could be indicated (Greely et al. Reference Greely, Sanakian, Harris, Kessler, Gazzaniga, Campbell and Farah2008).
No research about the efficacy of psychological treatments for university students with ADHD was found. Weiss et al. (Reference Weiss, Safren, Solanto, Hechtman, Rostain, Ramsay and Murray2008), conducted a review of the literature on psychological treatments for adults with ADHD. Out of 1419 articles only five were empirical studies that suggested psychological interventions were useful. This review highlighted a disproportionate emphasis on medication as the treatment choice for adults with ADHD, and recommended the development of more psychological interventions. Some studies do suggest the use of cognitive behavioural therapy (CBT) for university students with ADHD, because it has shown effectiveness in adults with ADHD for treating maladaptive and self-critical thinking processes (Ramsay & Rostain, Reference Ramsay and Rostain2006; Young & Bramham, Reference Young and Bramham2012; Pettersson et al. Reference Pettersson, Söderström, Edlund-Söderström and Nilsson2017). Academic coaching could be another useful intervention for university students with ADHD, but it is difficult to define it as a psychological treatment. Passmore stated that ‘coaching has become a recognized intervention, but sadly there are still no standards or licensing arrangements which are widely recognized. Professional bodies have continued to develop their own standards, but the lack of regulation means anyone can call themselves a coach. Whether coaching is a profession which requires regulation, or is professional and requires standards, remains a matter of debate’ (Reference Passmore2016: 3).
Nonetheless, academic coaching could help university students with ADHD to identify goals, develop study plans and strategies for achieving these plans, as well as monitoring progress towards attaining them – it can foster self-determination (Prevatt et al. Reference Prevatt, Lampropoulos, Bowles and Garrett2011). In one study, coaches helped university students with ADHD to develop self-regulatory behaviours such as time management, organisational skills, paying attention in class and taking good notes, with improvements still observed after 8 weeks (Swartz et al. Reference Swartz, Prevatt and Proctor2005). In another study, 19 university students with ADHD on 10 different US campuses were interviewed about the benefits of coaching. These students said that coaching helped to increase their self-discipline, self-efficacy, study skills, formulate realistic goals, think more frequently about their long-term goals and maintain a desire to achieve them (Parker et al. Reference Parker, Hoffman, Sawilowsky and Rolands2013). Additional benefits of coaching were in helping university students with ADHD to feel more in control of their emotions, behaviours and desires in the face of external demands – it strengthened resilience (Parker et al. Reference Parker, Hoffman, Sawilowsky and Rolands2011). Although coaching and CBT, whether delivered online or face-to-face may be effective interventions for university students with ADHD (Young & Bramham, Reference Young and Bramham2012; Curtis et al. Reference Curtis, Chapman, Dempsey and Mire2013), no studies were found that investigated their impact on improving academic grades and/or educational outcomes in general. These interventions could, however, enhance confidence, provide reassurance, and help university students with ADHD to learn new skills or develop different coping strategies for managing academic pressure (Field et al. 2013).
Substance misuse and non-medical use of stimulants
The patterns of substance misuse among university students with ADHD is such that they are about three times more likely to have used cannabis or tobacco, and about five times more likely to have used other illicit substances, in comparison to their non-ADHD peers (Rooney et al. Reference Rooney, Chronis-Tuscano and Yoon2012). University students with ADHD are also said to regularly consume alcohol, feel less able to control their alcohol intake and be more prone to episodes of binge drinking (Baker et al. Reference Baker, Prevatt and Proctor2012). University students with ADHD who use stimulant medication tend to report more drinking-induced blackouts, hospitalisation due to drinking, losing friends and romantic partners as a result of their drinking habits (Baker et al. Reference Baker, Prevatt and Proctor2012). In one study as cannabis and alcohol misuse escalated, university students with ADHD, increasingly skipped classes and reductions in their grades were observed. As this chain of events was experienced, the likelihood of misusing stimulant medications for academic purposes also increased (Arria et al. Reference Arria, Wilcox, Caldeira, Vincent, Garnier-Dykstra and O’Grady2013).
University students with ADHD who use stimulant medications are more likely to be approached by other students to sell, give or barter their medications (McCabe et al. 2006), while students taking other medical prescriptions are more likely to use their medication to barter for stimulants (McCabe et al. Reference McCabe, Teter and Boyd2005; Holloway & Bennett, Reference Holloway and Bennett2012). In one study Rabiner et al. (2009 Reference Rabiner, Anastopoulos, Costello, Hoyle and Swartzwelderb ), investigated the misuse and diversion of stimulant medications among 115 university students. Findings revealed that 89 of these students (69%) had used their medication as prescribed. However, 36 students (31%) had misused their medication by taking larger doses, or more frequent doses, or they used someone else’s medication, while 30 students (26%) had given their medication to peers and nine students (8%) had engaged in intranasal use in the previous 6 months. In a review of studies from North America, between 5% and 35% of university students reported having used ‘study drugs’ in the last year (Wilens et al. Reference Wilens, Adler, Adams, Sgambati, Rotrosen, Sawtelle, Utzinger and Fusillo2008). In Europe prevalence rates for the use of ‘study drugs’ is estimated between 0.8% and 16% (Castaldi et al. Reference Castaldi, Gelatti, Orizio, Hatmung, Moreno-Londono, Nobile and Schulz2012; Maier et al. Reference Maier, Liechti, Herzig and Schaub2013; Ott & Biller-Andorno, Reference Ott and Biller-Andorno2014). University students coin stimulant medication used for academic purposes as study drugs, smart drugs, brain dope or academic steroids. The misuse of stimulant medication is also described by several names – pharmacological cognitive enhancement (PCE), neuro-enhancement, cosmetic pharmacology.
The first national online survey of ‘PCE’ use in the United Kigdom and Ireland was conducted by Singh et al. (Reference Singh, Bard and Jackson2014). In this survey, 877 students with no known diagnosis of ADHD were asked questions about smart drugs, patterns of use, purpose of use and ethical issues pertaining to their use. The listed medications were methylphenidate, adderall, modafinil, donepezil, piracetam and atomoxetine. Most of the students (79%) were enrolled at 23 of the 24 Russell Group Universities. The most represented universities were Bristol, Manchester, Cardiff, LSE, Cambridge, Oxford and UCL. The top seven descriptions of ‘smart drugs’ reported by the students were caffeine pills, methylphenidate, energy drinks, vitamin supplements, modafinil, tranquillizers and speed. About 30–45% of students reported using energy drinks and caffeine pills as PCEs, while only 35 students reported using methylphenidates as PCEs (almost 4%). Modafinil was the most unknown yet also the most used, with 54 students using them as PCEs (almost 6%), whereas about 59% (514 students) said they had never heard of modafinil and about 24% (213 students) said they had no interest in trying the drug. Two-thirds of the students reported no interest in using methylphenidate, adderall or modafinil for any purpose and 14% of students (n=123) had never heard about smart drugs. The most common reasons cited for not using methylphenidate, adderall or modafinil was a lack of availability, followed by concerns about side-effects and illegality. Students who had used study drugs, mainly obtained them from friends, although in the case of modafinil, via the internet. Although 69% of students agreed or strongly agreed that PCE use at university was ethically problematic, for the students who had used or considered using smart drugs, the use of PCEs at university was not reported as problematic. When PCE use was framed in the context of cheating, 72% of students disagreed that it was cheating. Singh et al. concluded that university students in the United Kingdom and Ireland were resilient to PCE use, because low prevalence rates of using smart drugs were reported in their study.
Not much is known about the use of study drugs outside the US student population. Duke University in the United States for instance, has enacted a policy banning the misuse of prescription stimulants for academic purposes, adding it to the definition of cheating (Lakhan & Kirchgessner, Reference Lakhan and Kirchgessner2012). This contrasts with the finding by Singh et al. (Reference Singh, Bard and Jackson2014), that 72% of students disagreed that PCE use was cheating. Defining the use of study drugs as cheating could fuel notions that stimulant medications enhance academic performance, and this could drive the practice underground, just like all other illicit substances. The use of illicit substances does contravene the drugs and alcohol policies of most universities, and it may make sense to include the misuse of prescribed stimulants under this policy. However, such a move, especially in Ireland and the United Kingdom, where recognition of adult ADHD is beginning to grow, might heighten concerns about university students malingering with ADHD and/or augment unhelpful assumptions that ADHD is not a real disorder (Moncrieff et al. Reference Moncrieff, Rapley and Timimi2011).
Malingering
Malingering describes the behaviour of pretending to ill. Some authors believe university students malinger with ADHD. The research on malingering suggests that university students do so to get a diagnosis of ADHD and a prescription for stimulant medication (Harrison et al. Reference Harrison, Edwards and Parker2007). In one systematic review of studies about malingering, Musso & Gouvier (Reference Musso and Gouvier2014), reported on a number of strategies that university students used to feign ADHD during an educational psychology assessment. These strategies included ignoring visual and auditory stimuli, making intentional errors of commission and omission, responding randomly to questions, fidgeting with intention, ‘zoning out’, disobeying instructions, selecting items on a screening tool that matched Diagnostic Statistical Manual (DSM-IV) criteria, pretending to have trouble with memory recall or acting confused. Concerns about malingering among university students have prompted researchers to look for reliable assessment methods for its detection. Out of several ADHD symptom checklists, neurocognitive tests, symptom validation tests, neuropsychological assessments, none had proved to be reliable in detecting malingering (Conners, Reference Conners1995; Booksh et al. Reference Booksh, Pella, Singh and Gouvier2010; Sollman et al. Reference Sollman, Ranseen and Berry2010; Jasinski et al. Reference Jasinski, Harp, Berry, Shandera-Ochsner, Mason and Ranseem2011). A reason given for this finding was that many psychological measures/instruments have subscales to assess the validity of self-reports, but ADHD symptom checklists/assessment tools do not have similar subscales (Quinn, Reference Quinn2003). University students who self-report symptoms of ADHD, especially with the absence of teachers or parents’ information, can feign ADHD, in the same way that anyone can feign a mental or physical health condition. The detection of malingering ultimately depends on the knowledge, skills and expertise of the practitioner undertaking the assessment of ADHD. While concerns about malingering are valid, the belief that university students tend to pretend to have ADHD, can also result in a failure to recognise the disorder (Webb, Reference Webb2001). A missed or under diagnosis of ADHD is even more likely in university students who are 2e, obtain good grades or have developed effective coping strategies for their symptoms (Beljan et al. Reference Beljan, Webb, Amend, Web, Goerss and Olenchak2006).
Discussion
A summary of the key findings is presented in Table 3. These findings contribute to understandings about the impact of ADHD on the educational outcomes of university students. Methodological limitations of most of the studies, such as small sample sizes recruited at a single institution, makes it difficult to generalise findings to university student populations in North American, Ireland and the UK. Many of the studies reviewed also tended to compare the academic functioning of university students with ADHD versus their non-ADHD peers. Not many studies examined educational outcomes of university students with ADHD relative to their peers with ADHD. But once this is done, it becomes apparent that many university students with ADHD adjust well to all the domains associated with university life (Blase et al. Reference Blase, Glibert, Anastopoulos, Costello, Hoyle, Swartzwelder and Rabiner2009). Another issue could be the assumption that EF deficits affect the way that university students with ADHD learn and process information (Biederman et al. Reference Biederman, Fried, Petty, Henin, Wozniak, Corkum, Claudat and Faraone2006). The research about the EF deficits<>ADHD pathway to poor educational outcomes remains inconclusive. EF deficits are not found in all people with ADHD (Thorell, Reference Thorell2007). This could explain why some studies (e.g. Pope, Reference Pope2010) identified more with the EF deficits<>ADHD inattentive sub-type pathway to poor educational outcomes, rather than with the hyperactivity/impulsivity or combined sub-type. ADHD inattentive sub-type is usually associated with poor academic functioning (Weyandt & DuPaul, Reference Weyandt and DuPaul2008). Females are said to have more ADHD inattentive sub-type (Hinshaw et al. Reference Hinshaw, Owens, Zalecki, Huggins, Montenegro-Nevado, Schrodek and Swanson2012), yet females are also more likely than males to do well at school, enter into higher education and graduate from university (Independent Commission on Fees, 2015).
Table 3 Summary of key findings about university students with attention deficit hyperactivity disorder (ADHD)
PCE, Pharmacological cognitive enhancement.
Traditional educational environments are said to be ADHD-user unfriendly (Carter, Reference Carter2005; Davis et al. 2011; Dare & Nowicki, Reference Dare and Nowicki2015; Lee & Olenchak, Reference Lee and Olenchak2015). One argument for the association between ADHD and NMTech overuse, substance misuse, non-medical use of stimulant medications and malingering, could be that they are evolutionary strategies used by university students with ADHD to adapt to systemic barriers within HEIs (Slee, Reference Slee2013; Barberis & Buchowicz, Reference Barberis and Buchowicz2015). In the early 1900s, one of the key principles of ‘scientific education’ was ‘to eliminate the waste of retardation, ill-health and lowered vitality’ (Bobbitt, Reference Bobbitt1912: 266,). Grades on standardised tests seemed to be the means by which this ‘elimination’ occurred (Terman, Reference Terman1906; Snedden, Reference Snedden1921). Even today, this still could be one reason why university students with ADHD generally do not perform well in time-limited examinations.
Conclusion
In Ireland and the United Kingdom, a paucity of research about the impact of ADHD on the educational outcomes of university students was found. This is concerning because ADHD is typically associated with poor educational outcomes. This literature review provides some insights into key areas of concern. While symptoms of ADHD can indeed impair learning at university, no research in Ireland or the United Kingdom, was found about how reasonable adjustments to programmes of study promote positive educational outcomes. No studies were found that examined the views and perceptions of university students with ADHD about how they adjust to university life, or about the academic challenges they face and how these are managed or overcome. This gap in the literature needs to be addressed. University students seem to continuously face a lack of timely access to treatment services for ADHD. In some areas in the UK for instance, waiting times for access to treatment in the National Health Service (NHS) can be up to 2 years. University students who suspect they may have ADHD cannot afford to wait this long to access treatment, without risking academic failure or increased psychopathology. For these students’ the misuse of caffeine products or stimulants (licit or illicit) may seem like attractive options.
The provision of rapid access to treatment for students with ADHD may be a challenge for clinicians working in national health services. Such challenges have motivated the author to undertake a research project to develop a model of practice, that sits at the interface between education and psychiatry. This inter-disciplinary designed model will provide HEIs with a strong business case for funding ADHD diagnostic assessments for their students. For too long young people with ADHD have been marginalised. Under current systems, these students continue to be at considerable risk of not having their learning problems, treatment and support needs identified. Interestingly in 2005, Maryla Carter submitted similar concerns in a memorandum to the Select Committee on Education and Skills in the UK Parliament about children with ADHD. In an excerpt from this memorandum she stated: ‘… this situation is leading to children with ADHD being “abused” by the system—a system which has not been designed to include such neuro-atypical human beings … yet with a prevalence of around 3% one could argue that having ADHD is not particularly atypical – but merely different … As things stand at present, the real needs of children with ADHD are being sacrificed upon the altar of inclusion … All too often the outcome is the complete opposite of this—exclusion … frequently followed by problems to do with mental health, drug addiction and the criminal justice system … Our society is paying an enormous price for this imposition of inappropriate education …’ (Carter, Reference Carter2005).
The philosophies of difference, equity and self-realisation can provide a conceptual framework for researchers wanting to undertake further work in this topic area. The difference of ADHD needs to be recognised and catered for within learning environments (Mackenzie & Watts, 2011). Once this is achieved, different educational outcomes for university students with ADHD may ensue. Equity is about enabling university students with ADHD to increase the good things in their lives and decrease the bad things (Bentham, Reference Bentham1948). Equity is central to the principle of difference and self-realisation, which is about the right of university students with ADHD to achieve their full academic potential, even if it means providing them with extra support (Dewey, Reference Dewey1893). The social model of disability supports this view and adds the importance of removing systemic barriers that deter self-realisation (Oliver, Reference Oliver2013). After all, university students with ADHD are at a crucial stage of transitioning into adult life. Their success at university is likely to determine their career success and progression within highly competitive employment markets.
Acknowledgements
The author would like to thank her supervisor Professor Philip Asherson; Dr Ulrich Müller and colleagues at the UK Adult ADHD Network (www.UKAAN.org), for their expert guidance and support with her ongoing research and service development project for university students with ADHD.
Conflicts of Interest
None.
Ethical Standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committee on human experimentation with the Helsinki Declaration of 1975, as revised in 2008. The authors assert that ethical approval for publication of this review article was not required by their local REC.
Financial Support
A bursary towards PhD tuition fees is being received from the Royal College of Nursing Foundation.





