

The quest to reduce civilian harm
War is the realm of uncertainty; three quarters of the factors on which action in war is based are wrapped in a fog of greater or lesser uncertainty.
— Carl von ClausewitzFootnote 1The number of dead and injured has been a measure of war for as long as bodies have littered battlefields. As the news and the injured reached home, however, societies realized that the effects of battles reverberate far beyond the combat zone and long after the dust has settled. As Plato is said to have declared: “only the dead have seen the end of war”.
In seeking a better measure of the human cost of war, military and other institutions now seek to gauge “civilian harm”.Footnote 2 Along with research, human rights, and humanitarian organizations, they investigate the relative impact of conventional versus asymmetric and urban warfare,Footnote 3 and of short, intense military campaigns versus long, drawn-out ones.Footnote 4 Much of the discussion of this collective effort centres around data: what quantitative data is required, how to collect it, how to complement it with qualitative data, and what indicators serve best as proxies for what is not readily measurable.
As the first article in this series discussed, the evidence base required to detail the impact of an explosion upon water or wastewater services can be generated with considerable technical data and institutional or engineering expertise.Footnote 5 Considerably more information and skills are required to determine the effect that the damaged water service has on indirect impacts, however – such as a reduction in livelihoods or as a driver of their displacement. This is because of the great number of variables involved; the local economy may have already been in a poor state, for example, and the decision to flee could be more related to security and/or greater opportunities for child education, than concerns about drinking contaminated water.Footnote 6 In most cases, and certainly in the protracted urban armed conflicts that this article focuses on, the desired evidence base is not at hand. The process leading to the decision to carry out attacks in these contexts is necessarily based on the best available intelligence, and not on perfect intelligence. This uncertainty is part of the “fog of war” which famously engulfs the options which are perceived to be available to combatants.
This article tackles the challenge of improving the database: first, by detailing how the damage caused by an attack impacts upon the quality of public service delivery; and second, by investigating how and the extent to which that impact translates into further civilian harm. More specifically, it queries the quality of information and evidence base for the impact that attacks in protracted armed conflict have on the quality of water and wastewater services, and the extent to which the effects of the attack on the degraded service reverberate onto the outbreak and transmission of infectious disease. The data reviewed comes from policy and research papers (primarily technical engineering reports), observations and a review of the impact of explosive weapons in Basrah, Yemen and Gaza. These are interpreted within uncertainty theory and discussed in relation to international humanitarian law (IHL), standard military operational planning processes, and intelligence-gathering and decision-making procedures in the midst of armed conflict, including prior to attacks.
The review establishes that there is a strong evidence base of the consequences of attacks using explosive weapons on the functioning of water/wastewater services, and a high level of confidence in information about the consequences of degraded services on infectious disease. Attaining a similar level of confidence in the knowledge of reverberating effects of an attack along this consequential chain (i.e. how sure are we that attack x has caused disease y?) would require a damage assessment of the physical integrity of the infrastructural asset and the impact it has on the delivery of the service, disease monitoring and geo-referenced epidemiological data on non-communicable diseases on the affected population, and a robust method to control for the influence of the great number of compounding factors involved.
Acknowledging that the evidence base is not likely to be of the quality desired when targeting decisions are made, the analysis identifies a number of patterns that may guide and inform the military operational planning and targeting processes. For water/wastewater services in particular, for example, the clearest risk of an outbreak or spread of cholera arises when people consume water which has been contaminated with wastewater (which is referred to as “cross-contamination”). The article also discerns several patterns related to the duration of the conflict within which the attack occurs. For example, as the conflict become protracted, the resilience of the service is expected to degrade, because battle damage accumulates and routine operations and maintenance are no longer carried out; the risk of an outbreak or spread of infectious disease is expected to increase, as exposure to hazards (such as cross-contamination) becomes more likely; and the evidence base for gauging the reverberating effects is expected to improve, as the effects become more visible, familiarity with the systems is gained, and more effort into intelligence gathering can be invested.
The article concludes that, in general, the reverberating or indirect effects caused by attacks on water/wastewater infrastructure can be foreseeable in some contexts and become more foreseeable as the conflict prolongs. The most pragmatic path for military institutions and those involved in targeting operations to take this into account is through a “precautionary approach”,Footnote 7 which assumes the existence of the reverberating effects, and which seeks to identify and understand them through intelligence preparation of the operating environment (IPOE), and standard military operational planning processes.
Reverberating effects
Some definitions of the terms are in order, given the complexity of the challenge that has been laid out. Based on their decades of experience, humanitarian water engineers assert that the impact of armed conflict on a service can be measured in terms of direct, indirect or cumulative impact, and can occur on the people, hardware and consumables which keep the service running.Footnote 8 The services in question could be health care, education, solid waste removal, financial flows, or the so-called “lifeline services” of electricity, water and wastewater. Most services are dependent on other services for their proper functioning, and some are very highly interdependent (e.g. effective treatment of patients at a hospital typically requires electricity and clean water).Footnote 9 The impact of an attack during armed conflict can result in damage to a service, which can be measured in terms of the direct effects and the reverberating effects.Footnote 10 Such attacks can take various forms, such as targeting of service provider personnel or supply-lines of consumables, cyber-attacks on infrastructure systems, and the use of explosive weapons on or affecting the service systems (the latter of which is most commonly considered in this article).
In a general sense, the impact of an attack or an explosion is understood in terms of the marked “impression” or “footprint” of an attack, while the effect of an attack refers to the consequences that follow it. Table 1 exemplifies the terms in order to distinguish the differences. Traditionally concerned with the functioning of a particular service, the humanitarian engineering view of the reverberating effects of an explosion or attack are seen to extend to the functioning of other services that the service is dependent on, or which depend on it.Footnote 11
Table 1. Measures of the impact and reverberating effects of an attack classed according to expected distance and duration, with examples from a water treatment plant

IHL (also known as the laws of armed conflict) obliges those planning or deciding upon attacks to take into account all reasonably foreseeable incidental harm when considering questions of proportionalityFootnote 12 and precautions in attack.Footnote 13 Such “harm” includes both direct effects of an attack (e.g. deaths, injuries, or damage to civilian objects) as well as reverberating effects (also known as the indirect consequences).Footnote 14 IHL jurists also note that the extent to which the resulting incidental harm can be foreseen depends on, inter alia, the circumstances of the attack and the target, and that “patterns of incidental harm can be foreseen based on the past effects of urban warfare”.Footnote 15 Similarly, the disarmament research community refers to the range as first-level, second-level and third-level impactsFootnote 16 – which by definition extend to all interdependent services.
The example of a damaged drinking water service in Table 1 helps to distinguish use of the terms, and further notes how the effects of an attack reverberate in time and across space. The immediate impact of an explosive weapon that detonates near a water treatment plant could result in physical damage to the pumps which push the treated water to consumers. The consequences of the damage to the water service could extend to the health service, if less water is pumped throughout the water network and a nearby hospital is without water in its taps. Some of the consequences of the lack of clean tap water in a hospital include the lack of adequate sterilization of surgical instruments, and (so) a greater number of infections of patients’ wounds. Data collection efforts aimed at better gauging civilian harm would class all such consequences as “reverberating effects” (while the number of people infected could also be classed as a “third-level” impact).
The previous article in this series explains how the spatial extent of the reverberating effects of an attack depends primarily on the hierarchy of the component suffering the direct impact (i.e. “upstream” components, e.g. water treatment plants; “mid-stream” components, e.g. water transmission lines supplying water to neighbourhoods; or “downstream” components, e.g. household water piping or rooftop storage tanks).Footnote 17 The duration of the reverberating effects depends on the “baseline resilience” of the service before the explosion, which is itself a function of system redundancies and emergency preparedness and response. The baseline resilience of a service is also referred to as the “underlying conditions” or “pre-crisis vulnerability” of a service.Footnote 18 In brief, and as Figure 1 shows, the less resilient the service is when the attack occurs, the greater the impact and the reverberating effects are expected to be. As a jab to a boxer in the twelfth round is likely to cause more damage than a jab in the first, an attack on a service that has experienced years of neglect and which is not likely to be rebuilt immediately is expected to cause more disruption than it would on a well-maintained service with full emergency-preparedness measures in place.

Figure 1. Expected relation between the civilian harm caused by incidental damage to a service, and the baseline resilience of that service, as armed conflict prolongs. The longer the armed conflict and less resilient a service is, the greater the civilian harm is expected to be.
Uncertainty and (pre)caution
Though the examples discussed are straightforward, most reverberating effects are not. Like the tornado caused by the flap of the proverbial and distant butterfly's wings, the reach of the consequences of an attack are almost without limit. As discussed earlier, an assertion that an explosion near a water treatment plant results in mass displacement cannot be made with any confidence, because there are dozens of other reasons which can explain reductions in economic activity or displacement.
The reasoning follows the classic adage of unforeseen consequences: “for the want of a nail, the kingdom was lost”. As the number of factors that shape an outcome increase, so does our ability to prove causality decrease. In other words, the longer that the chain of consequences under question is, the less confidence we can have in the information we have about it. Climate scientists refer to this compounding of factors as a “cascade of uncertainty”.Footnote 19
The relevant question generated by uncertainty theory is: if an observed association between factors cannot be proven with confidence, does that mean it does not exist? The related policy question is: If an association is observed but has not been “proven”, should policy be designed to incorporate its possibility, or to ignore it? The range of answers from different institutions will vary from reckless to cautionary, depending mostly on the costs of getting it wrong, and how familiar they are in dealing with the absence of the desired level of knowledge.
It is in this sense that the quest for ever more data about civilian harm is an attempt to reduce uncertainty. With precisely this in mind, simulation models feed on data to quantify risks and probabilities. The logic is compelling: a model could predict the strain that will be placed on Hospital X (measured in terms of the staff and beds) when 5000 civilians who contracted cholera following the bombing of Wastewater Treatment Plant Y compete for health service resources which are already allocated to caring for the 400 combatants who were wounded directly from the fighting. Targeting processes could then assign the wastewater treatment plant a corresponding level of importance. The number of civilian lives that would be spared could be estimated, and the reduction in civilian harm extrapolated accordingly.
Models have their downsides, however, as studies of wargaming and other models have shown.Footnote 20 The most well known of these is that the quality of the output of the model directly reflects the quality of the data entered into it – regardless of how sophisticated the algorithms and modelling process. “Garbage in, garbage out” is the undeniable if inelegant heart of modelling processes.
Even in the most wealthy, stable and well-ordered societies, public service providers do not have all the information they would like,Footnote 21 and so cannot rely fully on modelling. Even as they continue to monitor and collect more information, most institutions develop an approach to policy that is “comfortable” with uncertainty. For example, health, civil engineering and disaster risk-reduction guidelines usually choose to “err on the side of caution” by assuming that any negative impact of their projects will reverberate widely, and then establish measures to prevent or contain them.Footnote 22 This manner of developing policy in uncertain operating environments is widely known as the “precautionary approach”.
Military decision making and intelligence gathering follows much the same approach. Because armed conflict in cities is the normal operating theatre of seasoned military institutions, the processes developed to prepare for and to be more effective in battle are designed to make best use of the information that is available. For instance, risks can be calculated and then fed into the targeting procedure, which can then inform the proportionality assessments and weaponeering decisions.Footnote 23 The US military, for example, reduces the uncertainty of a complex operating environment by identifying, assessing and controlling risks arising from or during military operations throughout the targeting cycle (e.g. find, fix, track, target and engage)Footnote 24 and as part of the IPOE.Footnote 25 In the sense that the term is used here, such procedures are “precautionary”.
The measures taken by military institutions through these procedures puts them in a stronger position to achieve military objectives with less civilian harm, as well as compliance with the principles of IHL. As previously noted, however, such compliance rests on gauging the extent to which reverberating effects are “reasonably foreseeable” in the sense that they “may be expected” (Art. 51(5)(b) of Additional Protocol I).Footnote 26 The task for those who seek to better gauge (and, so, minimize) civilian harm is thus to map out the extent to which the reverberating effects of an attack may be expected.
Cause and effect between attacks, water, wastewater and disease
The extent to which the reverberating effects caused by attack play out on water/wastewater services can be gauged first by determining the level of confidence in information about the impact on the services, and the subsequent influence on the outbreak and transmission of infectious diseases.
Links between water and wastewater, and disease
The evidence base supporting the importance of clean drinking water for reducing the risk of outbreak or rate of transmission of infectious disease is by now so well established that it is no longer questioned very much. One of the greatest concerns is when wastewater contaminates drinking water. The spread of the Spanish flu through the mud, faeces and wastewater which lined the trenches of the First World War is considered to have killed more people than both world wars combined, for example. Similarly, the lack of clean water and adequate wastewater evacuation in the refugee camps of the Democratic Republic of Congo is blamed for the epidemics of dysentery and cholera which claimed over 40,000 people from Rwanda in 1994. In fact, the outbreak and transmission of cholera was linked to bugs in the water more than a century earlier, through pioneering efforts to contain the spread in London.Footnote 27 While the orthodox scientific knowledge of the day held that cholera was spread through the air, those who persisted in sampling drinking water prevailed, and the study of the ways that pathogens and environmental contaminants travel (epidemiology) was born. Chlorine was quickly found to be the best way to kill these pathogens; its addition to Tokyo's drinking water service led to a drop in the infant mortality rate of 18,000 per year in 1915 to less than 1000 by 1998, for example.Footnote 28
Like other diarrhoeal diseases, cholera and dysentery originate from a number of sources, are usually contracted by contaminated water or food, and are readily spread in water and wastewater,Footnote 29 and are just as deadly. The World Health Organization (WHO) estimates that they caused over 1.5 million deaths of children under the age of 5 years in low- or middle-income countries in 2002.Footnote 30 Indeed, children under the age of 5 years are “more than 20 times more likely to die from diarrhoeal disease linked to unsafe water and sanitation than violence in conflict”.Footnote 31
The transmission routes of these and related diseases are very well known. As in Figure 2, the cross-contamination of wastewater and drinking water is in fact just one of several potential routes of disease transmission (diarrhoeal or otherwise). Just some of the variables that compound the complexity – and, so, reduce certainty about the main drivers – include the presence of a new strain of disease in inward-migrating people, pathogens transmitted by flies or animals, and direct physical contact with contaminated surfaces.

Figure 2. Some infectious disease transmission routes. Pathogens which develop in humans and wastewater hazards can be carried through water bodies (and other carriers) until exposed to humans, causing disease.Footnote 34
Policy and operational responses designed to tackle the water-related transmission and exposure routes focus on interrupting them, through, for example, chlorination and handwashing, or prevention. The cardinal rules that humanitarian water engineers follow to avoid an outbreak of infectious disease is to chlorinate, so that the pathogens are eliminated, and to ensure that drinking water pipes and raw wastewater systems are kept physically separate (i.e. to prevent cross-contamination). Such interventions are effective. A systematic review of over 2000 interventions to prevent diarrhoea found that all of themFootnote 32 reduced the risk.Footnote 33 However, cholera and the more common forms of diarrhoea persist. In rural areas, the risk of cross-contamination arises from buckets dipped into an unprotected (and unchlorinated) village water well. In urban areas, the concern is when the wastewater is not treated adequately (because the treatment plant has been run down), a malfunctioning pumping station means the wastewater is not evacuated from a built up area, or when leaks from wastewater drainpipes seep into drinking water sources – particularly if the chlorination of the latter is below par.
The impact of attacks affecting water and wastewater services
Of course, different types of attacks affect water and wastewater services in different ways. A cyber-attack that aims to disrupt the services’ operating system may inflict damage that is much less visible than an air-to-surface missile attack on an isolated component of the infrastructure, for example. Explosive weapons employ low- and high-explosive substances to create blast, and commonly fragmentation, in order to achieve a particular effect. The damaged caused by the use of explosive weapons in protracted urban armed conflicts, where population density and foot traffic are high, is not only a result of the blast itself, but also of the fragmentation and heat which are produced by the detonation. These three mechanisms can also cause extensive harm to civilians and infrastructure through penetration, ground shock, cratering, secondary fragmentation and fire.
Researchers and humanitarian water engineers have documented such damage from armed conflicts that have taken place all over the world, the latter usually as an internal reporting requirement for the institution which employed them or as a means to request a pause in hostilities in order to ensure safe access for the operation, maintenance or repair of infrastructure.Footnote 35 The dozens of reports detailed in Table A in the Annex cover a very wide range of impact and follow no common methodology. Read collectively, however, they do reveal a number of patterns which offer a snapshot of the “working knowledge” which backs the authority they have developed on the topic over the decades of their careers.Footnote 36 Each of the reports documents the extent of direct damage to water infrastructure, at a minimum – possibly because this form of damage is the most visible and easiest to repair. The quality of the service prior to the attack may be inferred from this direct impact, particularly when the documentation spans a number of attacks, or when the same case is revisited years later by the same author (or a new author with access to the prior reports). The measures of this “baseline resilience” are defined generally by the level of inherent infrastructure redundancies in the systems, by the existence of an emergency preparedness plan (EPP), and the capacity of the service personnel to execute the EPP (or simply to maintain or restore the service in face of long-term degradation or short-term interruption).Footnote 37 The evidence base of Table A further reveals patterns of deterioration of wastewater treatment plants (which are usually prone to partial or total failure because of the lack of sophisticated replacement parts on the open market, as in Kabul, Monrovia, Brazzaville and Grozny) and malfunctioning chlorination systems (which often fail to lack of sophisticated replacement parts or chlorine gas, tablets, or liquid on the open market, as in Dilli, Huambo, Novi Sad and Baghdad). The concern for cross-contamination of wastewater and drinking water can be inferred in each of the engineers’ reports, and is prevalent in several. The concern is most notable where sewage ponds develop in public areas (and surrounding drinking water pipes) after drainage lines back up when booster pumps fail (Kabul, Beirut, Basrah, Mogadishu, Novi Sad). A further pattern that can be gleaned from the reports which is of direct relevance to the topic at hand is that the concern shown for degraded water and wastewater systems stems not from evidence but from assumptions that the public health risks increase accordingly. Data is collected from within the “silos” of professional expertise; humanitarian engineers and health workers rarely mix, and even less frequently with munitions experts and epidemiologists.
The chain of consequences that reverberate from damage to water and wastewater services and infectious disease
To summarize findings to this point: over a century of epidemiological study of transmission routes has developed a robust scientific body of knowledge that infectious diseases can spread through water and wastewater, and a more recent body of knowledge has documented how attacks can damage water and wastewater services in ways which facilitate cross-contamination between the two.
It is when seeking causation along the attack–water/wastewater service–infectious disease chain of reverberating consequences that the uncertainty begins to cascade. Indeed, a systematic review of nearly 4000 research articles (published between 1980 and 2014) on the effectiveness of water and sanitation interventions to improve health outcomes in “humanitarian crises” found the evidence base to be “extremely limited”.Footnote 38 Only six papers found interventions to produce change that was significant enough to be counted.Footnote 39
The bulk of investigations into the consequences of the attack–water/wastewater service–infectious disease chain remains associative, and very tricky to untie from the effects of the armed conflict within which they occur. Studies have shown, for example, how outbreaks of hepatitis A during the 1990s war in Bosnia are attributed – in part – to the virtual collapse of “the hygienic [read water and wastewater] infrastructure which was intended to protect against enteric disease”.Footnote 40 The outbreak was followed by “staggering” (and relatively well-documented) rates of diarrhoea and dysentery. In a similar vein, the impact of the US/UK invasion of Iraq on public health was considered to work its way “through specific diseases and conditions” such as AIDS and cancer.Footnote 41 Epidemiologists blame water-related pathogens (like Vibrio cholerae, which results in cholera) for 85% of the 50,000 deaths after the sudden influx of nearly one million refugees from Rwanda into the Democratic Republic of Congo in 1994,Footnote 42 though do not link it with attacks on water and wastewater services. And while there is clear association between periods of high-intensity armed conflict, damage to water and wastewater systems, and spikes in diarrhoea in Aleppo and Idlib (Syria), “multiple confounders” mean that no direct co-relation can be drawn.Footnote 43 Interpreting such associations as consequential chains with any certainty requires the deeper understanding provided by case studies.
Reverberating effects of attacks in protracted armed conflict
This section reviews public-domain literature on Iraq, Yemen and Gaza to gauge the extent of confidence in information about the attack–water/wastewater service–infectious disease chain. Because of the importance that the “baseline resilience” of any service (Figure 1) plays in determining the extent of civilian harm, attacks are considered within the protracted armed conflict in which they occur.
Water/wastewater and cholera in Basrah, Iraq
As shown in Figure 3, the decades-long decline of Basrah's drinking water system from world-class to “worst-class” has been attributed mostly to the accumulation of indirect impact of armed conflict,Footnote 44 rather than to by parties to armed conflict per se. As attacks precipitated each degradation, their reverberating effects should be considered, particularly for links with the thousands of cases of cholera and other water-related disease in 2015 (if not the “water riots” three years later).Footnote 45

Figure 3. The long and predictable decline of the quality of the drinking water service in Basrah. Draft based on Zeitoun et al. 2017.Footnote 49
Even when it was of top quality, Basrah's drinking water system was vulnerable to disruption due to its heavy reliance on a single source and means of delivery – the al-Bada'a water canal which brought freshwater hundreds of kilometres from the Euphrates River to a large reservoir that then supplied raw water to a series of treatment plants where the water was cleaned and pumped into the network in Basrah. This source was developed after the raw water quality in the original source (the nearby Shatt al-Arab river) had started to deteriorate (mainly due to salinization, as far back as the 1980s).Footnote 46 The canal and related distribution pipes were damaged by attacks in 2003,Footnote 47 thereby setting off a heavy reliance on locally desalinated and unregulated water supply services.Footnote 48 Over 4500 cases of cholera were reported in Iraq in 2007, primarily in Baghdad.Footnote 50 The baseline resilience of the wastewater service was compromised to a greater extent as the wastewater treatment plant was never completed (because construction was halted as the foreign contractors fled the instability that followed hostilities in 1991).Footnote 51 The sewers and wastewater pumping stations that had been completed on the very flat city filled up, and, as a result, standing wastewater puddles have been present in populated areas for decades.Footnote 52
As the quality of the water and wastewater services declined, the risk of both contamination of the water and public exposure of untreated wastewater in populated areas increased. By 2015, the water authorities were obliged to return to the extremely salty Shatt al-Arab river as an alternative source. Water engineers who faced the challenges were certain of cross-contamination of the wastewater and drinking water,Footnote 53 and many were warning of the possibility of an outbreak of communicable disease. Over 2000 cases of cholera were reported soon afterwards.Footnote 54 By 2018 over 110,000 cases of diarrhoea, vomiting and other ailments were reported.Footnote 55 These have been attributed to a combination of ageing filtration media for water treatment, failing pumps (indirect impact) and the temporary discharge of wastewater to the Shatt al-Arab river (which had by that time become a source of drinking water).Footnote 56
Wastewater and cholera throughout Yemen
Subject to armed conflict since 2015, the worst outbreaks of cholera globally this century have occurred in Yemen.Footnote 57 Over two million cases and 3500 deaths were reported during the identifiable waves of 2016 and 2017.Footnote 58 While some have attributed this to changes in rainfall,Footnote 59 most concur that the outbreaks are due to failures in the water and wastewater services, which are a result of the destruction of and damage to critical infrastructure that enables these services.Footnote 60
In response to the outbreak, humanitarian actors have stressed the importance of improving the “underlying conditions” (read “baseline resilience”) of the health and safe drinking water, sanitation and hygiene (WASH) sectors.Footnote 61 The country does not have much water to draw on in the first place,Footnote 62 with coastal cities suffering from saltwater intrusionFootnote 63 and cities in the highlands, such as Ta'iz, famously running out of drinking water in 1996.Footnote 64 Only about 50 to 60% of people in the country had access to safe piped water services before the hostilities.Footnote 65 Indeed, well before the start of the current hostilities, one of the main actors in the development of Yemen's water sector was advocating the importance of alleviating the effects of the earlier crisis in 2011. Gesellschaft für Internationale Zusammenarbeit GmbH (GIZ) notes that the hostilities in Ta'iz city led to a sharp decrease in water supply (from 80% in 2014 to 38% by 2017) and wastewater services (from 70% in 2014 to 38% in 2017).Footnote 66 This kind of deterioration does not bode well in a country where cholera is endemic. The same report also notes that water consumption in twelve out of seventeen governorates in Yemen had fallen below 50 litres per person per day by 2016, which is the level of access required to maintain health concerns at “low” levels,Footnote 67 coupled with a rapidly collapsing health system. Compounding the pressure, roughly 270,000 Yemenis had fled to Ta'iz governorate by 2017, some of whom may have carried different strains of the disease.Footnote 68 It is therefore not surprising that Ta'iz was among the governorates that reported the highest suspected cholera cases (over 31,000 as of 3 August 2017 for the period between 27 April 2017 to 3 August 2017).Footnote 69
The very many routes through which the resilience of the drinking water systems in Yemen was compromised are shown in Figure 4. This emphasizes how specific elements of the water and energy infrastructure and other aspects of the service were vulnerable on one level to armed conflict, and at a second and even more profound level to the adaptations undertaken by individuals and service providers in order to continue to benefit from water or electricity.

Figure 4. Framework of vulnerability and resilience of water systems in Yemen.Footnote 75
Figure 4 suggests that private water vendors may be filling an essential need, but also unwittingly spreading cholera – because of the distribution of untreated (and possibly cholera-contaminated) water.Footnote 70 The baseline sanitation conditions also do not help. Fewer than half of Yemenis had access to the soap so crucial to interrupt disease transmission routes.Footnote 71 Only the major cities are served by wastewater treatment plants,Footnote 72 and less than half of the homes have “adequate” sanitation.Footnote 73 The resilience of both water and wastewater services are known to be linked to the electrical power supply.Footnote 74 When fuel shortages spiked during the economic blockade, operation of water and wastewater, health and many other services was undermined.Footnote 76 To make matters worse, there was a lack of cholera vaccine stockpiles.Footnote 77
By 2019 over 145 airstrikes on WASH facilities had been recorded.Footnote 78 By 2020, ten of the country's thirty-three water treatment plants and five of the country's twelve wastewater treatment plants had been damaged or destroyed.Footnote 79 Access to safe water at the household level dropped in every governorate.Footnote 80 The general paucity of electricity and fuel for generators is judged to have seriously undermined the quality of the water and sanitation services.Footnote 81 As such, the potential for untreated wastewater to cross with drinking water was high,Footnote 82 and the spread of cholera was entirely predictable.Footnote 83 As a United Nations Children's Fund (UNICEF) employee stated, “we are just one airstrike away from an unstoppable epidemic”.Footnote 84
Though humanitarian agencies mobilized, the cholera outbreak still came, in no small part because – as in Basrah – of the mixing of untreated wastewater and drinking water. “(T)he accumulation of stagnant water in the streets due to frequent sewer backups are precipitating the spread of diseases such as cholera, vector-borne diseases, and parasites.”Footnote 85 Indeed, the greatest number of cases appear to have come from the areas where wastewater treatment plants were not functional,Footnote 86 and were also associated with increased incidence of diarrhoea.Footnote 87
Wastewater and diarrhoea in Gaza (before May 2021)Footnote 88
Subject to numerous episodes of armed conflict since 1948, and to full territorial closure and naval blockade since at least 2006, Gaza is notoriously bad both in terms of public healthFootnote 89 and of quality of drinking water.Footnote 90 There furthermore appears to be a strong association between the incidence of diarrhoea and the attacks carried out during the “summer war” of 2014 (see Figure 5).
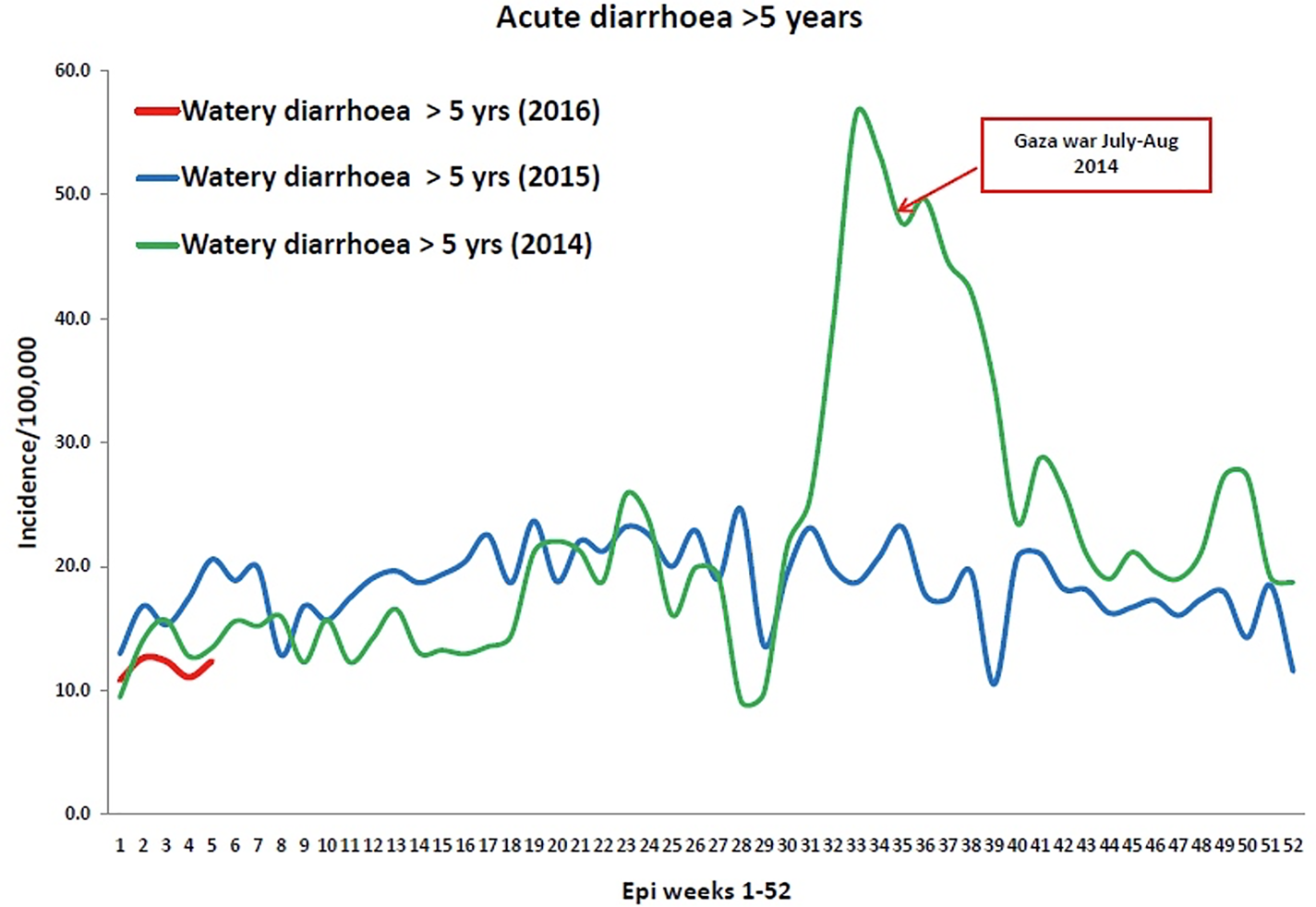
Figure 5. Comparison of reported cases of acute diarrhoea, for 2014 (including the July “summer war”) and 2016.Footnote 91
The “underlying conditions” of water and wastewater services in Gaza are as well studied as they are concerning.Footnote 92 Over 90% of the drinking water supplied by the municipality exceeds WHO drinking water guidelines for nitrates (and 79% for chlorides).Footnote 93 Roughly 40% of water sampled at taps from two hospitals was found to be biologically contaminated in 2020.Footnote 94 This is not surprising, considering how rife the conditions for cross-contamination with wastewater are.Footnote 95 Less than half of the wastewater is routinely treated,Footnote 96 and most regularly seeps into the seaFootnote 97 or into Gaza's main source of drinking water: the aquifer located between one and fifty metres below the sand surface.
The direct impact from the hostilities in 2008–2009, 2012, and even more extensive damage caused in 2014 seems likely to have contributed to the conditions required to communicate disease. One of the anaerobic ponds of the Gaza City wastewater treatment plant was hit in 2009, for example, thereby creating a small flood (over 55,000 square metres) of partially treated wastewater in the surrounding fields.Footnote 98 Alongside damages to a considerable amount of water and wastewater infrastructure, the nearly completed North Gaza wastewater treatment plant was damaged in 2014.Footnote 99
Any evaluation of the likely risk of cross-contamination should also consider the (likely greater) risk of exposure from the great extent of degradation of the water and wastewater services. Routine operations and maintenance become neglected,Footnote 100 as the water authorities struggle to get people to pay their bills,Footnote 101 fuel shortages are chronic, spare parts are very difficult to import past the blockadeFootnote 102 and administrative buildings themselves are attacked.Footnote 103 Like the water services, the quality of the health services is furthermore clearly tied to the (poor) levels of electricity available.Footnote 104 As state-supplied power cuts are scheduled, hospital and wastewater treatment plants use diesel-driven electrical generators for power in between.Footnote 105 When there is not enough diesel to operate the generators, several of the municipal or hospital wastewater treatment plants discharge over the surrounding soil – and into the aquifer or the sea.
The conditions for cholera are so rife and predictable that journalists and think-tanks have drawn attention to the risks faced by Israel.Footnote 106 The decline in the baseline resilience of water and wastewater services in Gaza creates a system-wide vulnerability such that if any single point of failure is rendered inoperable, the entire service risks collapse, while coping mechanisms to safeguard public health are largely inadequate in face of the lack of safe alternatives.
Consequences and implications
Considered together in Table 2, the review of policy and research papers, observations, and the impact of explosive weapons in the protracted urban armed conflicts in Iraq, Yemen and Gaza reveals several conclusions that may be drawn about how effects reverberate from an attack on water/wastewater infrastructure through to the outbreak and transmission of infectious diseases. As previously noted, any conclusions drawn should be done from within the context of the protracted armed conflict in which they occur.
Table 2. Parsing of the cases in the “Reverberating effects of attacks in protracted armed conflict” section, in relation to establishing the level of confidence of the knowledge about reverberating effects along the attack–water/wastewater service–infectious disease chain

Amongst a considerable amount of other findings, a comparison of the cases reveals a clear association between the risk of cross-contamination between drinking water and wastewater, and the observed outbreak or transmission of infectious disease. There was significant information in each of the cases about the degradation of the baseline resilience of the water and wastewater services, and, in the case of Basrah, this is detailed to a considerable extent.
The pattern is reflected in the blue lines of Figure 6, which plots a typical pattern of degradation of water and wastewater services against much more general trends of increasing risk of cross-contamination, risk of outbreak or transmission of disease, and quality of the evidence base about the reverberating effects. The trend of increased risk of cross-contamination (shown in blue) is not detailed because of the very many potential determinants which are not related to an attack (e.g. the lines were not separated by design, the materials used were faulty, etc.). The increased risk of transmission of infectious disease (shown in red) is directly related to the risk of cross-contamination. Further detailing of this trend would require controlling for the previously discussed non-attack-related variables (such as endemic pathogens, new strains introduced to a population, environmental factors, etc.).

Figure 6. Compounded figure based on the review of Yemen, Gaza and Basrah showing the trends between the baseline resilience of water and wastewater services, the risk of cross-contamination, and the associated consequences in terms of infectious disease. The combination of rehabilitation of infrastructure (which restores service delivery) and emergency preparedness planning (e.g. identification of alternative sources to be used as a backup if the primary source fails) together help to strengthen the resilience of the services. The confidence in knowledge about the degradation of the baseline resilience is high, relative to the confidence in the knowledge of the likelihood of cross-contamination and its cause of infectious disease, for the reasons explained in the text. The figure also shows that the quality of the evidence base and the foreseeability of reverberating effects can increase over time, subject to intelligence-gathering efforts.
As such, establishing a cause-and-effect relationship along the attack–water/wastewater service–infectious disease consequential chain with a high degree of certainty would oblige tests that controlled for the influence of these other variables on the outcome observed (as this would allow judgement of the extent to which the variable in question is significant).
Indeed, this article's analysis suggests that more research can be done to factor in the specific characteristics and vulnerabilities of civilian infrastructure and services in order to mitigate civilian harm during conduct of hostilities.Footnote 107 As just one example, the analyses required to feed into targeting procedures should seek to identify the visible infrastructural laydown of water and wastewater services. These could be mapped as part of an IPOE or prior to an attack using geospatial and systems mapping techniques, and specify a range of points of particular hazard (including single points of failure as well as upstream and mid-stream infrastructure) which if rendered inoperable would affect the largest part of the population in the service area. Taken as part of the IPOE, the information of critical civilian infrastructure in the area of operations would be improved through enhanced stand-off recognition (remote sensing techniques, satellite imagery) or directly from allied/local forces or from local authorities.
The effort could be complemented by improved systems-level understanding obtained by involving the relevant engineering expertise and using other open-source information which could help to identify the population served by specific ground-level objects (i.e. water treatment plants) and sub-surface objects (transmission lines under main roads, or bridges). Carried out prior to an attack, the effort can inform weapons selection (usage and restrictions), identification of restricted targets, and the development of a no-strike list. A similar effort would be expected if planning multiple attacks during a protracted armed conflict, since infrastructure condition and use changes with time. Routine ISR (intelligence, surveillance, and reconnaissance) data collection procedures would have to be prioritized and augmented when in the midst of hostilities, to accommodate for the suspected reverberating effects.
Because of the greater level of knowledge that it is possible to acquire, as well as the general awareness that existing services are very likely to be degrading due to reduced operations and maintenance, the quality of the evidence base can increase as the conflict prolongs. This is shown by the green line of Figure 6. What the local health services and humanitarian actors know about the cholera outbreaks in Yemen in 2021 is much better than what was known when they occurred in 2018, for example.
With the importance of understanding the underlying conditions/baseline resilience of any service in mind, the patterns revealed show that reverberating effects of an attack can be expected, to an extent (dashed line of Figure 6). It would not be unreasonable to expect an outbreak of infectious disease if a wastewater treatment plant were damaged, and if its proximity to drinking water sources or infrastructure meant there was a high risk of cross-contamination, for example. It follows that the extent of measures that parties to armed conflict must take to avoid or at least minimize such reverberating effects also increases as the conflict prolongs.
In short, it is possible to establish the same level of confidence in the three-element (attack–water/wastewater service–infectious disease) consequential chain as in the double-element links between them, through a suite of robust epidemiological and damage assessment studies. The effort required to obtain this level of confidence is very much easier to specify than it is to execute, however. Combatants, lawyers, policy-makers and humanitarian organizations alike will thus inevitably be obliged to answer the earlier theoretical and practical questions about uncertainty. For the topic at hand, the question will be some variant of: if robust epidemiological and damage assessment studies cannot prove an outbreak of cholera was due primarily to the incidental damage inflicted by an attack on a wastewater treatment plant, does that mean that they are not linked?
Those seeking to quantify and reduce civilian harm during the conduct of hostilities must therefore decide how they will deal with uncertainty. The decision taken may matter little to humanitarian practitioners and those tasked to stabilize infrastructure and service delivery, considering how humanitarian work continues unabated by any equivocality.Footnote 108 The answer matters considerably for those involved in the conduct of military operations and, in particular, the targeting process, on the other hand, because they are compelled by their own targeting procedures to reduce the complexity of their operating environment and ensure compliance with the laws of armed conflict/IHL.
In the absence of the preferred level and quality of information, those who seek to reduce civilian harm should follow a “precautionary approach” which assumes the causal links and chains, and which is readily adapted to standard military operational planning process and targeting procedures.
Annex: Literature on the effects of war on WASH systems
Table A presents an incomplete list of documentation, mostly by humanitarian water engineers charged to repair water and sanitation systems damaged by military attacks. Read collectively, the reports reveal patterns about the influence of the resilience of the service before the attack occurs (or “baseline resilience”), cross-contamination between wastewater and drinking water, and, to a lesser link, observed links with outbreak or transmission of infectious diseases.
Table A. Published and unpublished literature on the effects of war on WASH systems










