


Open-source projects are initiatives to develop software or hardware ideas which are freely available solutions for use and modification (1). For open-source hardware instructions, knowledge and electromechanical parts or plans that allow the construction of a specific device are provided (2), for example, a self-replicating 3D printer (RepRap, http://reprap.org/). Open-source software (OSS) is a computer program for which the source code is freely published and available to the public, enabling anyone to copy and modify it without paying royalties or fees (1). The OSS community has existed for several decades, but the popularity of OSS increased after the success of the Linux operating system and the Apache Web server software (3). The advantages of the use of open-source technology in medicine (e.g., cost reduction and the ability for modification) have been the subject of several reports (Reference Ratib, Rosset and Heuberger4–Reference Jalbert and Paoli6). The disadvantages include difficulty in determining the costs associated with software implementation for a specific solution and lack of dedicated support online or by phone (Reference Erickson, Langer and Nagy7).
Open-source hardware is not applicable for FDA (U.S. Food and Drug Administration), European Union, or CE (Conformité Européenne) certification for general medical devices because it provides neither a well-documented workflow for production nor proper documentation. In contrast, OSS may receive FDA and CE approval and serve as an alternative to commercially available solutions, such as Osirix software (8;9). This study is a systematic review of the current literature on the use of OSS in dentistry, designed to answer the following research questions: (i) Which OSS packages for dental purposes are described in the literature? (ii) In which areas of dentistry is OSS used? (iii) How many OSS solutions are described in the dental literature? (iv) What is the reporting quality of studies on the subject of OSS?
MATERIALS AND METHODS
A single observer performed a comprehensive database search of PubMed (Medline), Web of Science, Science Direct, and Scopus on February 1, 2017. No time or language frame was applied. Only articles published in peer-reviewed journals were considered. Table 1 lists the combination of search terms which were translated into the appropriate equation for each database. A senior librarian was consulted to translate the equation correctly for other databases. The titles and abstracts obtained from the electronic search were screened and evaluated by two reviewers. Only articles that fell within the scope of the study (i.e., use or description of OSS in any dentistry fields) were retrieved. Studies related to open-source hardware, the use of OSS in general medicine or maxillofacial surgery only, and commercial software were excluded. Articles in the field of electronic health records and practice management were included because these topics are universal for all health care facilities.
Table 1. Search Output with Different Search Term Combinations

a The results were limited to the dental journals only.
b Truncation character - searches for the first 150 variations of a truncated term.
The same OSS solutions may be implemented in general dental practice and hospitals. General overview articles describing radiological OSS created to work with DICOM (Digital Imaging and Communications in Medicine) files were also included for the same reason. These studies do not perfectly match to dentistry, but these articles cannot be omitted to present this topic comprehensively. Radiology, health records management, and education are considered equally important as endodontics, prosthetics, and other branches of dentistry.
Discrepancies in the selection process were resolved by discussion. A PRISMA flow diagram illustrates the search and evaluation process (Figure 1). Two reviewers independently analyzed all of the included articles included using a data extraction form. The level of evidence of those articles was based on the study type, using the levels of evidence as described by the Oxford Centre for Evidence-Based Medicine (CEBM) (10). The studies were classified as: 1a, systematic reviews of randomized controlled trials (RCTs); 1b, RCTs; 2a, systematic reviews of cohort studies; 2b, cohort studies; 3a, systematic reviews of case-control studies; 3b, case-control studies; 4, case series; and 5, expert opinions.
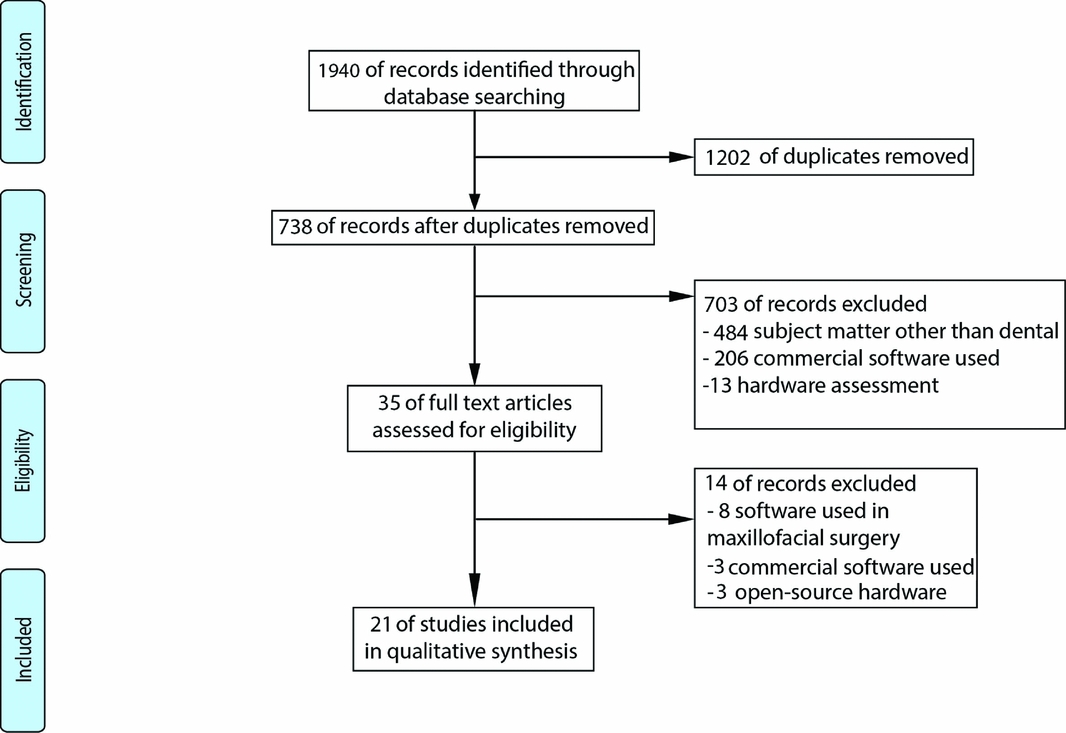
Figure 1. A PRISMA flow diagram illustrating search and evaluation process.
To assess the reporting quality of studies, the CASP Checklist was adopted and modified (11) (Table 2). Main as well as ancillary questions were retrieved and divided into four domains: internal and external validity, reliability, and objectivity. Also, three questions concerning software version, the use of comparison software, and availability of software for research purposes were added. When one or more of the key domains did not meet the criteria or was unclear, the overall study was judged as not high-quality or unclear quality. Conversely, the study was considered high-quality when all of the key domains met the requirements. Only articles of experimental studies were submitted to the reporting quality assessment. In the analysis of all the other studies, only the first three research questions were used.
Table 2. Critical Appraisal Criteria

This review was registered in PROSPERO, the International Prospective Register of Systematic Reviews, under number CRD42014010024.
RESULTS
A total of 1,940 articles were found, and following removal of duplicates by EndNote X5 reference manager software (Thomson Reuters, Philadelphia, PA) the search yielded 738 articles. The screening process based on exclusion criteria removed 703 articles, and a further fourteen records were excluded after full-text assessment of eligibility: in eight articles, the software described were for maxillofacial surgery applications, commercial software was used in three records, and open-source hardware was presented in three articles. The remaining twenty-one studies were included for data extraction (Supplementary Table 1) using the Patient-Intervention-Comparison-Outcome (PICO) algorithm (Reference Huang, Lin and Demner-Fushman30).
The twenty-one articles included ten experimental studies, three general overview articles, two survey studies, three descriptive reviews, one letter to the editor, one editorial, and one news article.
Twenty-six different OSS programs were described in the analyzed studies and ten of these programs were used for image visualization (Visualization Toolkit, ITK-Snap, Seg3D, 3DSlicer, Fiji, ImageJ, OsiriX, Xebra, 64-Bit MeshLab, 3DMeshMetric). Five OSS programs were used for healthcare records management (VistA, OSCAR, GEHR, OpenEMed, GALEN), four were used for educational processed (Supercourse, DentCPD, Moodle, Anki), one was used for remote consultation (Artma Virtual Patient) and simulation, and six were used for general purposes (Mozilla Thunderbird, GIMP, Open-office, InfranView, Wordpress, Piwik).
GENERAL OVERVIEW ARTICLES
Three articles were classified as overview studies: one article examined open-source solutions in medical information technology (Reference McDonald, Schadow and Barnes17), and two articles described the general aspects of software used in medical imaging (Reference Ratib, Rosset and Heuberger4;Reference Yoo and Metaxas29), McDonald et al. briefly described the history of open-source solutions, their licensing policy, and its role in medical (information technology), particularly patient health records (Reference McDonald, Schadow and Barnes17). An editorial for the Medical Image Analysis Journal written by Yoo and Metaxas focused on the potential outcomes, benefits, and co-founders of Insight software (Reference Yoo and Metaxas29). Another article provided an overview of the architecture and workflow of some available image-analysis OSS packages (Reference Ratib, Rosset and Heuberger4).
Education and Communication
Five articles described the usefulness of open-source solutions in education and communication. Wurche et al. evaluated the readership of a dedicated student blog-based online magazine using Wordpress technology (Reference Wurche, Klauer and Nürnberger28). A Letter to the Editor by Sa et al. mentioned an online lecture repository in epidemiology and prevention known as Supercourse (Reference Sa, Sekikawa, Linkov, Lovalekar and LaPorte19). This project attracted approximately 10,000 participants from 138 countries who collaborated as users or reviewers. Importantly, El Tantawi et al. analyzed the experience of a limited-resources dental school with e-assessments (Reference El Tantawi, Abdelsalam, Mourady and Elrifae15). The authors used an online survey to monitor students’ attitude and problems related to e-assessments provided by the OSS system.
Another study evaluated students’ perception and use of an electronic-spaced repetition oral pathology-radiology system in dental hygiene education and predoctoral dental education (Reference Al-Rawi, Easterling and Edwards12). Kossioni et al. reported on the design and testing processes of an online module created for continued professional development (Reference Kossioni, Kavadella and Tzoutzas16). The primary area of interest of the tested e-module was “Sterilization and cross-infection control in the dental practice.”
Oral Implantology
Two studies presented OSS application to oral implantology. Chen et al. described the modification processes of Insight ToolKit and Visualization ToolKit as one of the steps in their experiment on the accuracy of a stereolithographic surgical guide (Reference Chen, Yuan, Wang, Huang and Kang13). The second study presented “telenavigation client” software that allowed multiple users to participate on-line during implant surgery by means of real-time tracking of surgical device position with an attached tracking sensor (Reference Truppe, Schicho, Kawana and Ewers24).
Radiology
The principal area of interest of three articles was dental radiology. One article appraised postprocessing image protocols available as OSS to identify the best method to search and measure additional mental foramen within cone-beam computed tomography (Reference Santos, Pinheiro, Umetsubo, Sales and Cavalcanti20). A second study briefly reviewed the possible use of OSS with the use of Really Simple Syndication (RSS) technology and offered examples of some applications for e-mail management, word processing, spreadsheets, database, presentation creation, and image editing (Reference Scarsbrook5). A study by Erickson et al. provided an overview of the basics of OSS and discussed its potential impact on radiology development (Reference Erickson, Langer and Nagy7).
Orthodontics
Three studies addressed OSS in orthodontics. One study comparatively analyzed the accuracy of two open-source and four commercial software solutions (Reference Weissheimer, Menezes and Sameshima27). This comparison was performed in three-dimensional (3D) measurements of upper airway volume in growing patients. Sicurezza et al. measured the orbital volume in patients treated with rapid maxillary expansion using Osirix software (Reference Sicurezza, Palazzo and Leonardi21). The third study by Ruellas et al. presented and evaluated a 3D coordinate system for assessments of directional changes (Reference Ruellas, Tonello and Gomes18). This study was based on the 3D computed tomography reconstructions of facial skeletons prepared in ITK-Snap and transferred and re-oriented in a 3D Slicer.
Health Records and Practice Management
One of the articles examined the use of OSS for electronic health records (Reference Webster26). Webster briefly described the advantages of open-source health record systems and provided three examples (the Veteran Health Informatics System and Technology Architecture, the Canadian open-source electronic medical record system OSCAR and a District Health Information System).
Endodontics
Four studies described the use of OSS in endodontics. DeDeus performed an experimental study which was the only article to meet all of the quality appraisal criteria (Reference De-Deus, Marins and Neves Ade14). The authors assessed the accumulation of hard-tissue debris inside the root canal after biomechanical instrumentation. Two studies by Silva et al. compared the use of Fiji OSS in canal transportation after instrumentation with different rotary root canal instruments (Reference Silva, Muniz and Pires22;Reference Silva, Vieira and Tameirão23). Another article, by Villoria et al., assessed the use of OSS in monitoring of the periapical lesion healing after endodontic treatment (Reference Villoria, Lenzi and Soares25).
No reports about the use of OSS in periodontics, prosthetics, and conservative dentistry were found.
An analysis of the level of evidence revealed that no articles had level 1 evidence, and five studies were level 2b (Supplementary Table 1) (Reference Ruellas, Tonello and Gomes18;Reference Sicurezza, Palazzo and Leonardi21–Reference Silva, Vieira and Tameirão23;Reference Weissheimer, Menezes and Sameshima27). After the quality reporting assessment (Table 3), only one of the articles was considered high quality, fulfilling all of the criteria (Reference De-Deus, Marins and Neves Ade14). Sicurezza et al. was graded “unclear” because of lack of information about a possible conflict of interest (Reference Sicurezza, Palazzo and Leonardi21).
Table 3. Critical Appraisal of Experimental Studies

Note. +, high-quality note; −, non high-quality note; ?, unclear quality note. The lowercase letters indicate questions from Table 2 with negative or unclear note.
DISCUSSION
During our research, we found only a small number of studies on the use of OSS in dentistry. Although the conclusions drawn from studies support the use of OSS, most of the articles presented a low level of evidence (3b-5) and poor quality of reporting, which makes it difficult to recommend OSS as a clinically useful software. The only study with high-quality reporting was a case-controlled study but the conclusions were based on very small research group, three teeth, in what way does it not make it possible to say that the results are representative.
Four of five studies with the highest level of evidence (2b) examined clinical changes in orthodontics (influence of head orientation on directional changes in 3D space; orbital volume and aperture width changes after rapid maxillary expansion) (Reference Ruellas, Tonello and Gomes18;Reference Sicurezza, Palazzo and Leonardi21) and endodontics (canal transportation) (Reference Silva, Muniz and Pires22;Reference Silva, Vieira and Tameirão23), but none of the identified studies included a comparison between OSS and any other software. The only level-2b study that included a comparative analysis of a commercial and open-source software was assessing software precision in airway volume measurement (Reference Weissheimer, Menezes and Sameshima27). The study was based on 33 participants and lead to the conclusion that the use of Osirix and ITK-Snap OSS presented clinical value.
The usability of OSS was evaluated only in a few areas: mental foramen localization, upper airway calculation in growing patients, an experimental assessment of hard debris in the root canal system after root canal treatment, information gathering (RSS), practice management, and use for educational purposes. None of the studies revealed the use of OSS in prosthodontics which is currently the most intensively developing area of digital dentistry. Virtual planning and design of prosthetic reconstructions provide many opportunities for OSS solutions.
Another aspect of the use of OSS in dentistry is education: 10,000 participants from 138 countries used the Supercourse e-module entitled, “Sterilization and cross-infection control in a dental practice”, which makes this software one of the most popular e-lectures on this topic (31). Supercourse is a network of 56,000 scientists from 174 countries who share a free library of 5,802 lectures in thirty-three languages, but it contains only eleven lectures on dental topics. These numbers are impressive, but several issues regarding the use of open intellectual property, a unified rating system and a standard citation system may require proper regulation (Reference Sa, Sekikawa, Linkov, Lovalekar and LaPorte19;Reference Eysenbach and Sa32).
Free on-line distribution and the bypassing of intermediary vendors suggests that OSS is observed as an alternative to commercial software which should be considered with caution. This fear is a misinterpretation because the distribution of OSS lessens the potential for financial gain, but more clearly defines the role of vendors as providing professional services, such as implementation and maintenance. With no possibility for benefit from the sale of a particular solution, a reduction in the number of potential sponsors from national institutions and potential user communities is common (Reference Yoo and Metaxas29). Donations or grants for OSS could produce substantial savings for national or international institutions, such as the European Commission or the U.S. Veterans Health Administration. For example, the implementation cost of the VistA hospital management software is 40-fold less than any commercial solution, but it still requires 20,000 hours of programming (Reference Webster26). However, OSS should not be considered a panacea for any problem. Open-source code allows a wider audience for reviews, but free access makes it susceptible to hacking and data theft (33). Therefore, OSS is discouraged for the management of a confidential database.
The evaluation of OSS in medicine should not be overlooked. Professional medical certification (FDA and CE) often cannot be applied to OSS because it requires a legal commercial entity for distribution liability and support availability. It is also important that FDA and CE certification confirm that the software and its provider ensure an error-free workflow, but not the accuracy of software actions/calculations, and provide appropriate documentation and support. Therefore, experimental studies and algorithm evaluations should be conducted and published. The establishment of a dedicated section in peer-reviewed journals in which the medical and technical aspects of specific software packages and their applications could be presented simultaneously is one possible solution, and this would also provide a standard citation system for OSS creators and developers. Medical ratings, such as the impact factor and the number of citations, may provide sufficient credit for software creators and could encourage the next generation of researchers to join open-source projects. The Review App Series in the Journal of Digital Imaging, which started in September 2014 (Reference Shih34), provides an interesting example of such a solution. In brief reports, authors subjectively assess the pros, cons, usability and proposed potential improvements of mobile apps for digital imaging.
It should also be emphasized that our research was limited to the articles that clearly stated that the presented software was OSS. Studies without such information in their text, abstract, title, or keywords were not included. We believe that the inclusion of information that the technology used in a particular study was open-source could be important for future analyses.
CONCLUSIONS
Our review results showed that the medical literature on the topic of OSS in dentistry is limited and includes mostly expert opinion and case-control studies. The authors of the current study suggest that OSS should be added to the MeSH keyword tree to facilitate classification of studies including open-source software. It will also make it easier to find appropriate OSS solutions for specific indications, which can play an important role in the implementation of digital solutions in some rare fields where strong financial efforts would be economically unjustified.
The second suggestion is to include OSS as a control group in experimental studies on software validation. Such comparative analysis can have positive effects for the commercial programming vendors by showing them the most advantageous OSS solutions that can be deployed into commercial software packages.
It may also be beneficial for customers who, apart from obtaining detailed information on the performance of software packages, might be able to decide if the risk of using OSS without technical support and requiring greater computer skills is justified in specific cases.
SUPPLEMENTARY MATERIAL
Supplementary Table 1: https://doi.org/10.1017/S0266462317000708
CONFLICTS OF INTEREST
The authors have nothing to disclose.






