



Health systems around the world are faced with complex challenges: rapid changes in technology; pressures to include new interventions for prevention, diagnosis, therapy, or rehabilitation; population aging; and health budgets that represent a greater proportion of countries' gross domestic product year after year.
Health systems in Latin America and the Caribbean (LA) face the same complexities as other health systems around the globe regarding new technologies but with the additional burden of working toward establishing and strengthening universal health coverage (UHC) and to reduce the profound inequalities and inefficiency that persist (Reference Dmytraczenko and Almeida1–Reference Cotlear, Gómez-Dantés and Knaul3).
Health technology assessment (HTA) plays a central role in the decision-making process for the prioritization of health system resources and to assess the potential value and impact of including a technology in a benefits package (4).
HTA is seen as a bridge between the worlds of research, regulation (the responsibility of regulatory agencies that approve market access), and coverage or reimbursement decision making; however, achieving this in reality can be difficult (Reference Velasco, Finn and Kristensen5). One of the main barriers is the fact that these three domains of research, regulation, and decision making hold different objectives, languages, motivation, values, training, and institutional processes. Decision makers, especially those who are responsible for health system budgets, need information that is context specific and directed to a particular question for decision making. For these reasons, information must be available at an appropriate time, be reliable, concise, and written in understandable language (Reference Drummond, Schwartz and Jönsson6;7). In contrast, the world of research generates less context-specific information that is the product of studies using rigorous methodological approaches such as randomized clinical trials which are generally less compatible with decision-making timelines and less representative of the day-to-day realities of the health system (Reference Rotstein and Laupacis8). Significant differences also exist between the world of decision making and that of regulatory approval where, in the latter, the variables considered for market access approval as well as the attributes considered as valid (quality, safety, efficacy) are not the same as those used in decision making for the allocation of health system resources, which focus on dimensions such as effectiveness or cost-effectiveness (Reference Eichler, Bloechl-Daum and Abadie9).
HTA is presented as a mechanism that can mediate between the worlds of research and decision making (Reference Rotstein and Laupacis8). However, for this mechanism to work adequately, those that produce and work in HTA must understand the needs, values, and processes of the decision-making world. Decision makers, for their part, must understand and have confidence in the HTA process.
While it is relatively easy to agree on what constitutes a good HTA, it is much more difficult to determine what are the elements and processes of a good decision and the way that HTA and decision making should be linked. Despite these challenges, it is broadly accepted that having a clear link between the assessment and decision making is a principle of good practice in HTA, as recognized both at the international level and in LA countries (Reference Pichon-Riviere, Augustovski and Rubinstein10;Reference Pichon-Riviere, Soto, Augustovski, García Martí and Sampietro-Colom11).
For the past 15 years, Health Technology Assessment International (HTAi) has organized the Global HTA Policy Forum that aims to provide a neutral space for strategic discussions on the current state of HTA, its development, and the implications for health systems, industry, patients, and other stakeholders (12;13). In 2016, the first Latin American Policy Forum (LatamPF) was held in Costa Rica. At that Forum, participants further advanced work on the good practice principles of HTA that should be followed in the region, and the presence of a clear link between the assessment and decision making was identified as the highest priority principle to be improved and strengthened in LA countries (Reference Pichon-Riviere, Soto, Augustovski, García Martí and Sampietro-Colom11). This topic was the focus of debate in the fourth Latin America Policy Forum (2019) where the objective was to explore how to improve the link between HTA and decision making in the countries of the region.
This paper presents the main results of the Forum. It is not a formal consensus document and it should not necessarily be interpreted as a representative of the views of the participants or organizations in which they work.
Methods
The scientific secretariat (Institute for Clinical Effectiveness and Health Policy, IECS Argentina) prepared a background document on the link between HTA and decision making (Reference Pichon-Riviere, Garcia Martí, Alfie, Augustovski and Sampietro-Colom14). For this, they conducted a literature search, document review, and search of HTA agency and government Web sites to identify the characteristics of the link between HTA and decision making in a series of countries (Germany, Australia, Brazil, Canada, Scotland, England, and Thailand). The main objective of this document was to build a common understanding among the participants, to harmonize the definitions of key terms, and to facilitate discussions at the in-person meeting (available at http://www.htai.org). The HTA process, and subsequent decision making, was conceptualized as a process with four main phases: (i) identification and prioritization of technologies for assessment; (ii) assessment; (iii) appraisal; and (iv) decision making.
In addition, with the aim of including basic information about the current situation in the region, the background document was accompanied by the results of a survey of the representatives of participating countries that was administered ahead of the in-person meeting to gather information about the characteristics of the process of decision making and the link with HTA.
The in-person meeting of the fourth LatamPF was held in Buenos Aires on 29 and 30 April 2019. There was a total of fifty-four participants: thirteen representatives of HTA agencies and eight representatives of payers from the public, social security, and private sectors; twenty-one representatives from industry in the areas of drugs, medical equipment, and diagnostic tests; one representative from the Pan-American Health Organization; two representatives from patient associations; two representatives from HTAi; and seven academics, organizers, and members of the scientific secretariat of the event. In total, there were twelve countries from the region represented (Argentina, Brazil, Chile, Colombia, Costa Rica, Ecuador, El Salvador, Mexico, Panama, Paraguay, Peru, and Uruguay). Presented in the Acknowledgements section is a list of the participants, their affiliations, and countries.
The format of the in-person meeting included plenary presentations, breakout groups (n = 4), and plenary discussions.
The event began with a presentation on the characteristics of the link between HTA and decision making in Europe, Asia, England, the United States of America, and Canada delivered by Brian O'Rourke, President and CEO of the Canadian Agency for Drugs and Technologies in Health (CADTH). The current situation in the region was presented by the representatives of five countries (Argentina, Chile, Colombia, Mexico, and Peru) who described the characteristics of the current links between HTA and the decision-making process, along with the main challenges faced. These were followed by presentations from the representatives of the medical device industry and a patient representative to provide their perspectives on the topic.
Two working group activities were conducted using an abbreviated design-thinking methodology (Reference Johansson-Sköldberg, Woodilla and Çetinkaya15;Reference Brown16) that was tailored to meet the objectives, timeline, and dynamics of the Forum. Each group was led by a facilitator trained in the method and a scribe to take notes. Afterwards, the results of the breakout groups were reported and discussed in two plenary sessions. This methodological approach was designed through several meetings of the research team with the Qualitative Health Research Unit at IECS, who also collaborated in the design and selection of materials to use and in the training of the facilitators.
The objective of the first group activity was to discuss and analyze the present situation in the region regarding the link between HTA and decision making. First, for each of the phases of the HTA process, positive and negative examples of this link were identified from among the current experiences in the region. Positive examples were defined as those characteristics or processes that improve the link between HTA and decision making or that make this link more appropriate. Participants began by writing examples of what, in their view, would be positive or negative experiences, they then shared these experiences with the other participants and through a group discussion, each group voted to select examples that were considered the most representative. Starting from these examples, the groups then debated the main consequences of a lack of a link between HTA and decision making in the region and selected those which they considered to be the most relevant. They also discussed the barriers and facilitators to strengthening the link between HTA and decision making.
The second breakout group activity was to identify for each of the phases of HTA, and in reference to international experiences, the most relevant attributes that could lead to a more effective link between HTA and decision making. In the groups, participants began by each proposing at least three attributes for each of the phases of HTA and they compiled a common list of agreed attributes. Next, each group voted to identify from the recently created list those actions and attributes of the highest priority for promotion in the countries in LA, taking into account their relevance to improving the link between HTA and decision making and the gap between their ideal and real levels of application in LA. The second group activity also included a discussion to identify success stories in the real world that serve as good examples of how to improve the link between HTA and decision making and what could be the main actions to implement in the region.
The Forum was conducted under the Chatham House Rules (17). All materials were produced in Spanish and English. The Spanish version of this paper is available: https://doi.org/10.1017/S0266462320000045.
Results
The country presentations showed that important advances have been made in the region with many cases where the link between HTA and decision making has been developed and strengthened, despite the heterogeneous levels and significant differences across as well as within countries with complex and fragmented health systems. In some cases, recent changes in government affected the continuation of some projects. In all cases, countries reported pending actions and areas for improvement to the link between HTA and decision making. In the survey on the characteristics of the decision-making process and the link with HTA in LA, it was revealed that only four of the twelve countries participating in the Forum have established an explicit process for the prioritization of technologies for assessment, and only five of the twelve countries have established a regulatory framework that links HTA formally with decision making. Furthermore, the survey results showed that the involvement of stakeholders is still limited in most of the countries. Supplementary Material 1 contains the full results of the survey.
Presented below are the main findings of the qualitative analysis of the following aspects: (i) positive and negative examples in the region of the link between HTA and decisions; (ii) the consequences for the health system due to an inadequate link between HTA and decision making and the barriers and facilitators to improving this; and (iii) the characteristics, attributes, and processes of highest priority for implementation in the health systems of Latin America so as to improve the link between HTA and decision making. The Supplementary Material provides further detail of these results.
Positive and Negative Examples in the Region of the Link Between HTA and Decisions
Table 1 presents a summary of the actions and experiences of the countries that were case examples of the positive and negative links to decision making in each of the HTA phases. Positive examples were those processes or situations in which the participation of different stakeholders was achieved (e.g., cases where the participation of different stakeholders is considered systematically in the prioritization process or where countries and health systems are already including patients, industry, and other stakeholders in the assessment process); where there were transparent rules to guide the different phases of HTA (e.g., agencies and countries that publicly release the HTA documents upon which decisions will be made, or that have clear rules about information requirements or the form in which different stakeholders can participate); and those concrete cases where a positive change was observed as a result of the HTA mechanism (e.g., the avoidance of incorporating an ineffective or unsafe vaccine, or achieving the inclusion of a new comparator that was identified through the appeal process and which would not have been otherwise considered, or the inclusion of HTA recommendations in clinical practice guidelines).
Table 1. Examples of Actions that Improve or Weaken the Appropriate Link between HTA and Decision Making

Negative examples included deficient prioritization processes, for example, cases where countries or health systems had sufficient mechanisms for identifying technologies but no clear prioritization process, meaning that many of the technologies identified were never assessed, or cases where political pressure was a determining factor in the prioritization of technologies to assess. The negative examples also showed situations where judicialization, or excessive political or interest group pressure distorted the link between HTA and decisions (e.g., to influence the selection of technologies to be assessed or to directly influence the assessment and/or decision-making process).
Furthermore, situations were identified where an inadequate link between HTA and decision making resulted in an inefficient process and suboptimal results for the health system (e.g., when interventions and technologies receive a favorable recommendation but are not included in the benefits package, or, alternately, cases where interventions are adopted by the health system despite having contrary information that was not considered during the decision-making process).
Consequences for the Health System due to Inadequate Links Between HTA and Decision Making and Barriers and Facilitators to Improvement
From the examples previously discussed, participants identified the main negative consequences of the inappropriate connection between HTA and decision making that currently affects many of the health systems in LA. These are listed in Table 2. The main consequences are associated with how the HTA process is perceived (e.g., a lack of legitimacy of decision making, stakeholders who feel excluded) and the difficulty to achieve the objectives of the HTA (e.g., inadequate implementation of decisions, delays, and inefficient use of resources).
Table 2. Current Situation in Latin America: Main Consequences of an Inadequate Link between HTA and Decision Making

The breakout groups identified a series of barriers and facilitators to improve the link between HTA and decision making in the region, which are detailed in Supplementary Material 2. The barriers include structural aspects such as institutional weakness (i.e., lack of an adequate framework for institutionalization in many of the countries) or limited technical resources (both in terms of quantity and training) and economic resources for HTA in the region as well as more general aspects of the health systems and countries such as excessive judicialization, the lack of training for different stakeholders, the lack of continuity in policies (related to changes in government), or limited data and local information that would help produce sufficiently contextualized assessments.
On the other hand, the current moment is considered to be a time of political readiness in LA to introduce changes in how HTA is linked to decision making. There is better knowledge and understanding of these issues among stakeholders, there are significant international experiences that can be drawn upon, HTA processes have been established in many countries in the region, and there are regional mechanisms to facilitate cooperation.
Priority Improvements to be Implemented in the Health Systems of Latin America and Recommended Actions
Taking action to strengthen the link between HTA and health system decision making requires that health systems in the region be characterized by a series of attributes, elements, and/or processes. Most of the attributes considered to be high priority, and also which could be feasibly implemented in the region in the short to medium term, relate to increasing the participation of different stakeholders, and improving the transparency of the HTA process along with the establishment of a legal framework and/or formal process that explicitly links decisions with HTA and the production of recommendations.
In Table 3, these priority attributes are listed for each of the phases of HTA. The complete list is available in Supplementary Material 3.
Table 3. Characteristics, Attributes, Elements and Processes of Highest Priority to be Implemented in Health System in Latin America to Improve the Link between HTA and Decision Making

Once the barriers and facilitators to strengthening the “HTA-decision” link were identified, and the priority attributes of health systems that enable good implementation, a series of concrete actions was then suggested for the short and medium term for the advancement and improvement of the way HTA is linked with decision making in LA. These include actions recommended for the HTA agency level, for changes at the level of the health system, and for actions at the regional and global levels. Table 4 shows the main actions that were recommended.
Table 4. Main Actions Recommended to Improve the Link between HTA and Decision Making in the Region
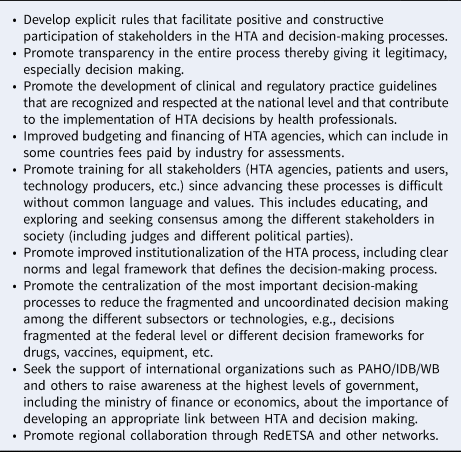
PAHO, Pan American Health Organization; IBD, Inter-American Development Bank; WB, World Bank.
Policy Implications
An appropriate link between HTA and resource allocation decision making is a key element for all health systems. At the international level as well as in the region, an appropriate link between HTA and decision making has been acknowledged as fundamental, and without this, the HTA process itself is at risk (Reference Drummond, Schwartz and Jönsson6;Reference Pichon-Riviere, Augustovski and Rubinstein10;Reference Pichon-Riviere, Garcia Martí, Alfie, Augustovski and Sampietro-Colom14). Although there have been important advances in the region, the current deficiencies in the link between HTA and decision making are diminishing the legitimacy of decisions made based on HTA as well as their appropriate implementation, resulting in the suboptimal implementation of coverage policy. They also expose the HTA process to excessive political, administrative, and/or judicial influence; to decisions that imply an inefficient use of resources; and to stakeholders who are excluded from the assessment and decision-making process. This is not surprising in light of the survey results which showed a low degree of formal linkage between HTA and decision making in twelve of the countries participating in the Forum.
While the characteristics and values of the health systems in the region are heterogeneous, there are some common areas of application across the countries to help strengthen the link between HTA and decision making and which were mentioned repeatedly during the Forum. Some aspects to highlight were: (i) to strengthen the institutionalization of HTA in countries that have not yet done so through the sufficient allocation of technical capacity, time, and financial resources; (ii) improve the transparency of the decision-making process as a key aspect for its improved legitimacy, for example, defining the criteria upon which coverage decisions are made and by the active inclusion of all relevant stakeholders in all phases of the process from topic selection to the assessment and final decision; (iii) to review the process and levels of decision and improve coordination, which is important given the usual state of fragmentation of decision making currently seen in many of the countries in the region with regards to medicines, vaccines, and equipment, or at the federal and provincial level, or between different health subsystems.
Forum participants agreed that in the region currently, there is a window of opportunity since the topic is seen as a priority by the majority of actors in society with the added momentum from the World Health Organization and the Pan American Health Organization to include HTA as an essential tool to help health systems to achieve UHC (7). The Latin American HTA Policy forum has provided further insights to support this advance. It now depends on the different health system stakeholders in the region, including politicians, HTA professionals, technology producers, patients, and citizens, to seize upon and maximize this opportunity to strengthen the link between HTA and decisions about the coverage of health services.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0266462320000033.
Acknowledgments
Thank you to the event participants for their valuable contributions: Adriana María Robayo García (Instituto de Evaluación Tecnológica en Salud [IETS]—Colombia), Alexandre Lemgruber (Pan American Health Organization [PAHO]—United States of America), Alicia Ferreira (Fondo Nacional de Recursos—Uruguay), Alicia Granados (Sanofi—Spain), Ana Eduviges Sancho Jiménez (Ministry of Health—Costa Rica), Ana Pérez Galán (Ministry of Public Health—Uruguay), Analía López (Secretaría de Salud, Ministry of Health and Social Action—Argentina), Andrea Alcaraz (IECS—Argentina), Ariosto Matus Pérez (Roche—Mexico), Aurélio Yamada (BioMarin—Brazil), Brian O'Rourke (CADTH—Canada), Carlos Mendoza (Edwards Lifesciences—Mexico), Chris Carvalho (HTAi—Canada), Dino Sepúlveda Viveros (Ministry of Health—Chile), Eva María Ruiz de Castilla (Latin American Patient Academy—United States of America), Fabiana Raynal Floriano (Ministry of Health—Brazil), Fernanda Laranjeira (Janssen-Cilag—Brazil), Gabriela Rodriguez (IECS—Argentina), Giovanni Guevara Vazquez (Ministry of Health—El Salvador), Hector Castro (MSH; HTAi—Colombia), Homero Monsanto (Merck & Co.—United States of America), Isabel Peirano (Novartis—Argentina), Jeremias Bernal Gascón (Ministry of Health PTY—Panama), Jimena Morales Ayala (Consejo General de Salud—Mexico), Johanna Guambo (Ministry of Public Health—Ecuador), Joice Valentim (Roche Pharma—Suiza), Jose Luis Montes (MSD—Argentina), Juan Luis Gerardo Durán Arenas (Instituto Mexicano de Seguridad Social—Mexico), Juan Valencia (Medtronic—United States of America), Julian Arcos (Medtronic—Colombia), Kariluz Maestre (Novartis—Colombia), Katelyn Pretzlaff (HTAi—Canada), Lizbeth Acuña Merchán (Cuenta de Alto Costo—Colombia), Manny Papadimitropoulos (Eli Lilly—Canada), Marjorie Obando Elizondo (Fondo de Seguridad Social de Salud de Costa Rica [CCSSS—Costa Rica]), Mercedes MacMullen (Pfizer—Argentina), Mohit Jain (BioMarin—United Kingdom), Natalia Zarino (Eli Lilly—Argentina), Nicolás Nobile (AMGEN—Argentina), Pablo Denamiel (Superintendant of Health Services—Argentina), Patricia Caballero (National Health Institute—Peru), Pedro Galván (Instituto de Investigaciones en Ciencias de la Salud—Paraguay), Silvana Kelles (UNIMED-BH—Brazil), Solana Terrazas Martins (Ministry of Health—Chile), Stefan Weber (AMGEN—Suiza), Valeria Liegard (Johnson & Johnson—Argentina), Vania Cristina Canuto Santos (Ministry of Health—Brazil), Virginia Llera (Geiser Foundation—Argentina), William Dorling (Pfizer—United Kingdom). We also thank Tara Schuller for her work in translating the manuscript from Spanish to English.
Funding
The organization of and participation in the Forum was funded by Health Technology Assessment International (HTAi). The preparation of the manuscript was completed by the Institute for Clinical Effectiveness and Health Policy (IECS) with funding support from HTAi.






