Ankylosing spondylitis (AS) is a prototype, subtype, or clinical outcome of spondyloarthritis (SpA), especially axial SpA (Reference Rudwaleit, Listing, Brandt, Braun and Sieper1). Among the available options for AS treatment, anti-tumor necrosis factor (TNF) therapy has become increasingly popular. However, several studies have reported high remission rates in AS patients following treatment (Reference Navarro-Sarabia, Fernandez-Sueiro and Torre-Alonso2). In addition, the United States Food and Drug Administration (FDA) has approved a number of TNF blockers for AS and indicate 50 mg of etanercept to be administered once weekly. Etanercept is a recombinant protein of p75 TNF receptor as a competitive inhibitor binding of TNF-alpha to cell-surface TNF receptors (Reference Goldenberg3). However, there is a discrepancy between the approved dosing regimen and that used in a related clinical trial (4), which demonstrated that a 25 mg twice-weekly regimen of etanercept was effective for the treatment of AS. Such discrepancies could cause confusion in the future selection of an appropriate dosing regimen (Reference Maxwell5).
Discrepancies in etanercept dosing regimen and duration of therapy for the treatment of AS patients also existed in prior studies. For example, McCormack et al. (Reference McCormack and Wellington6) recommended a twice-weekly dosage of 25 mg, but a clinical trial with active rheumatoid arthritis patients showed comparable efficacy and safety results between 50 mg once-weekly and 25 mg twice-weekly treatments (Reference McCormack and Wellington6). Additionally, several meta-analyses have been conducted to evaluate the efficacy and safety of anti-TNFs, especially etanercept treatment for ankylosing spondylitis (Reference Li, Zhang, Wang and Shi7–Reference Maxwell, Zochling and Boonen9). Some recent systematic reviews have tried to determine the optimal dosing regimen and duration of therapy for etanercept use (Reference Baji, Pentek and Szanto8;Reference Maxwell, Zochling and Boonen9) However, the findings of these studies were somewhat less robust, owing to the lack of updated clinical trials, analysis issues, and not providing outcome measures commonly recommended for evaluating efficacy of treatment for ankylosing spondylitis by experts (Reference Sieper, Rudwaleit and Baraliakos10).
There is still a need to verify the ideal dosing regimens and therapy duration for etanercept in the treatment of AS patients. To do this, using multifocal indices, we conducted a meta-analysis of recently published randomized controlled trials (RCTs).
METHODS
This review was conducted according to the Cochrane Collaboration Handbook (Reference Green, Higgins and Alderson11) and reported in accordance with the Preferred Reporting Items for Systematic Review and Meta-analysis guidelines (Reference Moher, Liberati, Tetzlaff and Altman12).
Data Sources and Search Parameters
The following major medical databases were searched: PubMed, Embase, Cochrane Library, and Web of Science. We designed and applied a search strategy using sensitivity criteria filtering for RCTs for etanercept including patients with AS. The search strategy is described in Supplementary Table 1. References of related articles were hand-searched, and the “Related Article” feature was used to discover additional articles while excluding unpublished dissertations or theses. Language was not restricted during the article search.
Table 1. Characteristics of the RCTs Included in the Analysis

ETN, etanercept; RCT, randomized controlled trial; OLE, open-label trial; Belgium, BE; Canada, CA; CN, China; DE, Germany; FR, France; FI, Finland; GR, Greece; AN, Netherlands; PL, Poland; PT, Portugal; HUN, Hungary; US, United States; IT, Italy; ES, Spain; United Kingdom, UK; qw, once weekly; biw, twice weekly
Study Selection
Two examiners independently screened the titles, abstracts, and full texts of articles to identify relevant studies for inclusion in the meta-analysis. Discrepancies in results were resolved by discussion. The efficacy and toxicity outcomes of interest in the RCTs were searched for by two independent investigators. Only trials that used randomized controlled study designs to compare the efficacy or safety between etanercept and a placebo were included. Studies included patients with radiographic axial SpA, which was defined as that satisfied the definition of the modified New York criteria, and nonradiographic AS, also termed early AS and defined by a score of 4 or more on the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) (Reference Rudwaleit, Listing, Brandt, Braun and Sieper1). Studies with less than 10 participants were excluded.
Data Extraction and Outcomes of Interest
Two reviewers separately collected the following relevant data: publication year, study design, study population, number of patients, previous or simultaneous use of disease-modifying anti-rheumatic drugs (DMARDs), nonsteroidal anti-inflammatory drugs and/or glucocorticoids, intervention, and outcomes. The primary outcome was measured by a population-pooled odds ratio (OR) showing the Assessment of SpondyloArthritis International Society 20 (ASAS 20) response, which was defined as a decrease of at least 20 percent and 10 units (on an illustrated analog scale from 0 to 100) in at least three of the following categories: patient global assessment, lumbar pain, physical function, and inflammation (without exacerbation >20 percent and 10 units in the remaining fourth category).
The ASAS 20 response represents the efficacy of the treatment (Reference Rudwaleit, Listing, Brandt, Braun and Sieper1). The secondary endpoints were assessed from BASDAI and BASDAI 50 responses. The BASDAI is widely used and was designed by medical professionals in conjunction with patients. The BASDAI gathers the patient's response to a self-administered questionnaire containing six questions regarding the symptoms of AS. The BASDAI 50 is a 50 percent improvement in the BASDAI score, and it represented the proportion of patients with improvements of at least 50 percent from the baseline value of the BASDAI. The Bath Ankylosing Spondylitis Functional Index (BASFI) (Reference Rudwaleit, Listing, Brandt, Braun and Sieper1) reflects the degree of disability in patients with AS. Other secondary outcomes that were evaluated included safety and adverse reactions.
Assessment of Bias Risk
The risk of bias in the clinical trials was assessed using the Cochrane Risk of Bias tool (Reference Green, Higgins and Alderson11) with respect to randomization allocation, double blinding, and description of withdrawals. Every domain was categorized as having a low, high, or unclear risk of bias. If the explanation in the report could not be classified as high or low, it was considered “unclear.” Two independent reviewers evaluated the methodological quality of the studies and resolved disparities by discussion. The methodological quality was examined according to the Jadad scale (Reference Moher, Cook, Eastwood, Olkin, Rennie and Stroup13), which assigns a study score ranging from 0 to 6, with 6 denoting the highest quality.
Data Synthesis and Analysis
Data from the eligible studies were entered into the Review Manager 5.1 software (version 5.1.2, The Nordic Cochrane Center, The Cochrane Collaboration, 2011). Concerning continuous data, the mean difference was calculated to perform the analysis. The mean difference was used for continuous data with 95 percent confidence intervals (CIs). The results were expressed as risk ratios (RRs) with CIs for dichotomous outcomes. Higgins’ I2 statistic and the chi-square-based Q-test were used to assess heterogeneity among studies and subgroup differences. The heterogeneity was denoted by p < .10 and/or I 2 > 40 percent. Factors that affected heterogeneity were investigated in positive cases (Reference Green, Higgins and Alderson11).
A random-effects model (the DerSimonian and Laird method) was used to analyze pooled data according to heterogeneity; otherwise, a fixed-effects model was used (the Mantel–Haenszel method) (Reference Green, Higgins and Alderson11). The statistical significance (p < .05) of the pooled ORs was determined by the Z-test. Publication bias in the literature was assessed by Egger's linear regression test, and visual inspection of asymmetry was performed in funnel plots. If a publication bias was present, p-values examined by Egger's test would have resulted in less than .05 (Reference Egger, Davey Smith, Schneider and Minder14). The “trim and fill” method was used to correct publication bias, which was made to correct the funnel plot by imputing where the missing studies would be likely to occur (Reference Duval and Tweedie15). The correction for missing studies could lead to relevant changes regarding the weighted mean effect, so the influence of the publication bias for the statistical significance in the overall effects was also evaluated (Reference Duval and Tweedie15).
RESULTS
Studies and Their Main Characteristics
A flow diagram of the clinical trial selection process is shown in Figure 1. A total of 2,079 articles were identified through a database literature search, and manual searching revealed additional reports. After eliminating duplicates, 2,067 records were retrieved. Ultimately, eleven RCTs that evaluated the efficacy and safety of etanercept in comparison with a placebo were included in the meta-analysis. The main characteristics of the RCTs included in this analysis are shown in Table 1. The total number of patients included in the meta-analysis was 1640, and the trials were performed in Europe, Asia, the United States, and South America.

Figure 1. Flow diagram of the selection process for the included studies.
Clinical outcomes that demonstrated the efficacy and safety of etanercept in the treatment of AS were evaluated in the RCT phase in all studies (Reference Dougados, Braun and Szanto16–Reference Huang, Zhang and Huang26). To determine the differences in the efficacy and safety of etanercept, we analyzed the results obtained in the randomized controlled phase: four studies (Reference Pang, Wang and Suo19; Reference Lin, Lin and Gu21;Reference Brandt, Khariouzov and Listing24;Reference Huang, Zhang and Huang26) continued therapy for 6 weeks; five studies (Reference Dougados, Braun and Szanto16–Reference Calin, Dijkmans and Emery18;Reference van der Heijde, Da Silva and Dougados22;Reference Barkham, Coates and Keen25) maintained treatment for 12 weeks, and two trials (Reference JC, Van Der Heijde and Braun20; Reference Gorman, Sack and Davis23) offered drug treatment for more than 12 weeks. Five trials (Reference Dougados, Braun and Szanto16;Reference Dougados, van der Heijde and Sieper17;Reference Pang, Wang and Suo19;Reference Lin, Lin and Gu21;Reference Huang, Zhang and Huang26) used a dosage of 50 mg administered once weekly to AS patients, whereas in other studies (Reference Calin, Dijkmans and Emery18;Reference JC, Van Der Heijde and Braun20;Reference van der Heijde, Da Silva and Dougados22–Reference Barkham, Coates and Keen25) etanercept was administered at a dosage of 25 mg twice-weekly. The methodological quality assessment is described in Table 2.
Table 2. Methodological Assessment of the RCTs Included in the Analysis (Jadad Score)

Efficacy
A greater number patients who received etanercept had a positive ASAS 20 response than those who received the placebo. There was an RR of 2.18 with a 95 percent CI of 1.78–2.67 for the 25 mg twice-weekly etanercept regimen without significant heterogeneity (I 2 = 0 percent; p = .80). For the 50 mg once-weekly regimen, the RR was 2.00 (95 percent CI, 1.70–2.37). The RR was 2.70 (95 percent CI, 2.09–3.49) when the drug was used for less than 12 weeks, versus 1.74 (95 percent CI, 1.37–2.22) for the 12-week treatment without heterogeneity. With a treatment duration of greater than 12 weeks, the RR was 2.56 (95 percent CI, 1.88–3.48).
The subgroup differences for ASAS 20 according to therapy duration showed that less than 12 weeks of treatment was more beneficial than treating for 12 weeks (p = .01, I2 = 83 percent). Moreover, dosing more than 12 weeks of etanercept was evaluated and found to be more effective than the 12 week duration (p = .06, I2 = 72.6 percent). The RR for the BASDAI 50 response was 2.20 (95 percent CI, 1.66–2.93) for 50 mg of etanercept administered once weekly, versus 3.41 (95 percent CI, 2.01–5.80) for 25 mg of etanercept administered twice-weekly with insignificant heterogeneity. The RR was 5.73 (95 percent CI, 1.85–17.72) when treatment lasted less than 12 weeks without heterogeneity, versus 1.95 (95 percent CI, 1.39, 2.72) for 12-week therapy without heterogeneity (Figure 2). The BASFI and BASDAI results are presented in Supplementary Table 2. The RR was more favorable for etanercept, although significant heterogeneity was observed among the trials.

Figure 2. Forest plots of etanercept efficacy compared with placebo evaluated by BASDAI 50 according to the duration of therapy.
Safety
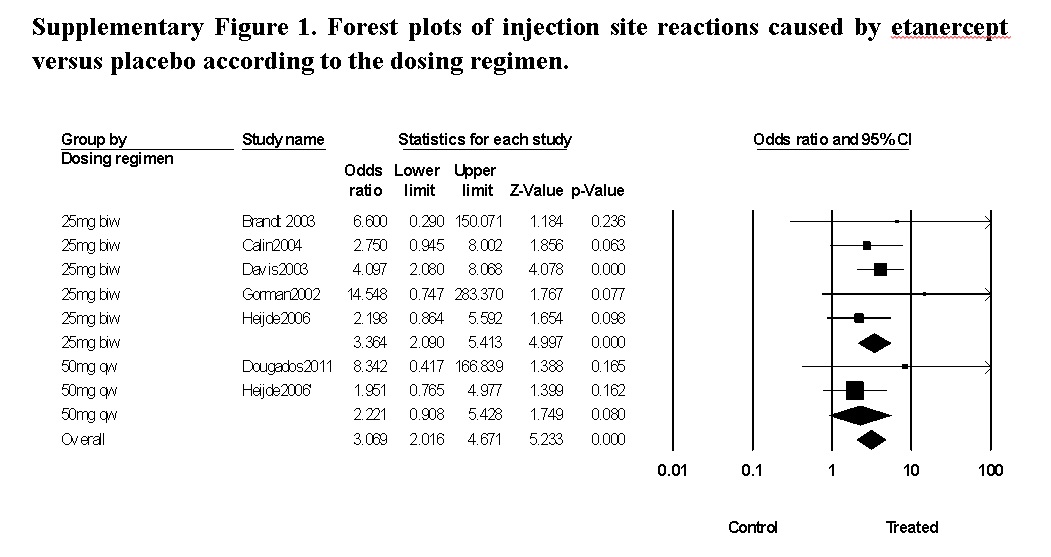
The only significant adverse reactions included were injection site reactions (Supplementary Table 3). The RR was 2.75 (95 percent CI, 1.84–4.09) for studies using the 25 mg twice-weekly treatment, versus 2.05 (95 percent CI, 0.95–4.43) for 50 mg administered once weekly. The use of etanercept was associated with a greater number of injection site reactions, as evidenced by an RR of 2.62 (95 percent CI, 1.84–3.71) without heterogeneity (Supplementary Figure 1). Other adverse reactions had insignificant disparities between the two dose groups that were consistent with the different dosing regimens and treatment durations (Supplementary Table 3).
Publication Bias
Publication bias was assessed using funnel plots and Egger's test. Asymmetric plots were observed in several responses such as ASAS 20 and BASDAI 50, suggesting a possible publication bias. However, with the small number of studies included in the analysis, it was possible that the statistical power was too low to distinguish real asymmetry; therefore, Egger's test was also used. In the present study, the analyzed ASAS 20 response outcomes showed a p-value = .03, while the p-value was 0.04 for BASDAI 50 response; p-values were calculated by Egger's test, and they indicated a publication bias. However, BASFI and injection site reaction results did not show a publication bias.
After the trim and fill procedure, we found that three studies were missing for each, and relevant changes in the overall pooled estimates (RRs) for each response outcome showed a publication bias. For the ASAS 20 response, the overall effect of the unadjusted RR was 2.07 (95 percent CI, 1.82–2.36) and the overall effect-adjusted RR was 1.99 (95 percent CI, 1.76–2.25). The outcomes of BASDAI 50 showed the unadjusted RR of the overall effect to be 2.43 (95 percent CI, 1.89–3.12), and the adjusted RR of the overall effect was 2.28 (95 percent CI, 1.79–2.91).
DISCUSSION
We conducted a meta-analysis to evaluate the safety and efficacy of etanercept to identify the most appropriate dose and duration of treatment in AS patients.
In the present study, no differences were observed between AS patients receiving etanercept 25 mg twice-weekly and those receiving 50 mg once-weekly. In addition, an etanercept dosing period of less than 12 weeks was more beneficial than other durations of therapy.
According to ASAS 20 responses, no differences were observed between 50 mg once-weekly and 25 mg twice-weekly dosing regimens, both of which demonstrated improvement of symptoms and physical limitations. BASDAI 50 outcomes indicated that the 25 mg twice-weekly etanercept regimen was more beneficial than the 50 mg once-weekly regimen in the present study. However, for the evaluation of AS symptoms, one group of international SpA experts currently recommends the use of ASAS 20 criteria to measure TNF blocker efficacy (Reference Sieper, Rudwaleit and Baraliakos10). AS disease activity is believed to be underdetermined by BASDAI (Reference Taylor and Harrison27). A previous analysis indicated etanercept 50 mg once-weekly dosing showed more effective for treating AS patients, but the study less focused on the outcome of etanercept thereby containing several other TNF-blockers during the indirect analysis (Reference Shu, Chen and Rong28). Moreover, a current systematic review evaluated the efficacy of etanercept treatment for AS patients using a different outcome measure, the ASAS 40 response, which also showed no discrepancies between these two dosing regimens (Reference Maxwell, Zochling and Boonen9).
Systematical evaluation of optimal durations for etanercept therapy to treat AS patients has been performed previously (Reference Baji, Pentek and Szanto8;Reference Machado, Baarbosa and Almeida29). However, these studies still had several limitations for analyzing data from the included trials. To provide more confident and specific outcomes, we categorized the treatment period into durations of less than 12 weeks, 12 weeks, and more than 12 weeks. We found that patients’ symptoms relatively improved with a treatment duration of less than 12 weeks. According to the ASAS 20 outcomes, we could not say significant efficacy differences existed between the less than 12 weeks and more than 12 weeks treatment duration groups. However, subgroup differences in the ASAS 20 responses demonstrated that etanercept treatment for less than 12 weeks showed benefit than treatment for exactly 12 weeks. This evaluation was confirmed by the BASDAI 50 response.
On the other hand, we could not demonstrate that dosing etanercept for more than 12 weeks was more beneficial than treatment for exactly 12 weeks, since this pooled ASAS 20 result could not be supported by another outcome such as BASDAI 50. Furthermore, a recent review reported that the ASAS 20 responses were not different between two durations of etanercept therapy, 12 and 24 weeks (Reference Baji, Pentek and Szanto8). As such, we can only suggest that AS patients should be treated with etanercept for less than 12 weeks.
However, some of these response measures evaluated were patient self-administered questionnaires, which may not correlate well with external indicators of disease activity (Reference Taylor and Harrison27). Questionnaire responses at the beginning of the treatment were usually more optimistic than later on, when patients had adjusted to the new health status. Considering the range of CIs in the present study for etanercept treatment duration of less than 12 weeks and the limitations of patient self-administered questionnaires, clinician decisions for etanercept therapy duration should be valuably considered, even though the analytic data showed that AS patients received the most benefit from less than 12 weeks of treatment.
According to the trial of Brandt et al. (Reference Brandt, Listing and Haibel30), the most efficacious end-points were reached at week 6, and were then maintained for 54 weeks after starting to dose etanercept for AS patients, and they therefore suggested that dosing etanercept at regular intervals with periodic interruptions should be used d for treating AS patients. The cyclic discontinuation of etanercept could also reduce the economic burden on AS patients (Reference Brandt, Listing and Haibel30), and prevent them from producing auto-antibodies (Reference Wallis, Haroon, Ayearst, Carty and Inman31). However, the outcome of the present analysis indicates that more supporting evidence is needed before suggesting that discontinuing etanercept therapy in AS patients might have an effect on response and/or remission after short-term treatment. Primary data corrected from RCTs or patient registries would be helpful in finding clear evidence in the future. BASFI and BASDAI scores were also consistent with the results of prior meta-analyses (Reference Li, Zhang, Wang and Shi7;Reference Maxwell, Zochling and Boonen9;Reference Machado, Baarbosa and Almeida29).
The most frequent adverse reactions reported in previous studies were headaches, upper respiratory infections, and injection site reactions (Reference Navarro-Sarabia, Fernandez-Sueiro and Torre-Alonso2). Although the incidence was not significant, serious adverse events were reported (Reference Machado, Baarbosa and Almeida29). According to the present analysis, the incidence of injection site reactions was significantly higher in the treatment group than the placebo group. In the subgroup analysis, injection site reactions were more common with the 25 mg twice-weekly dosing regimen. Other adverse reactions were not significantly different between the treatment and placebo groups.
In this study, we specified inclusion criteria for AS patients, dividing them into radiographic axial SpA and non-radiographic SpA (nr-axSpA) categories because of a recent attempt to diagnose AS according to the disease stage. However, there still have been many controversial efforts to clearly separate the stages of the disease (Reference Wallis, Haroon, Ayearst, Carty and Inman31). In addition, one study (Reference Dougados, van der Heijde and Sieper17) included in the present study included nr-axSpA patients showing a BASDAI score of 4 or more, which means these types of patients were good candidates to receive biological therapy. However, this study did not significantly influence the conclusion of our meta-analysis.
Conclusively, the present study showed it is more beneficial to use etanercept for less than 12 weeks, and two dosing regimens, 50 mg once-weekly and 25 mg twice-weekly, were equally effective for treating AS patients. However, if the patients present significant injection site reactions, we recommended 50 mg once-weekly dosing because that may require desensitization (Reference Bavbek, Ataman, Bankova and Castells32)
There were several limitations to this study. It did not differentiate results according to ethnic groups. A prior meta-analysis analyzed the efficacy of etanercept in AS patients according to ethnicity (Reference Li, Zhang, Wang and Shi7). However, studies included in that meta-analysis did not provide efficacy results according to race, and the analysis showed discrepancies in the number of patients in the trial groups compared with the original articles. The recommendations of international SpA experts for the measurement of TNF blocker efficacy have changed over time, leading to difficulty regarding the direct comparison of results among studies (Reference Sieper, Rudwaleit and Baraliakos10).
To evaluate the efficacy of etanercept treatment in AS patients, this analysis compared multifocal indexes. Studies included for this analysis used somewhat different outcome measures, so the models used in the present study may not provide fully comparable results. However, during the meta-analysis procedure, parts of outcome measures from an included study could be extracted and merged for pooling estimates (Reference Moore33). In the present study, included studies also provided outcomes of interests such as ASAS 20, and BASDAI 50. This study was the first meta-analysis to evaluate the efficacy and safety of etanercept in AS patients according to the dosing regimen and duration of therapy, using the most updated RCTs.
CONCLUSIONS
This meta-analysis analyzed the safety and efficacy of etanercept for the treatment of AS including recently published data. There was no significant efficacy difference between 50 mg once-weekly and 25 mg twice-weekly dosages, and etanercept dosing of a shorter duration than 12 weeks was more beneficial for AS patients. The safety of etanercept did not significantly differ between the dosing regimens, with the exclusion of injection site reactions.
SUPPLEMENTARY MATERIAL
Supplementary Table 1: https://doi.org/10.1017/S0266462317000150
Supplementary Table 2: https://doi.org/10.1017/S0266462317000150
Supplementary Table 3: https://doi.org/10.1017/S0266462317000150
Supplementary Figure 1: https://doi.org/10.1017/S0266462317000150
CONFLICTS OF INTEREST
The authors declare no conflict of interest.