



Health technology assessment (HTA) is a multidisciplinary process to determine the value of a health technology to inform healthcare resource allocation and decision making (Reference O’Rourke, Oortwijn and Schuller1). The HTA process uses explicit methods to evaluate a health technology including its social, economic, equity, and ethical impact and properties (Reference O’Rourke, Oortwijn and Schuller1). HTA has increasingly been adopted across various countries to support evidence-informed decisions for sustainable Universal Health Coverage (UHC). However, achieving sustainable and evidence-informed UHC poses a challenge for resource-and capacity-constrained low- and middle-income countries (LMICs) (Reference Sibbald, Singer, Upshur and Martin2). To support LMICs in their evolution to UHC and self-reliance, the US Agency for International Development (USAID) commissioned the Management Sciences for Health (MSH)-led Medicines, Technologies, and Pharmaceutical Services (MTaPS) program to develop a policy and guidance document on HTA institutionalization in LMICs, “A Roadmap for Systematic Priority Setting and Health Technology Assessment (HTA): A Practical Guide for Policy Action in Low- and Middle-Income Countries” (referred henceforth as the HTA Roadmap) was published in October of 2020. Leveraging from preliminary work conducted to inform such a Roadmap, this paper presents the findings from selected countries from an extensive literature review and emerging information complemented with further discussions with HTA practitioners in Asia.
Although the first HTA agency in Asia was established in Malaysia in 1995, its broader use within the region has gained significant momentum only in recent years (Reference Liu, Wu and Ahn3). The objective of this paper is to provide information about the progress of HTA within the region using a single “snapshot” via a Balanced Scorecard (BSC) in order to cross compare HTA institutionalization and share lessons learned with other LMICs to support their interests of advancing the use of HTA in their own settings.
Methodology
A systematic literature review was conducted to develop the HTA Roadmap commissioned by USAID and included articles published until April 2020 (Reference Castro, Kumar and Suharlim4). One of the key papers retrieved from this literature review, published by Chootipongchaivat et al., depicted “factors conducive to the development of HTA in Asia” (Reference Chootipongchaivat, Tritasavit, Luz, Teerawattananon and Tantivess5). Chootipongchaivat et al. (Reference Chootipongchaivat, Tritasavit, Luz, Teerawattananon and Tantivess5) expanded previous research by the World Health Organization’s (WHO) Asia Pacific Observatory on Health Systems to identify eighteen milestones (factors) considered as important for HTA institutionalization. The milestones were identified and ranked by the original authors based on a survey with HTA experts from seven Asian countries. The list of milestones is provided in Table 1.
Table 1. Milestones of National HTA Systems

HTA, health technology assessment.
The milestones listed in Table 1 were used in this paper to create a BSC to assess the progress of HTA in nine Asian countries at different stages of use of HTA. The authors scored the progress against each of the milestones made by HTA programs in China, India, Indonesia, Malaysia, Philippines, South Korea, Taiwan, Thailand, and Vietnam. Countries were selected to gather insights into the progress of HTA in LMICs in the region. Some of these countries (China, Indonesia, Malaysia, Thailand, South Korea, and Vietnam) were studied in the paper by Chootipongchaivat et al. and were included in this study for further research. India, Philippines, and Taiwan were included for additional evidence and comparison of the HTA progression within LMICs from the region. South Korea was selected as a benchmark. The progress of HTA was measured using the following scoring system on a scale of 1–5:
• 1—No progress on milestone, milestone not initiated, or limited information,
• 2—Milestone at early stages or ad hoc use of HTA,
• 3—Progress in achieving milestone for ongoing use of HTA but impact on decision making is variable/unclear,
• 4—Significant progress on milestone and high-quality ongoing use of HTA but limited remit in terms of type of decisions informed by HTA, and
• 5—Significant progress on milestone and high-quality ongoing use HTA that has a close connection to decision making and broad remit.
Countries could score a maximum of ninety points if they achieve a score of 5 on each milestone. The total score of each country will provide an indication on the advancement of HTA within each country allowing cross comparison. However, the score against each milestone is important for understanding areas in which the country may need to make additional efforts to develop its HTA program.
An update to the initial literature review conducted for the HTA roadmap document a year prior was conducted to expand the information for the scorecard. The updated literature review identified additional publications published from 15 Apr to 15 Sept 2020. In addition, key informant interviews were conducted with three regional HTA experts to fill information gaps from the literature review. Experts included leaders from HTA agencies/programs in China, Indonesia, and Taiwan. The experts interviewed were members of regional HTA networks such as the International Society for Pharmacoeconomics and Outcomes Research (ISPOR) and able to provide regional insights. One-hour interviews were conducted in English in September 2020 via conference calls.
Results
Malaysia was the first country in the region to establish an HTA program in 1995—the Malaysian Health Technology Assessment Section (MAHTAS) (Reference Liu, Wu and Ahn3). A decade later, countries like South Korea (2006) and Thailand (2007) also established HTA programs (Reference Liu, Wu and Ahn3). Other countries within the region, such as India (2019), Indonesia (2014), Philippines (2019), and Vietnam (2013) recently introduced HTA programs (Reference Liu, Wu and Ahn3;Reference Castro, Kumar and Suharlim4). Several factors have contributed to its growing use in the region. Multiple global and regional entities have made efforts to increase awareness of HTA. ISPOR has a regional chapter and has promoted the use of pharmaco-economics (Reference Liu, Wu and Ahn3). The International Decision Support Initiative (iDSI), WHO, Unicef, and UNDP are other stakeholders engaged in HTA support for countries in the region (Reference Castro, Kumar and Suharlim4). HTAsiaLink, the regional network for HTA agencies established in 2011, has facilitated regional collaboration and capacity building for HTA in the region (Reference Castro, Kumar and Suharlim4). The World Health Assembly (WHA) resolution WHA67.23 recommending the use of HTA for efficient resource allocation and UHC passed in 2014, catalyzing many countries to introduce HTA (Reference Castro, Kumar and Suharlim4).
Balanced Scorecard
Scores were assigned to each country based on findings from the literature review and results from the interviews with key informants. Of a total score of 90, South Korea had the highest score of 73 closely followed by a pioneer LMIC in this field, Thailand with 71 points, while Vietnam had the lowest at 28.5. All the countries studied have initiated HTA, with Malaysia, South Korea, Taiwan, and Thailand having the most advanced programs within the region. All countries except for China have national HTA method guidelines. All countries provide broad guidance on the HTA process and the types of decisions it informs. Benefits coverage and reimbursement decisions are the most common applications and starting points for HTA. Advanced HTA programs in Malaysia, South Korea, Taiwan, and Thailand inform a broad array of policy decisions, including clinical practice guidelines, pricing for health technologies, managed entry agreements, and evaluation of medical interventions or procedures. Table 2 provides a summary of the scores for each milestone for easy comparison among the countries included in the analysis.
Table 2. Progress and Characteristics of HTA in Selected Asian Countries
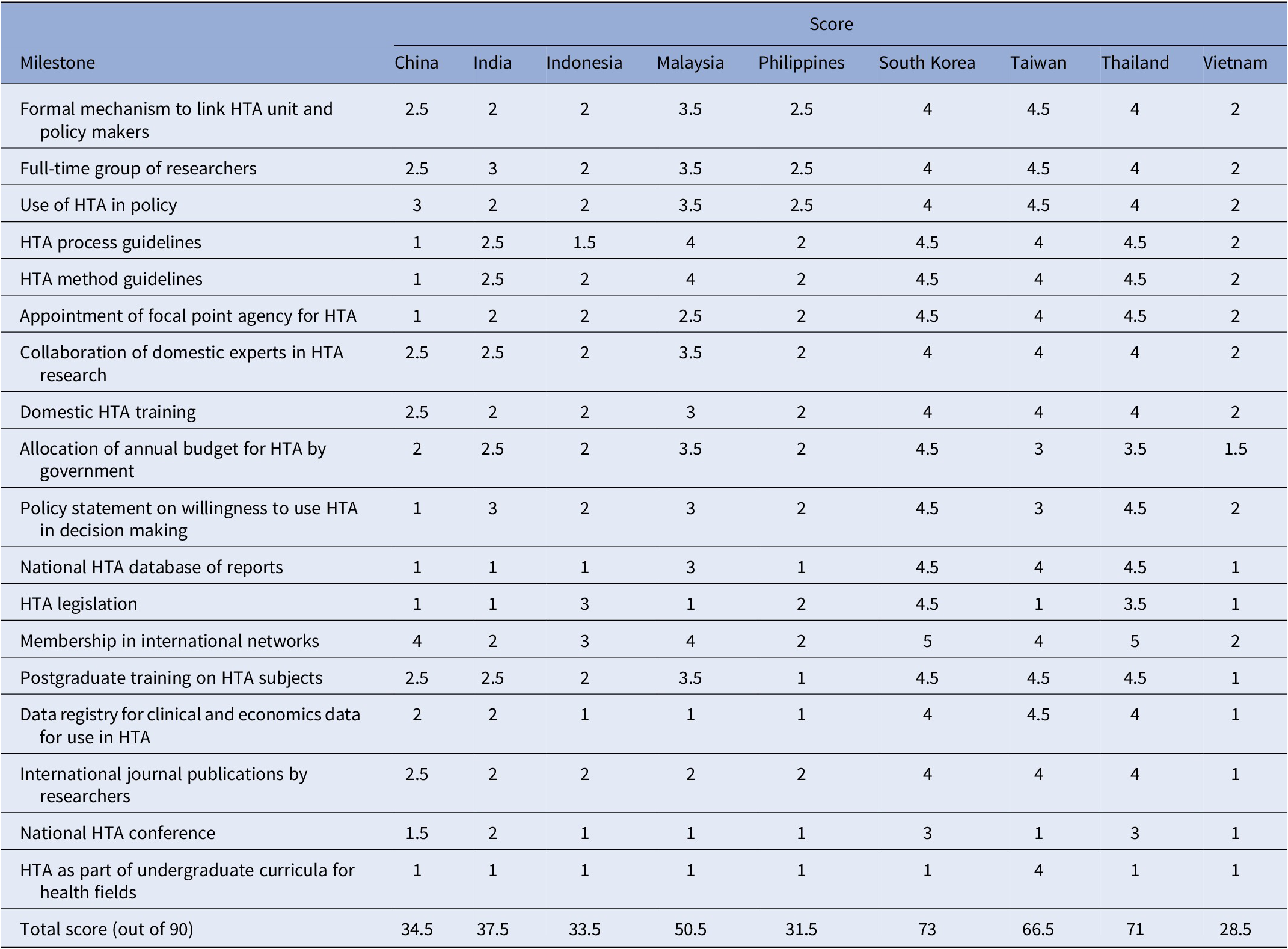
HTA, health technology assessment.
Country summaries (in alphabetical order)
China
Foundations for HTA were laid in the 1980s in China, while between 1993 and 2000, several HTA programs were established across universities in the country (Reference Wang, Jin and Bai6). Programs have been established at additional universities, governmental institutions, consulting companies, and industry-based organizations more recently (Reference Chen, He, Chi, Wei and Shi7). The National HTA Forum by the China National Health Development Research Center (CNHDRC) established the China Health Policy and Technology Assessment network in 2016 to further increase the capacity of HTA in the country and promote its use for policy making (Reference Wang, Jin and Bai6). The growth in HTA research and use for policy making has also been spurred by increased demand and favorable outlook toward HTA by the government (Reference Chen8). The National Health and Family Planning Commission (NHFPC) has issued guidelines to incorporate HTA in decision-making processes, such as price negotiations (Reference Chen, He, Chi, Wei and Shi7). The Ministry of Human Resources and Social Security (MHRSS) also increased the use of HTA principles by incorporating a value-based approach in updating the National Reimbursement Drug List (NDRL) (Reference Chen, He, Chi, Wei and Shi7). There is no national-level institution for HTA that informs broader policy making; use of HTA remains fragmented and limited to pharmaceutical products so far (Reference Chen, He, Chi, Wei and Shi7;Reference Chen8). Low levels of awareness among policy makers, need for additional HTA experts in the country, and lack of real-world local data also hinder HTA advancement in the country (Reference Chen, He, Chi, Wei and Shi7).
India
India has only recently established a national HTA agency—HTAIn (HTA in India) in 2019 (9). With the launch of Ayushman Bharat-Pradhan Mantri Jan Aayog Yojana, the Government of India’s UHC scheme in 2018, the government recognized the role for HTA to inform healthcare policy (9). Within a short span, HTAIn has set up a framework and stakeholder groups for conducting HTA in India. The agency is governed by its board, chaired by a member of the government’s planning institution, Niti Aayog (9). The board provides approval on the appraisal recommendations provided by a Technical Appraisal Committee that reviews the HTA studies’ outcomes (9). HTA studies are conducted by a network of academic institutes or technical partners (9). The overall process for HTA is managed and coordinated by a secretariat that also leads topic prioritization (9). Key challenges facing HTA in India include need for additional capacity and experts of HTA, evidence-based topic prioritization, long term financing, and limited availability of local data (9;Reference Smith10).
Indonesia
The Ministry of Health (MOH) established the Indonesian Health Technology Assessment Committee (InaHTAC) based on a Presidential regulation (2013) and subsequent (2016) Minister of Health Decree promoting use of HTA (Reference Sharma, Teerawattananon and Luz11;Reference Gleed12). InaHTAC is responsible for providing health policy recommendations to the Minister regarding which health technologies will be covered in the benefit package of the national health insurance program. The committee has completed and provided recommendations for twelve health technologies since 2014 and currently works with six Indonesian universities to continue to conduct assessments (Reference Sharma, Teerawattananon and Luz11;Reference Gleed12). InaHTAC is an independent committee with its secretariat within the MOH’s Center for Financing and Health Insurance (PPJK), which is responsible for health financing policy in the country (Reference Sharma, Teerawattananon and Luz11). HTAs have been conducted on topics selected by the PPJK and the National Health Insurance Agency (BPJS) (Reference Gleed12). However, a systematic topic selection process has yet to be established. Use of evidence and adoption of recommendations from HTAs conducted has been mixed. The appraisal and policy-making process in Indonesia is often ambiguous involving several institutions (Reference Gleed12;Reference Sudigdo13). Lack of adequate and trained HTA researchers, poor data quality, sustainable financing, and limited real-world data are additional challenges (Reference Sudigdo13).
Malaysia
MAHTAS was established in 1995 under the MOH to help ensure that facilities use safe, effective, and cost-effective health technology. MAHTAS commissions full and mini-HTA reports, information briefs, and horizon scanning of emerging health technologies (14). MAHTAS receives topic suggestions for HTA from various institutions within the MOH structure and produces an assessment of interventions procedures, and treatments to support the development of evidence-based clinical practice guidelines. Malaysia’s HTA program has begun playing a more significant role in health technology policy formulation and decision making (Reference Roza, Junainah and Izzuna15). HTA is also a core component for listing drugs on the MOH Medicines Formulary (MOHMF) (Reference Roza, Junainah and Izzuna15). Cost-effectiveness evidence is currently not mandatory, but there is growing interest in incorporating it in the HTA process by policy makers (Reference Roza, Junainah and Izzuna15).
Philippines
Philippines recently set up an HTA unit—the Center for Review of Health Technologies (STEP) within the Department of Health (DOH) in early 2019 (16;17). Philippines Methods Guide explicitly states that HTA will inform funding and coverage decisions for the country’s UHC scheme, PhilHealth (17). While STEP was established in 2019, HTA has been previously used to inform coverage decisions for PhilHealth with support from international partners such as iDSI, WHO, and Unicef (17). This included HTAs to inform the national formulary, adoption of the HPV vaccine, and streamlining the benefits package for certain high-cost medicines for noncommunicable diseases (Z-Package) (17). However, significant capacity building is still required to increase the number of HTA experts and practitioners within the country. STEP’s HTA program is nascent, and the impact and scale of the program will have to be determined over time.
South Korea
South Korea’s use of HTA is one of the most advanced in the region. Rising health expenditures led to several policy measures over the past two decades, including the use of HTA to inform coverage of the positive list system (PLS). PLS is the list of drugs that are covered by the national health insurance scheme, and evidence from HTA is also used to inform price negotiations for the PLS. The government established the Health Insurance Review and Assessment Agency (HIRA) in 2006 as an independent agency to manage the National Health Insurance scheme including conducting HTA. In 2008, the government set up an independent HTA agency, the National Evidence Based Collaboration Agency (NECA). NECA’s work and mandate has grown significantly since then and includes HTA, horizon scanning, setting research priorities, health policy research, and clinical evidence generation. NECA also has a department focused on big data for health care to further strengthen evidence-based decision making for the country. Despite the advanced nature of HTA in the country, challenges remain, such as building up sufficient trained professional staff and creating awareness about HTA among key stakeholders.
Taiwan
Taiwan has a department for HTA within the Center for Drug Evaluation (CDE), an independent research agency of the Ministry of Health and Welfare (MOHW) (18). Taiwan introduced HTA in 2007 to support the National Health Insurance Agency (NHIA) and inform benefits management and reimbursement of drugs, devices, and medical procedures (Reference Kao, Huang and Gau19). Since then, it has expanded to inform decisions on health policy and social care (Reference Kao, Huang and Gau19). The 10-year review of the HTA program implementation in Taiwan found that HTA has had a significant impact on reimbursement and health policy decision making in the country while improving the quality of care (Reference Kao, Huang and Gau19). Taiwan has adopted the pragmatic approach to HTA with a rapid review process (Reference Huang20). An HTA report is submitted to NHIA in forty-two calendar days wherein the team summarizes reports from HTA agencies in other high-income countries, including NICE (UK), CADTH (Canada), and PBAC (Australia) (Reference Huang20). The health economists in the HTA department also conduct the budget impact analysis using real-world data from the NHIA database (Reference Huang20). Key challenges to the HTA department include human resource capacity and financial sustainability of the program (Reference Huang20).
Thailand
HTA has existed in Thailand to a varying degree since the 1990s and plays a critical role in the country’s healthcare policy (Reference Dittrich and Asirifi21). The national HTA agency, Health Intervention and Technology Assessment Program (HITAP), was established in 2008 (Reference Dittrich and Asirifi21). The Subcommittee for the Development of the Benefit Package and Service Delivery (SCBP) realized the need for an explicit and evidence-based mechanism to inform coverage decisions (Reference Dittrich and Asirifi21). HITAP and the International Health Policy Program, the government’s leading health research think tank, were designated as the lead agencies for conducting HTA and policy research to support the SCBP (Reference Dittrich and Asirifi21). The remit of HITAP has expanded over the years to conduct HTAs for updating the National Essential List of Medicines, informing pricing decisions, and providing decision-support research on other programs and services of the Ministry of Public Health (MoPH) (Reference Dittrich and Asirifi21). HITAP has a robust program with detailed process and methods guidelines for HTA (Reference Dittrich and Asirifi21). Its recommendations have significant influence on decisions made by the MoPH and its associated institutions (Reference Tanvejsilp, Taychakhoonavudh, Chaikledkaew and Ngorsuraches22;Reference Leelahavarong, Doungthipsirikul and Kumluang23). HITAP’s success has led to it becoming a regional capacity building resource for other countries in the region and globally (Reference Leelahavarong, Doungthipsirikul and Kumluang23). While HITAP is seen as a critical research and decision-support agency, it is still faced with the challenge of sustainable financing for its work (Reference Leelahavarong, Doungthipsirikul and Kumluang23). A significant portion of its funding comes from user institutions (e.g., units and programs within the MoPH) that commission HTAs, and this can vary from year to year. HTA process guidelines have been designed to promote transparency, but the complex health policy process in Thailand and multiple stakeholders make this challenging (Reference Tanvejsilp, Taychakhoonavudh, Chaikledkaew and Ngorsuraches22). The overlap among stakeholders engaged in both the assessment and appraisal processes has faced criticism (Reference Leelahavarong, Doungthipsirikul and Kumluang23). Additional capacity building to expand the cadre of HTA experts is needed to address the high demands for HTA in the country (Reference Leelahavarong, Doungthipsirikul and Kumluang23).
Vietnam
Vietnam is a recent entrant in the introduction of HTA, although, the HTA program came out of several initiatives of the government in previous years (24). With a focus on achieving sustainable UHC, the MOH started showing interest in HTA and established a framework for an HTA development plan in 2014 (24). With support from international partners such as iDSI, several HTA studies were conducted between 2014 and 2017 (24;25). The National Health Insurance Policy Consulting Committee created a task force dedicated to HTA in 2016, including leading the appraisal process of the initiated studies (25). Vietnam established its national HTA program in 2018 by appointing the Health Strategy and Policy Institute as the core agency for conducting HTA (25). However, the program is nascent and needs significant support for scale-up and building HTA capacity within the country (Reference Chen8). A sustainability plan also needs to be developed as initial momentum has been significantly supported by international partners.
Discussion
Based on our findings, we categorized the HTA programs across the various countries into three archetypes. The first includes countries with advanced HTA programs, such as Thailand and South Korea. These countries have independent HTA agencies with a broader remit, explicit process and methods guidelines, a full-time network of researchers, and routine use of HTA recommendations for policy making. The second type includes Taiwan and Malaysia with established HTA programs that have broad remits but may not use full economic evaluations for HTA. Finally, countries like China, India, Indonesia, Philippines, and Vietnam, have recently stepped up the use of HTA and have developed some supportive institutional structures or processes.
The increased use of HTA is driven by the goal of UHC and defining its scope of coverage. From established programs in countries like Thailand and South Korea to the more recent ones in China, India, Indonesia, and so on, HTA advancement was rooted in building sustainable UHC programs and supporting benefits package design. For other LMICs considering HTA as a policy and decision support tool, benefits package design or updating national essential medicines lists are good starting points for applying HTA.
A formal process or mechanism for linking HTA with policy making coupled with strong political commitment can lead to strong HTA programs. Thailand has institutionalized processes to integrate HTA into coverage decision making and has one of the strongest programs in the region. China may not have a national HTA program, but HTA informs formulary decisions. Malaysia has legislation supporting HTA, but its use and remit is not as extensive as in South Korea or Thailand. Indonesia also has national legislation but lacks a clear process to link HTA with policy making, thereby limiting its impact. Thus, this could be an important lesson for nascent programs in other LMICs—while regulations or legislations supporting HTA are helpful, political will is key.
Financial sustainability of HTA programs is a challenge for most countries. South Korea has the only program with dedicated financial investment by the government. It is a crucial factor in its quick expansion and comprehensive remit. Thailand and Taiwan have strong HTA programs driven by demand, but secure long-term financing is lacking. If economic conditions or politics will change, users may not commission HTAs, creating sustainability challenges. Countries launching HTA programs, such as India, Indonesia, Philippines, and Vietnam, need to learn from these experiences and integrate financial sustainability models in their expansion plans.
Research from across the countries revealed that awareness about HTA and its applications is still needed. HITAP’s efforts in raising awareness about HTA in Thailand has generated significant demand for HTA and sustained the program for nearly two decades. The HTA agencies in the other countries could learn from Thailand success and similarly work to raise awareness, thus leading to greater engagement of patient populations, transparency in the policy-making process, and demand for HTA.
As observed in the findings, HTA capacity and infrastructure is a challenge for all HTA programs. Advanced programs like those in Malaysia, South Korea, Taiwan, and Thailand continue to need additional trained experts to meet demand while trying to retain those trained. China, India, and Indonesia have a strong network of academic institutions that will play an important role for their nascent HTA programs. However, graduate programs specializing in HTA will need to be created for long term sustainability. The Philippines and Vietnam face significant shortages of adequately trained personnel and will require additional investments to address the gaps.
Collaborative projects could help create resource hubs and shared infrastructure for increasing the number of HTA experts in the region. Regional collaboration and capacity building have yielded increased engagement in HTA in the region. Emerging programs have received support from Thailand, South Korea, and international agencies for training on HTA methods, developing methodological and process guidelines, and guidance on institutional frameworks for HTA. Regional collaboration approaches like the European Network for Health Technology Assessment (EUnetHTA) could create effective peer-learning opportunities. LMICs could adapt Taiwan’s pragmatic approach to scale HTA in the short term by leveraging HTA results and recommendations from similar countries to inform their own evidence reviews. This can be helpful for countries early in their HTA evolution or interested in conducting rapid reviews. Having regional shared evidence databases for country members to access could be another aspect of regional collaboration.
This research yielded limited literature and discussion within the region related to the monitoring and evaluation of HTA programs. However, it concurs with other authors on the need for assessing the impact of HTA-related activities, especially among LMICs. This is important for advancing HTA use and harnessing the best practices and lessons learned by countries in their own HTA evolution. The authors hope that this research provides a pragmatic analytical framework for assessing HTA programs robustness and progress to implementation. The BSC developed can be an effective comparative tool to assess the state and progression of HTA implementation, as well as to identify potential weaknesses in their HTA evolution, across other geographies beyond Asia.
Funding Statement
This document is partly made possible by the generous support of the American people through the US Agency for International Development (USAID) contract no. 7200AA18C00074. The contents are the responsibility of Management Sciences for Health and do not necessarily reflect the views of USAID or the United States Government.
Conflicts of Interest
The authors declare that they have no conflict of interest.


