The Centers for Disease Control and Prevention (CDC) recommends implementation of an antimicrobial stewardship (AS) program in all acute-care hospitals, nursing homes, and outpatient clinics. 1 – Reference Sanchez, Fleming-Dutra, Roberts and Hicks 3 Because smartphones are increasingly used to access clinical decision support,Reference Carey, Payne, Ahmed and Goodson 4 – Reference Payne, Weeks and Dunning 6 several experts have explored smartphones applications (apps) to disseminate antibiotic prescribing recommendations.Reference Goff, Jankowski and Tenover 7 – Reference Moodley, Mangino and Goff 10 As of 2012, more than 1,200 infectious diseases-focused apps were available, a number of which contain AS guidance on either a national or local level.Reference Parfitt, Valiquette and Laupland 9 , Reference Moodley, Mangino and Goff 10 While nationally focused AS apps tend to be more comprehensive, they do not account for local antibiotic resistance patterns and formularies. For these reasons, local AS-focused apps may be preferable.
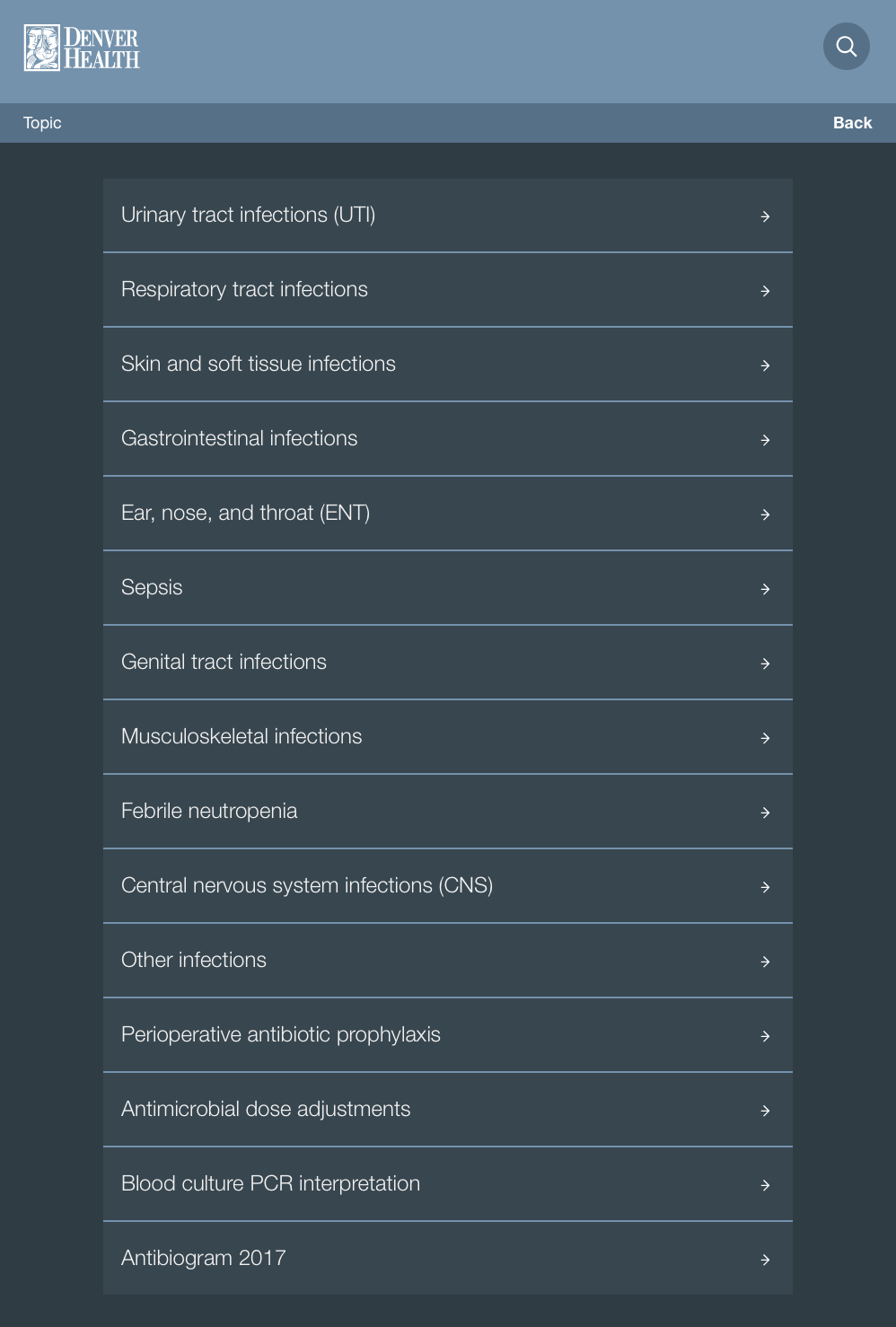
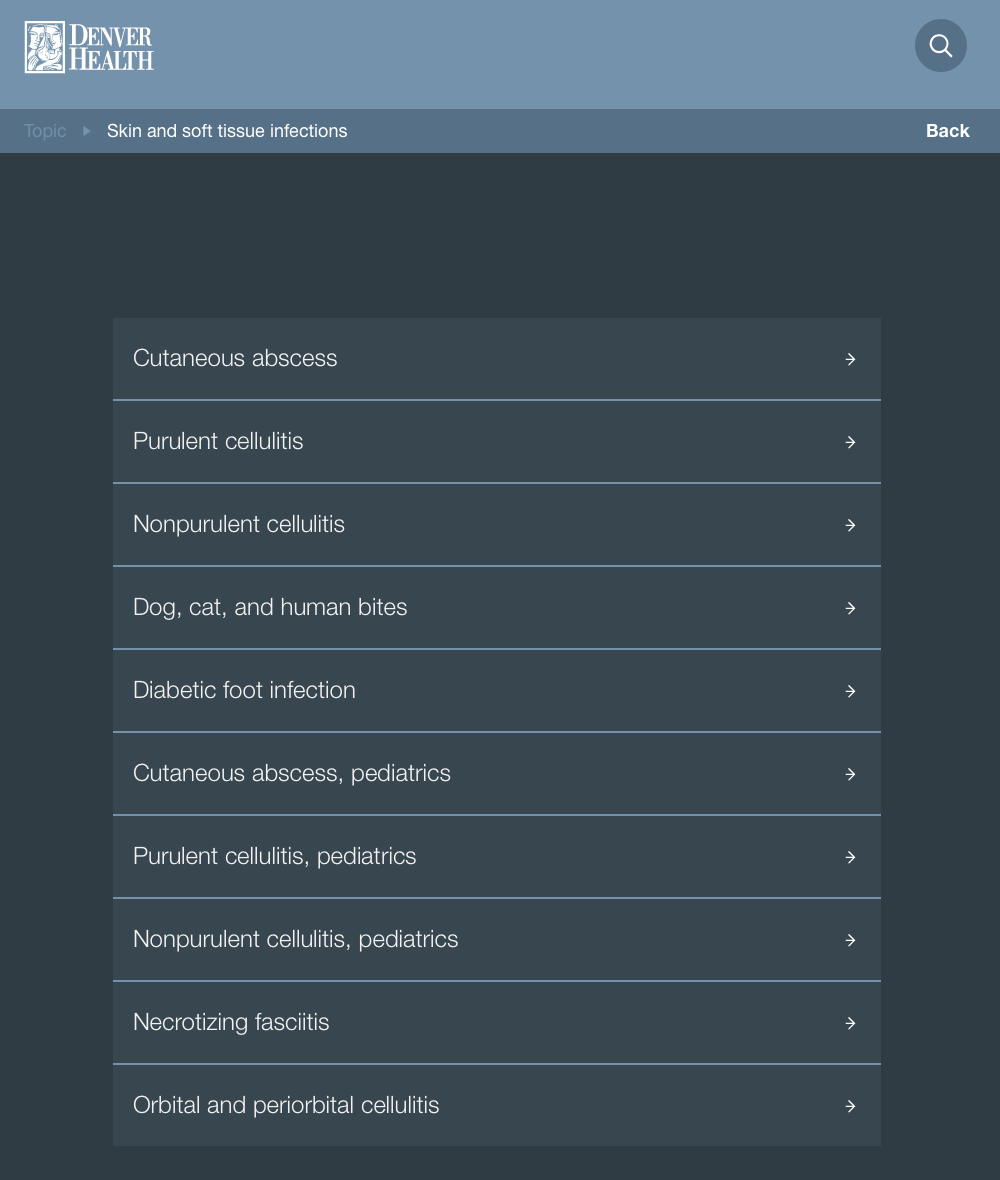
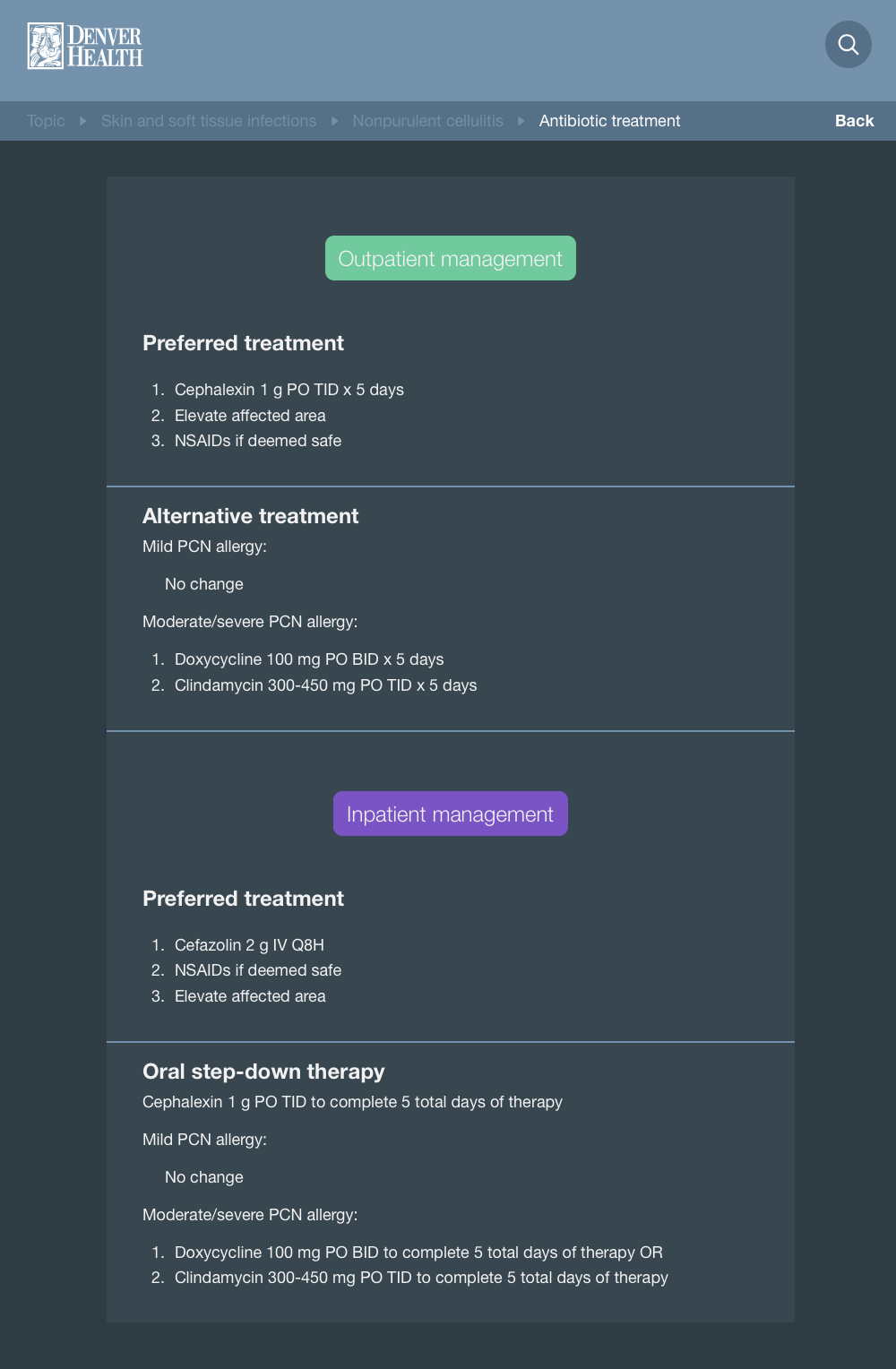
We developed and implemented an AS-focused app in August 2014; a second version was released in October 2016. The app contains local prescribing recommendations for >50 infections, perioperative antibiotic prophylaxis, antimicrobial dose adjustments based on renal function, and the annual antibiogram. The objective of this study was to determine patterns of app use over time and to explore the conditions for which providers most often seek prescribing resources.
Methods
Setting and Population
This cross-sectional observational study was conducted at Denver Health, an integrated healthcare system consisting of a 500-bed safety-net teaching hospital, an emergency department, 2 urgent care centers, 9 primary care clinics, and 17 school-based health centers.Reference Gabow, Eisert and Wright 11 In 2017, 477 physicians, 322 advanced practice providers, and 52 pharmacists were employed by Denver Health. Approximately 1,000 residents and 2,500 students rotate through the healthcare system annually.
App Development and Dissemination
The app is a mobile website that functions as a native application on smartphones and tablets; it can also be accessed by computer. The display is identical on all 3 types of devices (Supplement A). It is available via an open-access URL and is not marketed in app stores. The clinical providers on the AS team update and add content on a rolling basis.
The first app version was developed in 2014 by an emergency medicine resident (J.V.). It was disseminated to emergency medicine providers via e-mail and word of mouth. While the original intent was to provide empiric antibiotic recommendations for common infections treated in the emergency department, the content quickly expanded to include conditions encountered by inpatient and primary care providers, too. The app was then disseminated system-wide to hospitalists, surgeons, primary care providers, advanced practice providers, and pharmacists via (1) e-mail with instructions to obtain the app; (2) an advertisement at departmental meetings and teaching conferences; (3) instructions posted on the AS internal website; (4) a one-on-one tutorial in clinical settings; and (5) education in the required annual infection prevention and AS training module. Once providers accessed the URL, they were encouraged to select either “bookmark” or “add to homescreen” for easy future access. The first 2 implementation techniques were solely focused on marketing of the app, while the latter 3 were opportunistic, promoting the app through pre-existing AS or infection prevention connections.
While this app was anecdotally useful to providers, our information technology department could not support the app on its original platform. Therefore, we hired a software development company (Ingenious Softworks, Montevideo, Uruguay) to develop the app on a new platform. In October 2016, physicians, advanced practice providers, pharmacists, and residents affiliated with Denver Health were notified of the availability of the upgraded app via the same methods used in 2014. We began to track utilization in December 2016. The study period began on January 1, 2017 and ended December 31, 2017.
Data Collection and Definitions
Google Analytics was used to extract data regarding use of the antibiotic app.Reference Crutzen, Roosjen and Poelman 12 This technology identifies the IP address of a device that is accessing a particular website. It can characterize the number and type of unique devices, the number of sessions, the mean session duration, and the frequency that certain content was accessed. From these data, we analyzed antibiotic app utilization on both a monthly and aggregate basis.
“Sessions” were defined as the number of times a device engaged with the app. “Unique devices” were the number of devices used to access app content. To control for providers who accessed the app from multiple devices, we estimated the number of “unique users” as the number of unique smartphones per time period.
Statistics
Linear regression models were performed to assess how app usage changed over time. Regression was performed for all device types combined as well as stratified by device type (ie, smartphone, desktop, and tablet). To assess model fit, P values and adjusted R2 values were examined. All statistics were performed using SAS version 9.4 software (SAS Institute, Cary NC). This study is nonhuman subjects research because no identifying data were collected.
Results
The antibiotic app was accessed 23,734 times on 5,097 unique devices during the study period. The mean session duration was 2:22 minutes. Overall usage increased by ~94 unique devices per month (P<.001) (Figure 1). Usage increased significantly on smartphone (P<.001) and desktop devices (P<.001), but not on tablets (P=.14). Adequate model fit was observed for the overall (Adj R2=0.829) and device-specific models (adj R2 [smartphone]=0.679; adj R2 [desktop]=0.862) with the exception of the tablet-specific model (adj R2=0.127). While most unique devices were desktop computers (n=3151, 62.1%), most sessions were accessed from smartphones (n=18,860, 79.5%) (Table 1). Based on smartphone usage, we estimate that at least 1,887 unique users accessed the app in 2017.

Fig. 1 Sessions of content accessed and unique users accessing the antibiotic app per month.
Table 1 Antibiotic App Utilization Patterns

a Used to estimate the number of unique users of the antibiotic app.
The most frequently accessed content included treatment of urinary tract infections (UTIs) (336–688 sessions per month), respiratory tract infections (RTIs; 329–596 sessions per month), skin and soft-tissue infections (SSTIs; 289–615 sessions per month), gastrointestinal infections (108–195 sessions per month), and genital infections (52–153 sessions per month).
Discussion
Our institution-specific antibiotic app was utilized frequently in 2017, and its use grew over time. The increasing trend was seen for both smartphone and desktop devices, suggesting that compatibility with both types of technology is essential for the success of institutional apps. Moreover, UTI, RTI, and SSTI were the most commonly accessed topics on the antibiotic app. Not surprisingly, these are also the most common infections for which antibiotics are given in the hospital.Reference Braykov, Morgan and Schweizer 13 While some may say, “Old habits are hard to break,” we were pleasantly surprised that providers accessed prescribing guidance for common infectious conditions. This suggests that they are seeking new knowledge or double-checking that their prescribing habits are consistent with institutional guidance.
This study has several limitations. We were unable to track the type of provider that accesses data. We considered adding a login feature to the app but feared that this would be a barrier to use; the impact of a login on app use would be an interesting area of research in the future. Additionally, we are unable to determine whether providers follow the recommended antibiotic guidance after accessing the app. This would best be ascertained from a review of cases in the pre- and postantibiotic app periods. Finally, our estimate of the number of unique users is likely an underestimate because we used smartphone utilization as a surrogate, assuming that each person who accessed the app had accessed it at least once by smartphone. It is likely that some providers accessed the app from a desktop only.
In summary, the antibiotic app is widely and increasingly being used over time, suggesting that it is an effective tool to disseminate institution-specific antibiotic recommendations in our integrated health system. Additional work is needed to explore providers’ perceptions of the app and to determine whether its use has increased adherence to institutional prescribing guidance.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/ice.2018.135
Financial support
No financial support was provided relevant to this article.
Potential conflicts of interest
All authors report no conflicts of interest relevant to this article.