



Extended-spectrum β-lactamase (ESBL)–producing Escherichia coli and Klebsiella spp were highlighted in the most recent Centers for Disease Control and Prevention (CDC) Antibiotic Resistance Threats Report as a serious threat. They caused an estimated 197,400 infections and 9,100 deaths among hospitalized US patients in 2017. 1 In addition, ESBL-producing Enterobacterales (ESBL-E) are a global problem, with significant spread in Europe, Asia, Africa, the Middle East, Latin America, and North America. Reference Adler, Katz and Marchaim2,Reference Pitout and Laupland3 ESBLs are a subset of enzymes that confer resistance to a broad range of β-lactam antibiotics including penicillins, third-generation cephalosporins, and monobactams. ESBLs are inhibited by β-lactamase inhibitors such as clavulanate, sulbactam, and tazobactam. Reference Pitout and Laupland3 The most common ESBL producers are gram-negative organisms of the order Enterobacterales, and E. coli and Klebsiella spp account for most ESBL producers among the Enterobacterales. Reference Tamma, Smith and Adebayo4 ESBLs are highly heterogeneous, with >200 different ESBL enzymes, of which TEM, SHV, and CTX-M types are the most common. Reference Adler, Katz and Marchaim2 Most of these enzymes are located on mobile genetic elements, which allows ESBL genes to be transferred among different organisms. Reference Paterson and Bonomo5 Because ESBL-producing organisms often display a multidrug-resistant phenotype, few reliable treatment options Reference Harris, Tambyah and Lye6 are available other than carbapenems. Reference Adler, Katz and Marchaim2
The emergence of ESBL-producing organisms in the United States is largely driven by the dissemination of the CTX-M family of ESBL enzymes. Reference Adler, Katz and Marchaim2,Reference Tamma, Smith and Adebayo4,Reference Chen, Freeman and Nicholson7 Previously published reports indicated that ESBL-E rates have been increasing in some areas Reference Freeman, Sexton and Anderson8 ; however, the data on ESBL-E burden are mostly limited to regional studies or studies in hospitalized patients, 1,Reference Jernigan, Hatfield and Wolford9,Reference McDanel, Schweizer and Crabb10 which highlights the need for acquiring population-based ESBL-E surveillance data across the United States.
We conducted a surveillance pilot program through the Emerging Infections Program Healthcare-Associated Infections-Community Interface (EIP HAIC) Multisite Gram-Negative Surveillance Initiative (MuGSI) Reference Magill, Dumyati, Ray and Fridkin11 to describe the epidemiology of ESBL-E and to refine methods for ongoing surveillance.
Methods
From October through December 2017, we conducted a pilot program of active, laboratory-based surveillance in selected counties at 5 EIP sites. Population-based surveillance was conducted in 2017 at 3 sites in selected counties with a total population of 1,578,127: New Mexico (Bernalillo County; population, 676,773), New York (Monroe County; population, 747,642), and Tennessee (Maury, Lewis, Wayne, and Marshall Counties; total population, 153,712). However, 2 sites did not enroll all clinical laboratories in their catchment areas because of limitations with feasibility for the pilot program; therefore, these sites conducted sentinel surveillance in selected laboratories in specific counties: Georgia (Clayton County), and Colorado (Boulder County).
An incident ESBL-E case was defined as the first isolation of E. coli, K. pneumoniae, or K. oxytoca resistant to at least 1 extended-spectrum cephalosporin (ceftazidime, cefotaxime or ceftriaxone) and nonresistant (ie, susceptible or intermediate) to all tested carbapenems from urine or a normally sterile body site in a resident of the surveillance catchment area during a 30-day period. Respiratory specimens were not included for this surveillance pilot.
To identify cases, site staff obtained lists of E. coli, K. pneumoniae, and K. oxytoca isolates that met the case definition phenotype from participating laboratories through queries of the Laboratory Information Systems (LIS) or the Automated Testing Instruments (ATIs) with preference for obtaining data from the ATI. Site staff reviewed medical records and completed case report forms (CRFs) for all incident ESBL-E cases including information on patient demographics, location of culture collection, healthcare exposures, types of infection associated with culture, underlying conditions, patient outcomes, and selected other risk factors. Site staff conducted queries of state vital records to determine mortality within 30 days of incident culture collection.
We categorized ESBL-E cases as healthcare-associated if the incident culture was collected either (1) >3 calendar days after admission to a hospital or (2) at an outpatient visit or during the first 3 days of a hospitalization from a patient with a history of hospitalization, surgery, residence in a long-term care facility (LTCF) or residence in long-term acute-care hospital (LTACH) in the year prior to culture, or from a patient on chronic dialysis or with an indwelling device or external urinary catheter in the 2 days prior to culture collection. If none of these risk factors was identified, we categorized the case as community-associated. Healthcare-associated cases were categorized as hospital onset (HO), LTCF onset, or LTACH onset if the patient was located in one of these facility types >3 calendar days before the date of incident culture. A case was considered healthcare-associated community-onset (HACO) if the patient was located at other facility types (eg, assisted living facility) or at a private residence and had 1 or more of the healthcare exposures listed above.
A convenience sample of isolates from incident cases was submitted to the CDC for confirmatory testing and molecular characterization. At the CDC, isolates underwent species identification using matrix-assisted laser desorption/ionization-time of flight (MALDI-TOF) mass spectrometry using a Biotyper 3.1 system (Bruker Daltonics, Billerica, MA). Isolates also underwent reference antimicrobial susceptibility testing using broth microdilution and phenotypic screening for ESBL production using ceftazidime and cefotaxime alone and in combination with clavulanate. 12 Whole-genome sequencing analysis of isolates was performed using Illumina MiSeq (Illumina, San Diego, CA). Sequences were screened for the presence of acquired β-lactamase genes (including ESBL genes) using ResFinder and ArgAnnot databases. Reference Zankari, Hasman and Cosentino13,Reference Gupta, Padmanabhan and Diene14 Sequence types (STs) were determined using multilocus sequence type (MLST) schemes available from pubMLST and Institute Pasteur. Reference Jaureguy, Landraud and Passet15,Reference Diancourt, Passet, Verhoef, Grimont and Brisse16 We used the Achtmann multi-locus sequence type (MLST) scheme Reference Wirth, Falush and Lan17 from Enterobase Reference Zhou, Alikhan, Mohamed, Fan and Achtman18 to identify E. coli sequence types (STs), and the Pasteur MLST scheme (http://bigsdb.pasteur.fr/) Reference Diancourt, Passet, Verhoef, Grimont and Brisse16 for Klebsiella spp.
Surveillance data were collected and managed using Research Electronic Data Capture (REDCap) Reference Harris, Taylor, Thielke, Payne, Gonzalez and Conde19 hosted at the CDC. REDCap is a secure, web-based software platform designed to support data capture for research studies. The data were finalized in March 2019. We analyzed data using SAS version 9.4 software (SAS Institute, Cary, NC). Because surveillance was conducted during a 3-month period, we estimated the crude annual incidence rates per 100,000 population for the 3 EIP sites conducting population-based surveillance as the number of cases multiplied by 4 divided by population based on the 2017 US Census. 20 We performed descriptive analyses of cases with completed CRFs.
This activity was reviewed by the human subjects research advisors in the CDC National Center for Emerging and Zoonotic Infectious Diseases and was determined to constitute a nonresearch public health surveillance activity. Therefore, review by the CDC Institutional Review Board (IRB) was not required. The project also underwent review in each of the participating EIP sites and was either approved by the IRB with a waiver of informed consent or was considered a nonresearch public health activity.
Results
We identified 884 ESBL-E incident cases among 815 patients (Table 1). Of the 884 cases, 790 (89%) were E. coli bacteremia and 94 (11%) were Klebsiella spp bacteremia. The estimated annual incidence rate per 100,000 population was 199.7 overall in the 3 population-based sites. Site-specific incidence rates were 182.6 per 100,000 population in New Mexico, 173.9 per 100,000 population in New York, and 400.7 per 100,000 population in Tennessee. The estimated annual incidence rate among females (303.4 per 100,000 population) was 3.9 times the rate among males (78.6 per 100,000 population) (Table 2). The estimated annual incidence rate increased with age from 107.8 per 100,000 population among persons aged 19–49 years to 1,098.7 per 100,000 population among persons aged ≥80 years.
Table 1. Number of Incident Extended-Spectrum β-Lactamase–Producing Enterobacterales Cases and Estimated Annual Incidence Rate per 100,000 Population, by Organism, 5 Emerging Infections Program sites, United States, 2017 (N=884)

Note. EIP, CDC Emerging Infections Program.
a Klebsiella pneumoniae, Klebsiella oxytoca.
b Because surveillance in Colorado and Georgia was not population based, incidence is not provided.
Table 2. Number of Incident Extended-Spectrum β-Lactamase–Producing Enterobacterales Cases and Crude Incidence Rate per 100,000 Population, by Demographic Characteristics, 3 Emerging Infections Program sites, United States, 2017 (N=788)
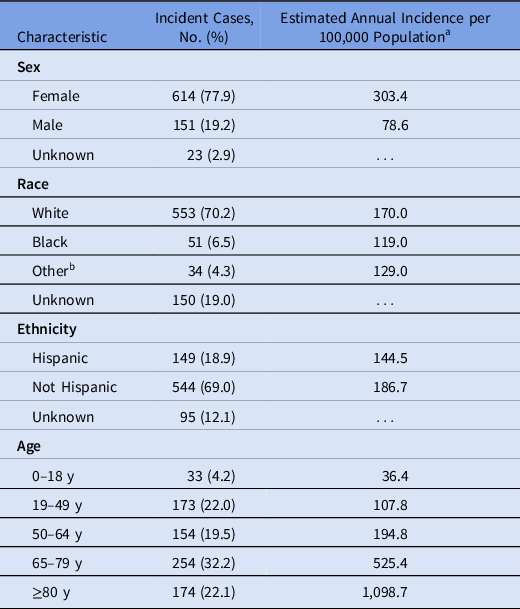
a Incidence estimate for sites conducting population-based surveillance (New Mexico, New York, Tennessee). Because surveillance in Colorado and Georgia was not population based, incidence is not provided.
b Asian, American Indian or Alaska Native, Native Hawaiian or other Pacific Islander.
Characteristics of incident ESBL-E cases with complete CRFs (n = 837, 94%) are presented in Table 3. Almost all ESBL-E cases were identified from either urine (n = 800, 96%) or blood (n = 30, 4%). The most documented infection types or syndromes associated with incident cultures were urinary tract infection (UTI; n = 696, 83%) and bacteremia or sepsis (n = 55; 7%). Among ESBL-E cases, 393 (47%) were classified epidemiologically as community-associated, 282 (34%) were HACO, and 40 (5%) were HO. The most frequently reported healthcare exposures among HACO ESBL-E cases in the year before incident culture were acute care hospitalization (n = 209, 74%), surgery (n = 111, 39%), and the presence of a urinary catheter in the 2 days before culture collection (n = 72, 26%). Also, 247 cases (30%) were hospitalized at the time of or within 30 days after initial culture collection. Within 30 days of positive culture collection, 22 cases (3%) died.
Table 3. Characteristics of Incident Extended-Spectrum β-Lactamase–Producing Enterobacterales Cases With Complete Case Report Forms by Species, 5 Emerging Infections Program sites, United States, 2017 (N=837)

Note. LTCF, long-term care facility; LTACH, long-term acute care hospital; HACO, healthcare-associated community-onset.
a Klebsiella pneumoniae, Klebsiella oxytoca.
b Peritoneal fluid, bone, deep tissue, vitreous humor.
c Clinic/doctors’ office, surgery, dialysis center, other outpatient clinics.
d Surgical site infection, decubitus/pressure ulcer, peritonitis, appendicitis, atrioventricular fistula/graft infection, cholangitis, chronic ulcer/wound, osteomyelitis, prostatitis.
e Homeless, left against medical advice, living in a shelter.
Clinical characteristics and risk factors are presented in Table 4. Most ESBL-E cases (76%) occurred in patients with underlying medical conditions. Antibiotic use within 30 days before culture was reported for 315 (38%) ESBL-E cases overall, including 102 (26%) of 393 community-associated cases. The most frequently used antibiotics were intravenous cephalosporins (n = 83, 10%), fluoroquinolones (n = 68, 8%), β-lactam combination agents (n = 64, 8%), trimethoprim-containing antibiotics (n = 51, 6%), and nitrofurantoin (n = 45, 5%).
Table 4. Clinical Characteristics, and Risk Factors Among Incident Extended-Spectrum β-Lactamase–Producing Enterobacterales Cases With Complete Case Report Forms, 5 Emerging Infections Program Sites, by Epidemiologic Class, United States, 2017 (N=837)

Note. IQR, interquartile ratio.
a Epidemiologic classification of 5 cases is unknown; these are included only in the total column.
b Chronic skin breakdown, chronic liver disease, alcohol abuse, peptic ulcer disease, metastatic solid tumor, hematologic malignancy, transplant recipient, spina bifida, injection drug use, liver failure, human immunodeficiency virus, premature birth.
Characteristics of ESBL-E isolates tested at CDC are presented in Table 5. By reference broth microdilution testing, 122 (90%) isolates met our surveillance definition phenotype of an ESBL producer using current CLSI breakpoints. 12 Among 104 E. coli isolates meeting the surveillance phenotype by reference testing, 97 (93%) were phenotypically ESBL-screen positive. Among ESBL-screen positive E. coli, CTX-M-type β-lactamases predominated (98%), with bla CTX-M-15 being most common (56%). In total, 23 unique STs were detected among the 97 ESBL-screen positive E. coli isolates; ST131 was most common (54%) followed by ST38 (12%) and ST10 (5%). In addition to β-lactam resistance, E. coli isolates meeting the surveillance phenotype frequently displayed resistance to ciprofloxacin (75%), tetracycline (54%), trimethoprim-sulfamethoxazole (53%), and gentamicin (29%). Among 18 Klebsiella spp isolates meeting the surveillance phenotype, 17 were ESBL-screen positive and 16 carried an ESBL gene. All ESBL genes were of the CTX-M type (bla CTX-M-15 and bla CTX-M-14). In total, 11 unique STs were observed among K. pneumoniae. Among 2 K. oxytoca isolates meeting the surveillance definition, 1 harbored bla CTX-M-15 and belonged to ST11.
Table 5. Characteristics of Extended-Spectrum β-Lactamase–Producing Enterobacterales Isolates Tested at CDC, 5 Emerging Infections Program Sites, United States, 2017 (N=136)

Note. CDC, Centers for Disease Control and Prevention; ESBL, extended-spectrum β-lactamase; ST, sequence type.
a Klebsiella pneumoniae, Klebsiella oxytoca.
b Other E. coli ST types included 20 unique STs.
c Other K. pneumoniae ST types included 9 unique STs: ST17, ST37, ST323, ST462, ST869, ST896, ST1207, ST2004, ST2133.
The antimicrobial susceptibility results for ST131 and non-ST131 E. coli are presented in Table 6. ST131 isolates displayed lower levels of fluoroquinolone susceptibility (4%) than non-ST131 isolates (42%), but otherwise showed similar susceptibility profiles for other antimicrobial classes. Among 52 ST131 isolates tested, 23 (44%) were community-associated.
Table 6. Reference Antimicrobial Susceptibility Testing Results for E. coli ST131 and Non-ST131 Isolates Meeting the Surveillance Phenotype, 5 Emerging Infections Program Sites, United States, 2017 (N=104) a

Note. ST, sequence type.
a Reference antimicrobial susceptibility testing was performed and interpreted according to Clinical and Laboratory Standards Institute (CLSI) guidelines (M100 2020, 30th edition).
b % susceptible isolates include susceptible (S) and susceptible dose-dependent (SDD).
Discussion
This 3-month pilot for ESBL-E is the first report of an active laboratory- and population-based surveillance initiative conducted in the United States. Our pilot program yielded several key findings. First, we confirmed a high burden of ESBL-E, 1,Reference Jernigan, Hatfield and Wolford9 with an estimated annual incidence rate of 199.7 per 100,000 population in sites conducting population-based surveillance. Thus, the incidence of ESBL-E at surveillance sites appears to be much higher than previously published estimates for other resistant phenotypes such as carbapenem-resistant Enterobacterales (2.93 per 100,000 population per year). Reference Guh, Bulens and Mu21 In addition, only 30% of cases occurred in hospitalized patients. This finding is notable because it indicates that the high burden of ESBL-E in hospitalized patients recently described by CDC represents only a fraction of the total infection burden. 1,Reference Jernigan, Hatfield and Wolford9 Second, almost half were community-associated with no previous specified healthcare exposure. Finally, ESBL-producing E. coli isolates were predominantly ST131, and most ESBL isolates harbored bla CTX-M genes. These findings suggest that the large degree of transmission of ESBL-E that has occurred in the United States may be partly driven by a single strain that has successfully established itself in the community.
Along with previous single- or multicenter studies reporting on the changing epidemiology of ESBL-E, Reference Doi, Park and Rivera22,Reference Thaden, Fowler, Sexton and Anderson23 the high proportion of community-associated cases in our data points to the presence of person-to-person transmission or other sources of ESBL-E in the community. Recent studies through modeling and molecular characterization of ESBL isolates from Europe have suggested that most transmission of ESBL-E organisms occurs person to person. Reference van den Bunt, van Pelt and Hidalgo24–Reference Arcilla, van Hattem and Haverkate27 Currently, few community-based strategies to decrease ESBL-E incidence in the United States have proven effective. Improving antibiotic use in the outpatient setting, especially for the treatment of urinary tract infection where E. coli is the most common etiology, might help reduce selective pressure for ESBL-E. In our study, almost 40% of all cases and a quarter of community-associated cases received prior antibiotics, which might have been underestimated because we did not assess antibiotic use beyond the previous 30 days and because medical records for outpatients and hospitalized patients might lack data on prior antibiotic exposures. Reference Goyal, Dean, Neill, Jones and Dascomb28 In addition, Low et al Reference Low, Neuberger and Hooton29 suggested that outpatient fluoroquinolone use increases the community risk for acquiring fluoroquinolone-resistant E. coli even for individuals who never received fluoroquinolone treatment. Thus, antibiotic stewardship could play a role in reducing the risk of resistance not only in the individual but also across the population. A possible future strategy under development is an effective vaccine for extraintestinal E. coli infections. Reference Poolman and Wacker30 Initial studies have suggested an acceptable safety profile and immunogenicity Reference Huttner, Hatz and van den Dobbelsteen31 of a candidate E. coli vaccine, which, if successful in clinical trials of efficacy, might be a promising strategy for preventing infections from ESBL-producing E. coli in the community.
Better understanding of sources of and risk factors for acquisition in the community is necessary to inform public health measures that reduce the incidence of infections caused by ESBL-E. Some risk factors for acquisition of ESBL-E have been explored by other investigators. Reference Goyal, Dean, Neill, Jones and Dascomb28,Reference Nadimpalli, Vuthy and de Lauzanne32 Studies in both the United Kingdom and the United States suggest that the predominant ESBL strains causing disease in humans are rare in retail meat samples, other food, or animals, Reference Day, Hopkins and Wareham26,Reference Doi, Paterson and Egea33 and investigators in the Netherlands have described household hygiene behaviors Reference van den Bunt, van Pelt and Hidalgo24 and international travel Reference Arcilla, van Hattem and Haverkate27 as contributors to ESBL-E transmission. More work is needed to determine what factors are most important in the United States. This research could include investigation of sources for ESBL-E acquisition such as water sources, Reference Falgenhauer, Zur Nieden, Harpel, Falgenhauer and Domann34,Reference Haberecht, Nealon and Gilliland35 travel to high-risk countries, Reference Arcilla, van Hattem and Haverkate27 investigation of household transmission, Reference Martischang, Riccio, Abbas, Stewardson, Kluytmans and Harbarth36 or screening for antimicrobial resistance genes or ESBL-E organisms in the environment. Reference Haberecht, Nealon and Gilliland35 Investigation of geographic variation could also contribute to better understanding of ESBL-E risk factors in the United States.
Although a large proportion of ESBL-E in our study were community-associated, slightly more than half of cases occurred in persons with prior healthcare exposures. A recent systematic review and meta-analysis by Vinks et al Reference Vink, Edgeworth and Bailey37 identified a pooled acquisition prevalence of 3.73% for ESBL-E in healthcare settings in Europe and North America, and they highlighted the contribution of LTCFs in sustaining national outbreaks. Thus, efforts to reduce transmission of ESBL-E and development of infections in colonized individuals in healthcare settings 38 are also an important public health strategy for EBSL-E prevention. For example, more than a quarter of HACO cases in our pilot program had a urinary catheter in place, so ensuring proper catheter care (including removal of unnecessary catheters) might help with ESBL-E prevention.
Multiple reports have indicated that certain strain types, such as ST131 and ST38, are playing an important role in the worldwide dissemination of ESBL-producing E. coli. Reference Pitout and Laupland3,Reference Peirano, van der Bij, Gregson and Pitout39 Similarly, in the convenience sample of E. coli isolates characterized in our pilot program, ST131 predominated and displayed higher levels of fluoroquinolone resistance than non-ST131 isolates. In addition, 52% of the ST131 isolates displayed resistance to trimethoprim-sulfamethoxazole, another drug commonly used to treat community urinary tract infections. Hence, the limited availability of oral antibiotics and continued spread of ST131 represents a challenge to manage community-associated UTIs.
Determining an appropriate surveillance definition for ESBL-E is challenging. ESBL-E should test intermediate or resistant to extended-spectrum cephalosporins when using current clinical antimicrobial susceptibility testing break points. 12 However, resistance to cephalosporins Reference Belley, Morrissey, Hawser, Kothari and Knechtle40 may also result from other mechanisms, such as AmpC-type β-lactamases. Guidelines from the Clinical and Laboratory Standards Institute (CLSI) recommend ESBL confirmatory testing of K. pneumoniae, K. oxytoca, E. coli, and P. mirabilis only when laboratories have not implemented current breakpoints or for infection control purposes. 12 A high proportion of isolates tested at CDC (90%) met the pilot surveillance case definition phenotype. Thus, the definition appears to have a good positive predictive value for identifying ESBL-producing isolates. In addition, the definition was easy to use. More than 80% of cases identified from urine had a UTI diagnosis by a medical provider or had symptoms associated with a UTI documented in the medical record, suggesting that the majority were considered to represent clinical infection by the treating provider although overdiagnosis could occur. However, the use of our case definition might underestimate true ESBL-E incidence. We did not include respiratory specimens, wound cultures, or skin cultures in the definition because of added complexities with assessing clinical significance of Enterobacterales isolates from these sources. We also did not include isolates resistant to or nonsusceptible to carbapenems.
Our pilot program had several limitations as well as important strengths. First, the ESBL-E pilot data were collected for only 3 months; and therefore, we did not account for the effect of seasonality on incidence. Given that it is not known whether ESBL-E incidence has seasonal variation in the United States, our reported incidence might have been under- or overestimated, and the generalizability of incidence might be limited. Second, surveillance was population based at only 3 of the 5 EIP sites. The other 2 sites conducted sentinel surveillance because of feasibility limitations. Third, available data on prior antibiotic use in some patients may have reflected empiric treatment of the ESBL-E infection rather than use that predated and potentially increased the risk of ESBL-E infection. In addition, we may have missed data on outpatient healthcare exposures if it was not documented in the record. Finally, we had only a limited subset of E. coli and Klebsiella spp isolates for testing, and we did not evaluate susceptibility to some oral antibiotics such as nitrofurantoin. The strengths of this study included a description of ESBL-E cases in entire counties regardless of healthcare setting, diversity of geographic regions, and confirmation of ESBL gene presence.
In conclusion, ESBL-E causes a high burden of infections in the community and in healthcare, and additional data are needed to further characterize risk factors and sources of acquisition to focus prevention efforts. Our results support those of other published literature, Reference Adler, Katz and Marchaim2,Reference Tamma, Smith and Adebayo4,Reference Chen, Freeman and Nicholson7,Reference Doi, Park and Rivera22 suggesting that the CTX-M β-lactamase is the predominant mechanism among ESBL-E in the United States. Based on our findings, the EIP implemented ongoing active population-based ESBL-E surveillance at 6 US sites in July 2019 to describe ESBL-E burden in additional areas and to assess the effect of efforts to combat antimicrobial resistance among Enterobacterales over time.
Acknowledgments
We thank Sandra N. Bulens, Megan Light, Meheret Endeshaw, and Anthony Fiore (CDC); Patrick Stendel (the Colorado EIP); Sarah Satola and Alex Page (the Georgia EIP); William Hudspeth (New Mexico Department of Health); Emily Hancock Lisignoli, and Katherine Gienger (the New Mexico EIP); Dwight Hardy (University of Rochester Medical Center, Rochester, New York); Roberto Vargas (Rochester Regional Health Center, Rochester, New York); Stacy Smith, Marsha Griffs, Melissa Haymons, Carissa Black, and Kenzie McClain (Maury Regional Medical Center Microbiology Laboratory, Columbia, Tennessee). The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Financial support
This work was supported by the CDC through the Emerging Infections Program cooperative agreement (grant no. CDC-RFA-CK17-1701).
Conflicts of interest
All authors report no potential conflicts of interest.
Data availability
Raw sequences have been deposited in the NCBI BioProject (ID no. PRJNA288601).






