Infections arising after flexible endoscopy were initially attributed to endogenous infections arising from the patient’s own microbes, and the exogenous infection rate from contaminated endoscopes was deemed to be <1 in a million procedures. Reference Ofstead, Langlay, Mueller, Tosh and Wetzler1 Before 2000, outbreaks that were associated with contaminated endoscopes were recognized as “exogenous” infections only when they were due to “primary pathogens” (eg, Salmonella spp, Mycobacterium tuberculosis, etc). Reference Spach, Silverstein and Stamm2,Reference Cowen3
As stated by Cowen, Reference Cowen3 “The principal cause of endoscopy-associated infections is failure to follow recommended protocols.” Recent outbreaks of multidrug-resistant organisms (MDROs) caused by contaminated flexible endoscopes have focused attention on the inadequacies of flexible endoscope reprocessing. Reference Epstein, Hunter and Arwady4–Reference Ofstead, Hopkins, Buro, Eiland and Wetzler9
The key issues currently associated with contamination of fully reprocessed flexible endoscopes include inadequate cleaning, inadequate disinfection, and wet storage, which leads to biofilm and/or build-up biofilm (BBF) within endoscope channels and allows bacteria to survive high-level disinfection (HLD) and sterilization. Reference Alfa and Singh7,Reference Ofstead, Wetzler, Heymann, Johnson, Eiland and Shaw8,Reference Barakat, Huang and Banerjee10–17
Ofstead et al Reference Ofstead, Wetzler, Eiland, Heymann, Held and Shaw18,Reference Ofstead, Heymann, Quick, Eiland and Wetzler19 and Barakat et al Reference Barakat, Huang and Banerjee10,Reference Barakat, Huang and Banerjee11 have clearly demonstrated that the alcohol and air flush provided by an automated endoscope reprocessor (AER) is insufficient and that residual moisture in flexible endoscope channels during storage is a widespread and underrecognized problem that can lead to biofilm formation. Reference Alfa and Singh7
Using the sample collection protocol validated by duodenoscope manufacturers, 20 the extensive review by US Food and Drug Administration (FDA) of 522 clinical studies 21 reported that 5.4% of reprocessed patient-used duodenoscopes were contaminated with high-concern organisms and that an additional 3.6% of duodenoscopes contained >100 colony-forming units (CFU) of low- to moderate-concern organisms. 21
The efficacy of sample collection plays a pivotal role in effective detection of microbial contamination in patient-ready endoscope channels. Reference Thornhill and David22 The variability in sample collection and culture methods makes it difficult to compare data among different clinical studies to determine the core critical principles of sample extraction from endoscope channels. Furthermore, the underlying principles needed to interpret positive cultures and to ensure that appropriate remedial actions are taken remain unclear.
The first objectives of this review are to provide an overview of the published endoscope channel sample collection and culture methods and to create a practical guide to identify the core critical components needed to optimize this process. Our further objectives are to provide an overview of the published approaches to interpretation of positive endoscope channel cultures and to create a practical guide for clinicians and infection control specialists for investigating the root cause of endoscope contamination. Root-cause investigations are essential to determine optimal remediation measures. To identify relevant articles, we conducted a literature search of PubMed using the following terms: flexible endoscope, endoscope contamination, carbapenem-resistant Enterobacteriaceae, endoscope culture surveillance, endoscope infection outbreak, endoscope sample collection, endoscope-associated infections, endoscope culture methods, endoscope guidelines, and biofilm. This literature review did not require approval from our institutional review board.
National endoscope reprocessing guidelines: Recommendations regarding culture monitoring of endoscopes to detect contamination
The current national guideline recommendations vary widely among countries (Table 1). None of the national guidelines (Table 1) specify that endoscopes should be quarantined pending culture results. However, Ma et al Reference Ma, Pegues and Kochman28 demonstrated that quarantine of levered endoscopes was feasible if there was adequate inventory to culture 25% of these devices on a rotating basis. The US 2018 20 duodenoscope sample collection protocol (Table 1) is the only national guideline that has been validated by the 3 main endoscope manufacturers to have 65%–100% extraction efficacy for duodenoscopes (combined instrument channel sample and lever recess sample). Thornhill et al Reference Thornhill and David22 noted that it is unclear whether this extraction efficacy would reflect recovery of injured or stressed bacteria from clinically used endoscopes. To allow direct comparisons among future studies, we recommend that researchers use of the FDA/CDC/ASM 20 protocol because it is the only validated sample collection protocol.
Table 1. Summary of Published Guidelines Related to Endoscope Channel Sample Collection and Culture Methods

Note. FBF, flush–brush–flush; FB, flush–brush; F-only, flush only; B, brush only; DI, deionized; RO, reverse-osmosis; CFU, colony-forming units.
a This protocol is the only validated channel culture method in the United States, so no other guidelines for the United States are listed.
The most common sample extraction fluids recommended are sterile saline, deionized or reverse-osmosis water (Table 1). Although most guidelines recommend the use of neutralizer (either as the extraction fluid or added to the sample after extraction from the endoscope channel) and sample concentration for culture, not all recommend the use of friction (eg, bristle brush) as part of channel sample collection. The interpretation guidelines vary between countries regarding the types of organisms considered actionable and the CFU cutoffs for unacceptable levels of growth. For most guidelines, detection of <10 CFU of “environmental” sporulating organisms (eg, Bacillus, Paenibacillus etc) is not actionable and is considered to represent accidental contamination during sample collection. A similar approach is taken for low- to moderate-concern skin and oral and/or respiratory organisms (Table 1). Most guidelines have focused on “indicator organisms” that include enteric organisms and gram-negative bacilli because these have been frequently associated with MDRO infectious outbreaks due to contaminated endoscopes. Furthermore, root-cause analysis and remedial action plans are not clearly outlined in current guidelines (Table 1).
Endoscope-channel sample collection methods
Despite published national and international guidelines (Table 1), a wide range of endoscope sample collection and culture methods have been used in published clinical studies, making it difficult to compare results. Reference Thornhill and David22 Table 2 provides a summary of the published literature related to endoscope-channel sample collection for outbreak and nonoutbreak clinical studies.
Table 2. Summary of Published Clinical Studies Related to Endoscope Channel Sample Collection and Culture Methods

Note. F, flush; FBF, flush–brush–flush; FB, flush–brush.
a Actionable organisms; excluding environmental organisms.
b Sterile buffer, eg, phosphate-buffered saline, physiological saline 0.9% NaCl.
c Culture media: eg, letheen broth, tryptic soy broth.
A wide array of fluids has been utilized for extraction of channel samples including sterile deionized or reverse-osmosis water, sterile buffers, culture media, and neutralizing fluids (Table 2). These extraction fluids were used alone or in combination with friction, and the most common source of friction was the bristle brush. Neutralizer was used in 19% clinical studies, and sample concentration was used in 54% of clinical studies (Table 2). Given the wide range in channel sampling methods, it is not surprising that many nonoutbreak clinical studies reported very low detection rates of actionable bacteria whereas others had high rates.
To identify components that improve endoscope culture sensitivity, we evaluated those clinical studies with 0%–3% culture positivity rates from instrument channels only (Table 2). Clinical studies with low endoscope-culture positivity rates did not include neutralizer at the time of sample collection and did not use filtration to concentrate the sample for culture (the use of friction for sample collection varied). Reference Ofstead, Wetzler, Eiland, Heymann, Held and Shaw18,Reference Ross, Bruno and Kozarek30,Reference Becq, Snyder and Heroux31,Reference Gillespie and Kotsanas34,Reference Alfa, DeGagne, Olson and Fatima35,37,Reference Gavalda, Olmo and Hernandez45,Reference Paula, Presterl, Tribl and Diab-Elschahawi56 Those studies in Table 2 that used filtration of instrument channel samples (with or without neutralizer and with or without friction) had culture positivity rates of actionable organisms between 7.5% and 75%. Reference Ofstead, Heymann, Quick, Eiland and Wetzler19,21,Reference Cotterelli, DeGiusti and Solimini32,37,Reference Cattoir, Vanzieleghem and Florin46,Reference Cristina, Sartini and Schinca49,Reference Rauwers, Voor’in’t holt and Buijs51 Although many other variables are related to the compliance with endoscope reprocessing instructions at the different clinical sites, these data support the value of filtration to improve culture sensitivity.
We found no published studies that specifically compared the recovery of microbes from patient-ready endoscope samples when neutralizer was added versus no added neutralizer. However, Thornhill et al Reference Thornhill and David22 indicated that recovery of injured microorganisms was important, and they summarized how microbes in flexible endoscopes are damaged: “Bacteria residing in an endoscope are frequently exposed to harsh conditions such as disinfectants, nutrient starvation, desiccation and high hydrostatic pressure resulting in injury and stress that makes successful recovery difficult.” Several other published studies support the value of neutralizers (eg, NPD-thiosulfate, Letheen or Dey-Engley broth) to inactivate traces of residual HLD Reference Duc, Ribiolett, Dode, Ducel, Marchetti and Calop60 and stimulated resuscitation of damaged microbes (eg, viable but nonculturable organisms) to grow on culture. Reference Li, Mendis, Trigui, Oliver and Faucher61–Reference Dey and Engley65 Furthermore, Da la Costa et al Reference da la Costa Luciano, Olson, Tipple and Alfa66 demonstrated the ability of NPD-thiosulfate neutralizer to protect P. aeruginosa from low-level residuals (ie, 1:10 dilution) of glutaraldehyde, accelerated hydrogen peroxide, and orthopthalaldehyde. This aspect of neutralization of traces of disinfectants is especially important when the channel sample for culture is collected immediately after HLD.
Most published clinical studies (Table 2) used endoscope-channel sample collection methods in which the % extraction efficacy was unknown. Only the FDA/CDC/ASM 2018 guideline 20 used a protocol that had extraction efficacy of 65%–100%, validated by duodenoscope manufacturers.
Published data regarding optimizing endoscope channel sample extraction
The published data from research related to optimizing sample collection for endoscope channels is summarized in Table 3. The need to consider biofilm when assessing endoscope-channel sample extraction has also been recommended. Reference Thornhill and David22,Reference Aumeran54 Aumeran et al Reference Aumeran54 focused on F-only sample collection and concluded that use of a tensioactive sampling fluid provided optimal extraction for biofilm. Gazdik et al Reference Gillespie, Sievert, Swan, Kay, Edridge and Stuart74 compared extraction efficacy of the duodenoscope lever cavity using a flocked swab versus the bristle brush in the interim CDC protocol (no longer accessible; replaced by FDA/CDC/ASM 2018 protocol 20 ). Recovery improved using a flocked swab that was smaller in size compared to that of the bristle brush used in the CDC interim method. The value of friction for sample extraction from both channels and duodenoscope lever cavity was further supported by Alfa et al, Reference Alfa, Harminder and Zoann64 who used the build-up biofilm (BBF) model as well as artificial test soil (ATS). The use of a borescope to visualize the removal of BBF from polytetrafluoroethylene (PTFE) channels documented that F-only methods (regardless of the type of fluid used) did not physically remove the BBF. Borescope assessment of flush–brush–flush (FBF) protocols demonstrated that the bristle brush removed most of the BBF, but thin tracks of residual material remained, whereas the pull-through device eliminated all detectable BBF. Reference Alfa, Harminder and Zoann64 Furthermore, the tiny bristle brush used for manual cleaning of the lever cavity was significantly better at extracting E. coli from the lever cavity compared to the CDC interim cavity collection protocol that used a very large bristle brush. Reference Alfa, Harminder and Zoann64 The duodenoscope channel extraction efficacy for this FBF protocol ranged from 67% to 100% for E. faecalis and from 67% to 80% for E. coli. Reference Alfa, Harminder and Zoann64 The authors recommended sterile reverse-osmosis water in the FBF protocol for sample collection combined with addition of a neutralizer immediately after sample collection. Cattoir et al Reference Cattoir, Vanzieleghem and Florin46 followed an extraction protocol using friction, but no neutralizer was less effective than the use of friction and neutralizer by Alfa et al Reference Alfa, Harminder and Zoann64 for nonbiofilm in PTFE channels (16% to 22% vs 80% to 100%, respectively). Data from both Cattoir et al Reference Cattoir, Vanzieleghem and Florin46 and Alfa et al Reference Alfa, Harminder and Zoann64 support their recommendation for the use of friction (FPF or FBF) to improve sample collection from endoscope channels.
Table 3. Summary of published research studies evaluating efficacy of endoscope channel sample collection methods

Note. BB, Bristle brush; PT, Pull-through.
a Biofilm-EF-PA; biofilm formed by Enterococcus faecalis and Pseudomonas aeruginosa in ATS
b ATS-EF-PA-CA; ATS containing 20% blood and E. faecalis, P. aeruginosa and Candida albicans
c NPD: neutralizing pharmacopeia diluent (Tween 80; 3%wt/vol, lechithin; 0.3% wt/vol, sodium thiosulfate; 0.5% wt/vol, L-histidine; 0.1% wt/vol); added after sample extraction
d TFF: Turbulent Fluid Flow
e Build up biofilm-EF-PA formed with E. faecalis and P. aeruginosa
f ATS-EF-EC; ATS containing 20% blood, E. faecalis and Escherichia coli
g ATS-EC-PA-KP-EF; ATS containing mucin, E. coli, P. aeruginosa, K. pneumoniae, E. faecalis
h Biofilm-EF-PA; biofilm formed using Tryptic soy broth containing E. faecalis and P. aeruginosa
Ji et al Reference Ji, Ning, Fei, Liu, Liu and Song69 demonstrated that both FBF and pump-assisted extraction of endoscope channel samples were superior to flush only (F-only) sample collection. Ma et al Reference Ma, Feng and Jiang68 reported that using a brush–flush method detected more positive cultures than an F-only method for the biopsy port to distal portion of the suction channel (33.3% and 8.3%, respectively). Sohn et al Reference Sohn, Alfa, Lai, Tabani and Labib67 demonstrated that turbulent fluid flow (TFF) provides optimal friction providing 85%–95% extraction efficacy from colonoscope channels (both 3.2-mm ID and 1.37-mm ID channels) and 69%–100% extraction from biofilm-coated PTFE channels. The novel TFF technology is currently the only method that provides friction in narrow 1.37-mm ID channels and is capable of 69%–72% biofilm extraction efficacy.
Summary of key sample collection and culture factors
The key factors shown in Table 3 for optimizing extraction of microorganisms (present as biofilm or nonbiofilm residuals) from endoscope channels include type of extraction fluid, friction, and the use of a neutralizer (either as the extraction fluid or added to the sample after collection). The key factor for culture of the extracted sample (Table 2) is concentration of the entire sample, and membrane filtration is the preferred method.
Interpretation of culture results
The national guidelines (Table 1) do provide some level of interpretation of culture results in terms of the type and level of organisms detected that require action. The Australian guideline 71 is one of the few national guidelines that provides a clinical guideline for interpretation and action when endoscope culture results are positive. This guideline is stratified by the type of endoscope that has been cultured and the type and level (CFU) of organisms detected. It provides recommendations on the interpretation of the culture results, and it recommends actions that should be taken. This clinical guideline is very helpful, but it provides only limited guidance on the investigation regarding what could be causing the positive culture result and/or remediation. We recommend a more consolidated approach to culture interpretation and investigative action based on the potential source of the microorganisms detected on culture of patient-used endoscope channels.
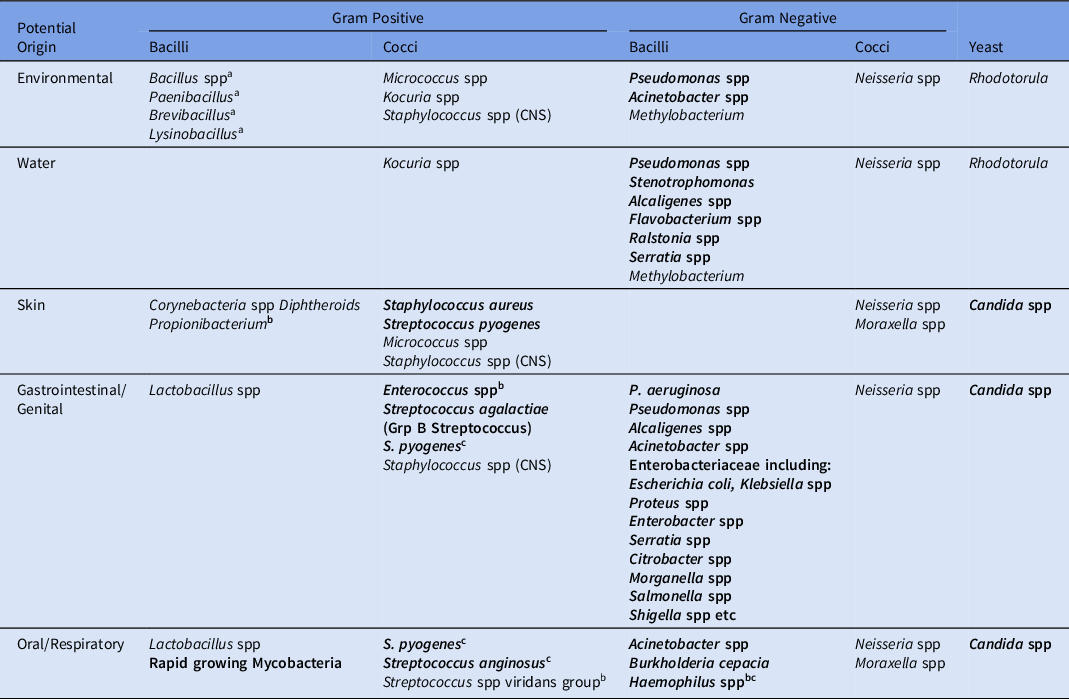
Table 4 provides an overview of the types of microorganisms that can be detected in endoscope channels when assessed by standard microbial culture methods (ie, not using specialized culture for pathogens such as Mycobacterium tuberculosis, anaerobic bacteria, Haemophilus influenzae, etc). The microbes have been stratified based on the most likely source of such microbes, recognizing that some microbes can originate from multiple different sources. As such, a logical approach needs to be taken when developing action plans as part of the investigative process to identify and eliminate the source of the microbe(s) detected when endoscope samples are culture positive. Gram-negative bacilli originating from the gastrointestinal tract (eg, E. coli, K. pneumoniae, and P. aeruginosa) have been the major causes of MDRO outbreaks associated with contaminated flexible endoscopes. Reference McCafferty, Aghajani, Abi-Hanna, Gosbell and Jensen5–Reference Alfa and Singh7,Reference Ofstead, Hopkins, Buro, Eiland and Wetzler9,72,73 As such, it is critical that this group of indicator organisms is acted on immediately regardless of the type of endoscope it is isolated from. If the isolate is an MDRO, then even transmission to another patient that results in colonization but no immediate infection is still cause for concern. Reference Alfa and Singh7,Reference Thornhill and David22 However, it is unclear whether urgent action is needed for moderate- to low-concern oral and/or respiratory or skin organisms that have some potential to cause human infections but have not been associated with MDRO outbreaks. Furthermore, the spore-forming environmental organisms and other low-concern environmental organisms are generally considered to be of little significance unless present in elevated numbers. This assumption has been questioned by Bridier et al, Reference Bridier, del Pilar Sanchez-Vizuete and Le Coq14 who documented that B. subtilis isolated from an AER and resistant to peracetic acid can form biofilm that can protect a sensitive strain of Staphylococcus aureus from being killed by peracetic acid (ie “bystander protection” from HLD). This finding highlights the importance of ensuring that endoscope channels are thoroughly dry during storage to prevent low- to moderate-concern organisms from replicating and forming biofilms that could protect indicator organisms. Reference Alfa and Singh7,Reference Bridier, del Pilar Sanchez-Vizuete and Le Coq14
Table 4. Potential Origins of Organisms Detected by Aerobic Culture of Endoscope Channels

Note. CNS, coagulase-negative Staphylococcus spp; CFU, colony-forming units. Bolded bacterial names: indicator organisms (same as organisms of concern 20 ): Action required. Nonbolded bacterial names: low- to moderate-concern organisms: no action, alert, or action based on CFU cutoff indicated in national guidelines (Table 1).
a Spore-forming bacilli.
b Some guidelines consider these bacteria as indicator organisms and other guidelines do not.
c Will not grow on basic media (eg, nutrient agar, tryptic soy agar, R2A, etc).
The various national guidelines listed in Table 1 all have actionable criteria but the “cutoff CFU” level requiring action versus alert varies as does the type of “indicator organisms” requiring action versus alert. We recommend focus on a practical “Clinical Investigation and Remediation Plan” that should be initiated based on the type of organism(s) detected. The approach we recommend is outlined in Table 5 for organisms requiring action as defined by the specific guidelines listed in Table 1. Detection of any of the indicator organisms or low- to moderate-concern organisms (shown in bold) that exceed the CFU cutoff listed in Table 4 from any flexible endoscope require immediate quarantine until the relevant repeat reprocessing and reculture procedures have been performed. (The cutoffs for action vary based on the specific country’s guideline.) Only if the reculture result is acceptable should the endoscope be released for clinical use (Table 5). Table 5 also provides a checklist indicating the specific aspects that should be investigated (including appropriate testing) based on the type of microorganisms detected. All detected shortcomings must be rectified. All audits and data obtained are critical aspects that should be reviewed with all reprocessing and clinical staff after the investigation has been completed. Actions taken to correct problems identified by the audits may require re-education, change of equipment, or revision of on-site protocols. In addition, a follow-up audit is needed to ensure that the recommended changes have been adequately implemented.
Table 5. Investigation for Action Level Due to Any Level of Indicator Organisms or Low- to Moderate-Concern Organisms That Exceed the CFU Cutoff Level of the National Guideline

Note. CFU, colony-forming units; GI, gastrointestinal; Env, environmental; Resp, respiratory; AER, automated endoscope reprocessor; PPE, personal protective equipment; MEC, minimum effective concentration; MIFU, manufacturer’s instructions for use; HLD, high-level disinfection.
a Negative control test: Have staff who normally collect endoscope channel samples do a “mock” manipulation in the same location they use for endoscope testing. Mock test: Place sterile mat on surface used for endoscope sample collection, use appropriate PPE as per channel collection protocol. Remove sterile brush from packaging and cut bristle off into sample collection fluid container then add sterile neutralizer fluid. This sample is sent for culture as per other channel samples and should show no growth. If growth is detected the staff need retraining in aseptic technique.
b The flushing pump tubing should not contain microbial biofilm. If the flushing tubing is visibly discolored this suggests biofilm may be present. A sterile swab should be inserted into the discolored tubing and submitted for culture. Any growth of indicator organisms indicates the tubing needs to be changed and the disinfection protocol reviewed to ensure the method and frequency recommended by the manufacturer are followed.
c The rapid cleaning tests currently available include kits that evaluate adenosine triphosphate or organic markers such as protein, carbohydrate and hemoglobin. Current guidelines recommend these tests to ensure that staff receive immediate feedback regarding adequacy of manual cleaning of endoscope channels as part of a quality system program. 21,72
d Although not required by all national and international guidelines the need to evaluate the quality of the final rinse water is important as published data Cotterellii et al Reference Cotterelli, DeGiusti and Solimini32 has revealed that final AER rinse water can be contaminated with indicator organisms and may be the basis for contaminated patient-ready endoscope channels. Those guidelines that recommended culture of final rinse water from AERs recommend filtration of 100 mL final rinse water that is aseptically collected at the end of an AER cycle and concentrated using filtration for culture. There should be no detectable CFU in the 100-mL sample.
e Moisture in endoscope channels has been demonstrated to be a widespread and underrecognized problem. Reference Alfa and Singh7,Reference Barakat, Huang and Banerjee11,Reference Ofstead, Heymann, Quick, Eiland and Wetzler19 It is crucial that drying prior to storage is thorough. This can be achieved using validated automated air-flushing pumps used prior to placing the endoscope in a regular storage cabinet or by using validated channel-purge storage cabinets. Moisture in endoscope instrument channels after overnight storage can be evaluated using a borescope, or it can be evaluated using cobalt chloride strips. Reference Barakat, Huang and Banerjee11,Reference Ofstead, Heymann, Quick, Eiland and Wetzler19 If moisture is detected, the site should implement a validated channel drying method.
Even without a positive culture for indicator organisms, we recommend periodically performing audits of the 7 key stages (except culture of AER rinse water) listed in the first column of Table 5.
When low- to moderate-concern organisms are detected in levels deemed to be an alert situation (according to relevant national or international guideline used), then Supplementary Table 1 (Supplementary Material online) provides a checklist of specific aspects to review with staff and subsequently assessed for compliance using observational audits. Low- to moderate-concern organisms have not been associated with outbreaks of MDROs, but an alert level of such organisms indicates breaches in some aspect(s) of the reprocessing and/or sample collection protocols that warrant investigation. In the alert situation, the endoscopes do not need to be removed from patient use, but a review of core steps should be conducted with staff and an observational audit should be performed to ensure that appropriate processes are used. If alert levels persist, then remedial action to improve reprocessing is essential.
The approach outline above is somewhat similar to those in the Australian guidelines 71 and the US guidelines 20 but it includes a more detailed outline of the investigation needed stratified by the type of organisms detected. It is crucial that as the data from the investigations recommended in Tables 5 and Supplementary Table 1 (Supplementary Material online) are completed, the results are reviewed with the reprocessing and clinical staff and retraining (where necessary) is undertaken. To ensure sustained compliance with remedial actions repeat endoscope cultures and a follow-up observational audit are warranted. Cristina et al Reference Cristina, Sartini and Schinca49 noted that “prompt signaling” for nonconformity after implementation of remedial actions is needed to quickly correct the situation.
Quality monitoring
The FDA 21 and CDC 72 have both recommended that healthcare facilities offering endoscopy services should implement quality systems for endoscope reprocessing. The CDC on-line tool kit provides a useful, detailed “Gap Analysis and Risk Assessment” tool related to reprocessing flexible endoscopes. 73 The latest FDA recommendations 21 state the following:
-
Consider using duodenoscopes that have disposable components, if available at your facility; this design may lower but not eliminate risks of infection.
-
Ensure that staff are meticulously following reprocessing instructions.
-
Institute a quality-control program that includes sampling and microbiological culturing, and other monitoring methods.
-
Consider reprocessing with supplemental measures such as sterilization or use of a liquid chemical sterilant processing system consistent with the device’s labeling.
-
Monitor your reprocessing procedures. Examples of monitoring are sampling and culturing using the Duodenoscope Surveillance Sampling & Culturing (/media /111081/download): Reducing the Risks of Infection developed by the FDA-Centers for Disease Control and Prevention-American Society of Microbiology Working Group on Duodenoscope Culturing.
-
Develop schedules for routine inspection and periodic maintenance in accordance with the duodenoscope manufacturer’s instructions.
Rapid methods such as adenosine triphosphate (ATP) tests Reference Rauwers, Voor’in’t holt and Buijs51,Reference Gillespie, Sievert, Swan, Kay, Edridge and Stuart74,Reference Olafsdottir, Wright and Smithey75 and detection of metabolically active gram-negative organisms Reference Singh, Duerksen and Schultz76 have been evaluated as methods to detect contamination in patient-ready endoscopes. The current rapid ATP tests are useful for monitoring manual cleaning, but they are not sensitive enough to detect low levels of viable microorganisms and should not be used to replace more sensitive culture methods. Reference Rauwers, Voor’in’t holt and Buijs51,Reference Olafsdottir, Wright and Smithey75 The overnight incubation needed for detection of metabolically active gram-negative bacteria limits the usefulness of this approach. Reference Singh, Duerksen and Schultz76 Rapid genetic amplification methods have been shown to be feasible, Reference Valeriani, Agodi and Casini77 but they are not yet commercially available.
Despite the FDA recommendation to culture duodenoscopes as part of a quality system program, a recent review of endoscopy practices in the United States Reference Thaker, Muthusamy and Sedarat78 has indicated that implementation of culture of flexible endoscopes has been limited (53.4%). The frequency of culturing duodenoscopes varied, with some sites taking culture samples after every procedure and others performing culture on a weekly, monthly, or quarterly basis. Reference Thaker, Muthusamy and Sedarat78 The GESA/GENCA 23 guideline is one of the few to specify the frequency of culture for different types of endoscopes, with frequencies ranging from monthly to quarterly (Table 2). In 2015, Sauvic et al Reference Saviuc, Picot-Guéraud and Cheong Sing57 reported, “In conclusion, despite a rigorous and controlled organization and the use of AER devices, endoscope reprocessing control remains imperfect. Microbiological surveillance testing continues to be necessary to raise awareness in personnel responsible for reprocessing and guarantee that they respect good practices and detect endoscopes or AERs requiring technical maintenance.” Despite published data and guidelines recommending endoscope culture, little has changed since 2015. The need for periodic culture surveillance of flexible endoscopes remains an important issue, as reflected by the actionable culture-positive rate of 9% reported in the FDA postmarket surveillance study. 21 As Thornhill et al Reference Thornhill and David22 states, “As healthcare providers increasingly rely on microbiological culture results to monitor reprocessing efficacy, it’s important to understand how sampling methods and culture conditions may impact those results.” This assertion is further supported by Ma et al, Reference Ma, Pegues and Kochman28 who concluded, “… we believe periodic culturing provides the most effective and widely available tool to detect system flaws that could increase the risk of transmission of infectious agents.”
In summary, although the frequency of culture is left up to the site, 20 we recommend that some flexible duodenoscopes (including all ultrasound endoscopes with a lever mechanism) at each site be cultured each week such that ALL duodenoscopes are cultured at least once per month as part of a prospective quality systems program. If this culture frequency is not achieved, minimally, we recommend performing periodic observational audits of the steps listed in column 1 of Table 5 to determine staff compliance levels. These 2 approaches will provide ongoing data that provide feedback to the clinical and reprocessing staff in the endoscopy unit to ensure that contamination of endoscopes does not become a “silent” problem that leads to unrecognized transmission of “indicator organisms” to patients. The investigative approach recommended in this review will ensure that monitoring of manual cleaning and monitoring of dry storage are routinely assessed to ensure that they are not overlooked as part of the quality process for endoscope reprocessing.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/ice.2021.128.
Acknowledgments
Financial support
No financial support was provided relevant to this article.
Conflicts of interest
Dr Singh reports personal fees from Amgen Canada, personal fees from Roche Canada, personal fees from Sandoz Canada, personal fees from Takeda Canada, personal fees from Guardant Health Inc, outside the submitted work. Dr Alfa reports personal fees from Olympus America, personal fees from Steris, personal fees from Heathmark Industries, personal fees from Kikkoman, Japan, personal fees from University of Manitoba, personal fees from Ruhof, personal fees from 3M, outside the submitted work.