



Carbapenem-resistant Enterobacteriaceae (CRE) have emerged as important pathogens causing healthcare-associated infections associated with significant morbidity and mortality.Reference Logan and Weinstein1 Colonization with CRE usually precedes infection and has been regarded as a risk factor associated with CRE-associated infection during hospital stay.Reference Dickstein, Edelman, Dror, Hussein, Bar-Lavie and Paul2 Among hospitalized CRE carriers, the rate of subsequent CRE-associated infections ranged from 8.8% to 25.5%.Reference Schechner, Kotlovsky and Kazma3–Reference Correa and Fortaleza7 Risk factors contributing to these infections can be categorized into device or procedure-related factors (ie, urinary catheter insertion, central venous catheter insertion, and presence of tracheostomy), comorbidities (ie, diabetes mellitus, solid tumor, and immunocompromised status), and hospitalization and colonization characteristics (ie, intensive care admission and number of colonization site). However, only few studies have evaluated the impact of antibiotic use on subsequent CRE-associated infection, mortality, length of stay, and duration of CRE colonization among hospitalized CRE carriers.Reference Schechner, Kotlovsky and Kazma3,Reference Borer, Saidel-Odes and Eskira4,Reference Correa and Fortaleza7 The primary aim of this study was to determine the rate of and contributing factors to subsequent CRE-associated infections among hospitalized CRE carriers. The secondary aim was to evaluate in-hospital mortality, length of stay, and CRE colonization characteristics.
Methods
We conducted a prospective cohort study among adult inpatients (aged ≥18 years) with CRE colonization detected during hospitalization between June 1, 2015, and December 31, 2018, in Thammasat University Hospital (TUH), a Thai tertiary-care hospital with an admission rate of ~55,000 patients and ~225,000 patient days per year. This study was approved by the Faculty of Medicine, Thammasat University Ethics Committee.
The patients included in this study were prospectively identified using the daily reports of clinical specimen and rectal swab culture results from the TUH microbiology laboratory. We reviewed patients’ medical records and relevant information for eligibility. We included patients with CRE colonization at any 1 or more sites of the body but no clinically infection. Only the first colonization detected during the study period for each patient was included. The exclusion criteria were death, being transferred, or being discharged from the hospital within 48 hours after the colonization detection. The included patients were followed in the hospital until death or being discharged. According to the TUH protocol, all patients who had CRE colonization or infection were isolated with contact precautions. If a patient had initial CRE colonization detected in clinical specimens other than a rectal swab, additional rectal swab culture for CRE was performed. Follow-up cultures for CRE were performed at the colonization or infection sites every week until the cultures were negative 2 consecutive times. We considered the time point of the first negative culture as the end of CRE colonization. We defined the duration of colonization as the time from the detection of the first CRE-positive specimen to the time all follow-up specimens were CRE negative. Additional rectal swab cultures were performed for patients who shared a room with newly diagnosed CRE infection or colonization or who received care from healthcare workers who also cared for patients with newly diagnosed CRE infection or colonization. CRE decolonization (ie, using chlorhexidine bath) was not performed at TUH. Rectal swabs and clinical specimens were inoculated on blood and MacConkey agar plates. The growing colonies were further identified for Enterobacteriaceae using biochemical tests. Antibiotic susceptibility testing was performed and interpreted according to the Clinical Laboratory Standards Institute criteria. The minimal inhibitory concentrations were analyzed using a Vitek-2 automated system (bioMérieux, Marcy-l’Étoile, France). Additional susceptibility testing for tigecycline, colistin, and fosfomycin was performed, and these results were interpreted according to the European Committee on Antimicrobial Susceptibility Testing criteria.
Receipt of antibiotic was defined as receipt of at least 1 drug from that antibiotic class for at least 48 hours and was categorized by the period of receipt (prehospitalization and during hospitalization). Subsequent CRE infection was defined as development of infection documented by positive cultures from clinical sites (at least 1 specimen) with clinical signs and symptoms correspondent with the sites of infection, which occurred after the detection of CRE colonization. Prolonged colonization was defined specifically for this study as having CRE colonization at any site for >30 days. All analyses were performed using SPSS version 22.0 software (SPSS, Chicago, IL). Adjusted odd ratios (aORs) and 95% confidence interval (CI) were calculated in multivariable logistic regression analysis to determine factors associated with subsequent CRE-associated infection.
Results
Of the 191,815 culture specimens sent during the study period, CRE were isolated from 187 of the 18,255 first culture specimen, of which 125 represented patient colonization. In total, 100 eligible patients were included in the final cohort (Fig. 1 and Supplementary Material online). The median age was 74 years (interquartile range [IQR], 63–82 years), and 52% were female (Table 1). A half of the cohort patients received antibiotics within 3 months prior to admission, and the 3 most common antibiotics received were cephalosporins (21%), penicillins (17%), and carbapenems (14%). Between admission and the time colonization was detected, 85% of the patients received antibiotics. The 3 most common antibiotics received during this period were penicillins (49%), cephalosporins (41%), and carbapenems (36%). Common specimens that CRE colonization by which first detection occurred were rectal swab (37%), urine (26%), and sputum (24%). Most of the CRE were Klebsiella pneumoniae (78%). Most of the patients had indwelling urinary catheters (80%) and had been on a ventilator (62%). The median number of colonization sites was 2, and the median duration from admission to CRE colonization detected was 19 days (Table 1).
Table 1. Baseline Characteristics, Colonization Characteristics and Outcomes of the Patientsa
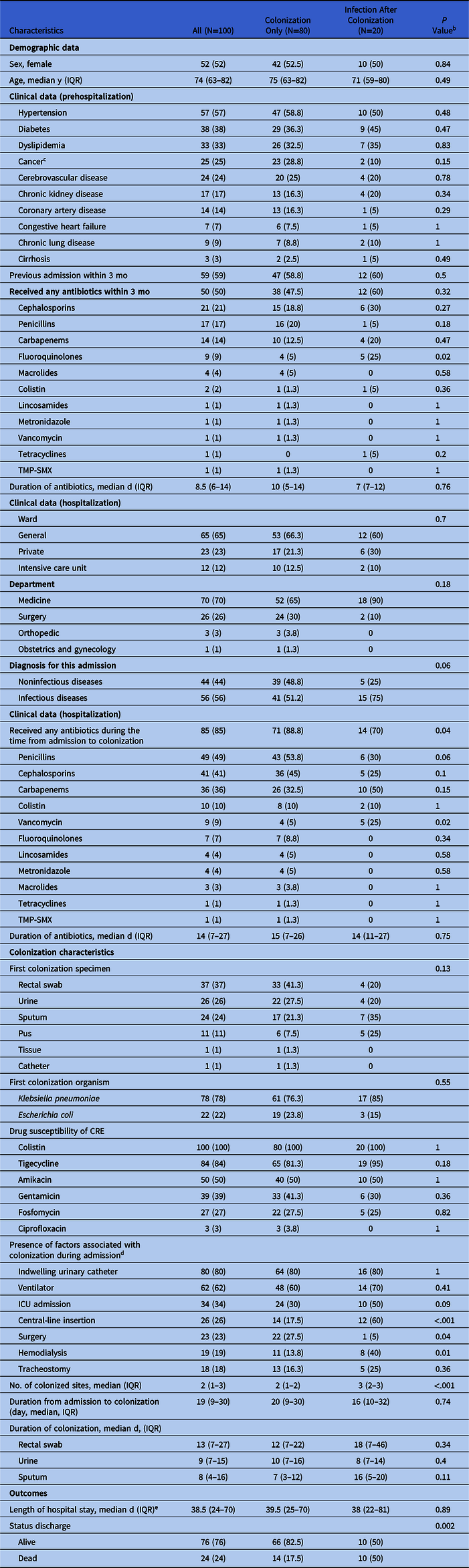
Note. CRE, carbapenem-resistant Enterbacteriaceae; ICU, intensive care unit; IQR, interquartile range; TMP-SMX, trimethoprim-sulfamethoxazole.
a Data are in no. (%) unless indicated otherwise.
b Comparing between patients with colonization only and those who developed infections after colonization.
c Included leukemia, lymphoma and cancers of urinary bladder, brain, breast, bile duct, colon, liver, larynx, lung, lymphoma, ovary, pancreas, prostate gland and rectum.
d Each patient could have one or more factors associated with colonization.
e Excluding the patients who died in both groups.
Of the 100 patients colonized by CRE during admission, 20 (20%; 95% CI, 12%–28%) developed subsequent CRE-associated infections. The median time from colonization detection to infection was 13 days (IQR, 6–30 days). The sites of subsequent CRE infections included bloodstream (45%), respiratory tract (30%), and urinary tract (15%). All bloodstream infection cases were central-line associated. By multivariable logistic regression analysis (Table 2), independent factors associated with subsequent CRE-associated infection were number of colonization sites (aOR, 7.98; P < .001 for each colonization site more), central-line insertion (aOR, 7.97; P = .009) and receipt of vancomycin during the time from admission to colonization (aOR, 24.77; P = .02).
Table 2. Multivariable Logistic Regression for Factors Associated With Subsequent Carbapenem-resistant Enterobacteriaceae (CRE) Infections

Note. OR, odds ratio; CI, confidence interval.
The median length of hospital stay was 38.5 days, and 24% of the patients died during their admission. The patients with subsequent infection had significantly higher hospital mortality than those without infection (50% vs 17.5%; P = 0.002), but they had comparable length of hospital stay (Table 1). Among the 20 patients with subsequent CRE-associated infections, all were treated with colistin-based regimens for 14 days: intravenous colistin plus fosfomycin (N = 8), intravenous colistin plus tigecycline (N = 6), intravenous colistin plus amikacin (N = 4) and intravenous colistin plus inhaled colistin (N = 2). Only 10 of the 20 patients (50%) achieved microbiological cure and survived.
Of the 100 study patients, 23 patients were discharged from the hospital while their latest CRE cultures were positive at the colonization sites and could not be followed. Among 77 patients who were evaluable for the duration of CRE colonization, 13 (17%) had prolonged CRE colonization. At the time the first culture turned negative for CRE, 20 of 77 patients (26%) were colonized by other bacteria at the previously CRE-colonized sites. Of these, 15 (75%) were colonized by Acinetobacter baumannii and 5 (25%) were colonized by Pseudomonas aeruginosa. Compared to patients without prolonged colonization, those with prolonged colonization tended to have longer length of hospital stay (70 vs 39 days; P = .07) and longer median duration of antibiotic use during the time from admission to colonization (15 vs 12 days; P = .07). We detected no significant differences in demographics, comorbidities, antibiotic use, and other risk factors for colonization between the 2 groups.
Discussion
The 20% rate of subsequent CRE-associated infection among hospitalized CRE carriers in this study was higher than those reported in other studies, summarized in Table 3 (Supplementary Material online). The higher rate compared to previous studies could be due to the broader active colonization surveillance including both rectal swab and other clinical specimen cultures and the higher proportion of overall study patients who were at risk for developing infection, including those with comorbid cancer, urinary catheter insertion, ventilator support, and those admitted to an ICU.Reference Schechner, Kotlovsky and Kazma3–Reference Correa and Fortaleza7
Independent factors associated with subsequent CRE-associated infection were higher number of colonized sites, central-line insertion, and receipt of vancomycin during the time between admission and colonization. The higher number of colonized sites represents the increased chance of infection through CRE-colonizing sites while a central venous catheter could serve as a route for CRE to travel from contaminated skin to blood vessels. Previous studies have identified prior use of fluoroquinolones, antipseudomonal penicillins, and carbapenems as independent factors associated with subsequent CRE-associated infections.Reference Schechner, Kotlovsky and Kazma3,Reference Borer, Saidel-Odes and Eskira4,Reference Correa and Fortaleza7 Given the broad-spectrum antibacterial activity of these antibiotics but no activity against CRE, selective pressure likely explains the ongoing growth and invasiveness of CRE among the carriers. Vancomycin use was independently associated with subsequent CRE-associated infection, which has not been previously described. The associated risk of vancomycin could be explained by the effect of vancomycin in eradicating the skin commensals, coagulase-negative staphylococci that protect against colonization by gram-negative bacteria, including CRE.Reference Grice and Segre8
Previous studies have demonstrated higher rates of mortality among inpatients with subsequent infection compared to those with colonization only.Reference Borer, Saidel-Odes and Eskira4,Reference Giannella, Trecarichi and De Rosa5 These results were consistent with our study’s findings and suggest the mortality burden of CRE-associated infection. Significantly longer length of stay in patients with subsequent CRE-associated infection has also been described.Reference Giannella, Trecarichi and De Rosa5 However, we did not find a significant difference in the length of stay between the 2 groups. This finding may have been due to other comorbid conditions of our patients rather than CRE infection that affected their length of stay.
The median duration of CRE colonization was 13 days, which was shorter than those reported in the 2 previous studies (387 and 165 days).Reference Zimmerman, Assous, Bdolah-Abram, Lachish, Yinnon and Wiener-Well9,Reference Haverkate, Weiner and Lolans10 The differences could be explained by the differences in study designs that allowed for determining accurate period of CRE colonization, study settings (after hospital dischargeReference Zimmerman, Assous, Bdolah-Abram, Lachish, Yinnon and Wiener-Well9 and during long-term acute-care facility stayReference Haverkate, Weiner and Lolans10 vs during acute-care hospital stay in our study) and the impact of colonization by other endemic bacteria, including A. baumannii and P. aeruginosa (26% of the first CRE-negative culture) in our setting. These organisms were likely to compete with CRE for colonization and may have shortened the duration of CRE colonization. However, the significance of the competing colonization needs to be evaluated in further studies. Factors associated with prolonged colonization among the study patients were longer length of hospital stay and longer duration of antibiotic use between admission and detection of colonization. These findings suggest the importance of minimizing length of hospital stay and duration of antibiotic use to shorten the duration of CRE colonization. Given that patients who had long-term indwelling devices tended to receive the extended duration of antibiotics, long-term indwelling device may influence the duration of CRE colonization and interact with the effect of antibiotic duration. Due to the small sample size, we did not detect a difference in the proportion of patients on long-term indwelling devices between those with and without prolonged colonization. Further studies are needed to determine the effect of long-term catheter on duration of colonization.
This study had several limitations. The generalizability of the results to other settings with differences in patient characteristics and protocols for surveillance and prevention of CRE transmission may be limited. Our sample size was small, and the genotypic testing for the CRE strains was not performed to determine the association between the colonizing and infecting isolates. The strengths of our study were inclusion of hospital-wide CRE-positive clinical specimens and rectal swab and the protocol-based weekly obtaining of the cultures for CRE that ensured accurately determining duration of CRE colonization.
In conclusion, the rate of subsequent CRE-associated infection was high among our hospitalized CRE carriers. CRE-colonized patients who have multiple sites of colonization, central-line insertion, and receipt of vancomycin between admission and colonization should be closely monitored for subsequent infection and empirically treated with CRE-active antibiotics if infection occurs. Implementation of antibiotic stewardship programs and infection control measures to restrict unnecessary and inappropriate use of indwelling devices are important in reducing the risk of CRE infection, shortening the duration of colonization, and preventing CRE transmission.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/ice.2020.220
Acknowledgments
We thank Infection Control Division and Microbiology Laboratory of Thammasat University Hospital for provision of patient and microbiology database.
Financial support
No financial support was provided relevant to this article.
Conflicts of interest
All authors report no conflicts of interest relevant to this article.





