

INTRODUCTION
The Government of Uganda adopted structural adjustment programmes in the 1980s and the early 1990s. This resulted in the decentralization and privatization of clinical veterinary services and the downscaling of civil services (Haan and Umali, Reference Haan and Umali1992). Clinical services, breeding and spraying for tick control were privatized, while vaccination of animals against epidemic diseases, quarantines and tsetse control were retained under the Ministry of Agriculture, Animal Industry and Fisheries (MAAIF). The purpose of these reforms was to reduce the costs of public administration and to cut public expenditure. Although the share of public administration costs as a proportion of public expenditure declined, this effect was offset by the following problems: First, there was an increased cost of budget financing resulting from a significant increase in interest rates caused by the increase in public budgetary support and the inflow of foreign aid (Lister et al., Reference Lister, Wilson, Steffensen and Williamson2006). Second, the creation of additional districts under decentralization resulted in increased public expenditure and stressed the capacity and accountability of both local governments and the central government. Corruption and financial indiscipline have also become serious problems, undermining the partnership between government and donors (Lister, Reference Lister2006). These problems also affected the financing of veterinary service delivery, thus weakening the governance of veterinary services. However, studies that examine the nature of these governance challenges and the actions and motivation of actors involved in the provision of veterinary services are limited, in spite of the need to identify critical intervention points in animal disease control (Rich and Perry, Reference Rich and Perry2010; Schwabenbauer, Reference Schwabenbauer2012).
This study applies Social Network Analysis (SNA) to examine the governance problems and identify influential actors in the prevention, treatment and control of animal diseases. Social Network Analysis has become an important approach for analyzing governance problems in health systems because many of problems with the provision of health care are relational (Luke and Harris, Reference Luke and Harris2007). For example, Blanchet and James (Reference Blanchet and James2012) have used SNA tools to examine health care systems in Ghana. Provan et al. (Reference Provan, Nakama, Veazie, Teufel-Shone and Huddleston2003) have also applied these tools to assess inter-organizational collaboration in disease prevention and health promotion.
Most of the SNA studies use mathematical processes to estimate structural measures of centrality such as ‘degree’, ‘betweenness’ and ‘closeness’ and ‘centrality’ to examine actors’ perceived influence or power (Borgatti, Reference Borgatti2005; Freeman, Reference Freeman1979; Stephenson and Zelen, Reference Stephenson and Zelen1989). While potentially useful, these measures often turn out to be confusing and contradictory or non-consistent (Freeman, Reference Freeman1979; Stephenson and Zelen, Reference Stephenson and Zelen1989). They do not account for the fact that the behaviour, decisions and interests of actors are socially determined (Krackhardt, Reference Krackhardt1987; Mizruchi and Potts, Reference Mizruchi and Potts1998). For example, if peripheral actors are able to directly influence one another, the central actor becomes the least powerful node in the network (Mizruchi and Potts, Reference Mizruchi and Potts1998). As a result, relating results from mathematically computed indicators with reality in meaningful ways often become a challenge. As an alternative approach, one could ask respondents to directly state the actor's perceived influence or power level (Krackhardt, Reference Krackhardt1987).
A promising new approach to SNA is the use of participatory social network mapping tools, which rely on the visualization of networks by respondents. Examples are the ‘Net-Map’ and ‘Process Net-Map’ tools, which use group-based interviews and mapping techniques. These tools have proved to be very useful for both collecting network data and performing a meaningful qualitative analysis of social network data because they generate the social network and identify at the same time the social-political relations underlying the social network (Gessa et al., Reference Gessa, Poole and Bending2008; Hogan et al., Reference Hogan, Carrasco and Wellman2007; Schiffer and Hauck, Reference Schiffer and Hauck2010). As further detailed in the Materials and Methods section, respondents first identify the relevant actors and their relations before they are asked to rate the power that they perceive each actor to have by using a visual aid. In the process, respondents are asked to verbally provide the reasons why different actors have the influence level attributed to them. The respondents may either be key informants or actors who are themselves part of the network. The visualization of the network of actors can be done using computer aids, or through pen and paper. The paper-based approach of arranging ties between actors typically yields more reliable results because they are visually appealing and can usually be understood more easily and instantly than maps generated with the use of computer aids (Hogan et al., Reference Hogan, Carrasco and Wellman2007). Moreover, the participatory mapping tools are flexible and provide room for clarification of concepts during the interview. However, some of the challenges involved in these participatory or qualitative techniques include the following: Defining the boundaries of the network (Heath et al., Reference Heath, Fuller and Johnston2009), and information distortions resulting from question-order effects as well as recall failures (Pustejovsky and Spillane, Reference Pustejovsky and Spillane2009).
In this paper, the participatory SNA tool called Process Net-Map was used to examine governance challenges involved in the provision of veterinary services. This tool has been developed by Birner et al. (Reference Birner, Cohen and Ilukor2010), and is based on the work of Schiffer and Waale (Reference Schiffer and Waale2008) with the aim to identify governance challenges encountered in the implementation of development projects (see also Raabe et al., Reference Raabe, Birner, Sekher and Gayathridevi2010; Schiffer and Hauck, Reference Schiffer and Hauck2010). The tool was applied in this study to identify influential actors in the provision of veterinary services, to study their interpersonal interactions and to identify the governance challenges in different types of service provision. The Process Net-Map tool is used to map the consecutive steps of the process under consideration, and it identifies the actors involved in this process. Thus, the tool circumvents the challenge of defining boundaries of a social network because it follows a defined process and induces respondents to the list of actors involved from the start to the end of the process. Moreover, questions are sequentially ordered as respondents are being asked to describe the process step by step. This makes it easier for respondents to use a recall approach. In the original Net-Map tool, respondents were asked to identify all actors who influence a certain outcome, an approach that makes recall more challenging. In this study, the Process Net-Map tool was used to generate evidence on how social and power relations influence the design and implementation of veterinary policies and the functioning of veterinary institutions. The tool was also used to identify possible strategies for intervention. The results were validated by conducting individual interviews with experts in animal health service delivery, such as representatives of the agricultural ministry and district governments, opinion leaders and veterinarians working with international and local government organizations. The application of the tool is further described in Section 2. The results are presented in Section 3 and synthesized and discussed in Section 4. In Section 5, the paper presents the conclusions. The results are presented in eight categories, distinguishing between clinical and preventive services, and between pastoral and intensive systems, so as to identify the actors and governance problems in each of these systems.
MATERIALS AND METHODS
The data for this study was collected using the Process Net-Map tool introduced above. The application of the Process Net-Map tool involved three phases: In Phase 1, respondents were asked in a step-by-step procedure to describe the process of delivery of animal health services and to identify the actors involved in each step, starting, for example, with the detection of a sick animal. As indicated above, the focus on the process of service delivery provided a reliable way to obtain data on established patterns of interaction between actors because it enabled participants to narrate what actually happens according to their own ‘real world’ experience. The name of each actor mentioned by the respondent was written by the interviewer on a small card and placed on a large sheet of paper. Arrows with different colours were drawn by the interviewer to represent different steps identified by respondent. This led to the Process Net-Map, as shown in Figure 1. In this study, the main links between actors, which are generated by the delivery process, are information flows regarding the disease and the resource flow involving drugs and money. Additional actors where added by the interviewer on the map whenever the participants recalled those. The arrows were marked with numbers, and the respective implementation step corresponding to each number was noted down at the border of the paper, as shown in Picture 1. The description of the process was continued until the point was reached where the animal was treated or vaccinated and the respective payments were made.
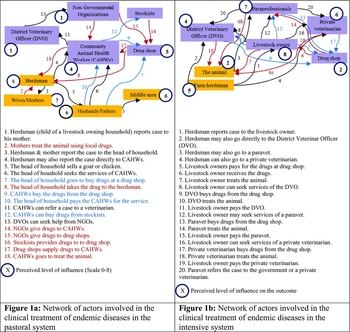
Figure 1. Network of actors involved in the treatment of endemic diseases.

Picture 1. Picture of Process Net-Map.
In Phase 2, the respondents were asked to identify the level of influence that each actor had on achieving the outcome of interest here, ensuring that the sick animal is treated or vaccinated correctly. To visualize these influence level of each actor, checkers game pieces were stacked on top of each other to build the so-called ‘influence towers’ and place them next to the actor in question. One to eight pieces were stacked on top of each other to show the level of influence of an actor, as perceived by the respondent (see Picture 1). The actors who were considered not to have any influence on the outcome were not assigned any checkers game pieces. Accordingly, actors with influence towers comprising eight checkers game pieces were perceived to be the most influential actors, while those without any checker game pieces were considered to be the least influential actors. Respondents were asked to adjust towers as they deemed necessary during the interview and to verbally provide the reasons why different actors had the influence level attributed to them. The visualization of influence levels during the interview serves as a useful tool to elicit information. In particular, it makes possible to easily ask the respondent to explain the influence levels of different actors vis-à-vis each other, which would be difficult without visualization, especially if the number of actors is large (Birner et al., Reference Birner, Cohen and Ilukor2010; Schiffer and Hauck, Reference Schiffer and Hauck2010).
In Phase 3, the respondents were asked to identify potential problem areas, which are likely to make veterinary service delivery ineffective. The focus was placed on eliciting the main governance problems that are known from the literature (see above) as well as other problems that may not have received much attention in the literature so far. Every individual participant was asked during the interview to share his or her experience on this question.
As shown in Table 1, a total of eight Process Net-Maps were produced for the study. In addition, 18 individual interviews without Net-Maps were conducted. The individual interviews were held with officials at the agricultural ministry, district governments, opinion leaders and veterinarians working with international development agencies and local government organizations. On average, about 20 people participated in each Process Net-Map exercise. Out of the 18 interviews without Net-Maps, 12 were conducted prior to conducting the Process Net-Map exercise. These interviews served to gain initial insights into veterinary service delivery in the case study areas and to ensure the selection of appropriate persons to be included in the Process Net-Map exercise. Six interviews were conducted afterwards to cross-check and validate the information generated from the Process Net-Map exercise. In each district, four Process Net-Map exercises were conducted. Two were conducted with both male and female farmers in each village, and with local leaders and at least two paraprofessionals and a veterinarian. Two Process Net-Map exercises were conducted in each district to deal with clinical services (endemic diseases), while the other two were conducted to collect information on preventive services (epidemic diseases control). As mentioned earlier, preventive services and control of epidemic diseases are still under the purview of the public sector, while clinical services are to be provided by the private sector. Thus, the type and number of actors involved and the service delivery problems were expected to vary according to the type of service. In addition, two districts with distinct livestock production systems were chosen to capture variations in the institutional setup, and in social and physical factors, which can also influence the performance of animal health delivery systems (Woodford, Reference Woodford2004). District A was selected to represent the pastoral production system, and district B was selected to present the intensive livestock production system. The names of districts are not disclosed to guarantee the anonymity of the participants.
Table 1. Number and type of interviews in the two case study districts.

Source: Authors.
In the context of this paper, the pastoral system is defined as a livestock production system where farmers keep large numbers of animals, mainly of local breeds, for food, cultural and cash purposes (Ruhangawebare, Reference Ruhangawebare2010). The pastoral systems in Uganda are mainly characterized by seasonal movements in search of water and pasture, and are mainly found in the Karamoja and Ankole regions of Uganda (Inangolet et al., Reference Inangolet, Demelash, Oloya, Opuda-Asibo and Skjerve2008; Kugonza et al., Reference Kugonza, Nabasirye, Mpairwe, Hanotte and Okeyo2011). By contrast, the intensive production system is defined here as one where animals are mainly of exotic breeds or crossbred. They are kept predominantly for commercial purposes (Garcia, et al., Reference Garcia, Balikowa, Kiconco, Ndambi and Hemme2008). A few farmers keep local breeds as well in the intensive production system. The types of veterinary service providers in these systems vary, and they include government staff, private veterinarians and paraprofessionals. In the pastoral system, one can find a group of paraprofessionals called Community Animal Health Workers (CAHWs). They usually have three months of non-formal training in animal health management. In the intensive production system, some paraprofessionals were found to have one to two years of training in animal health in formal training institutions, while others have one to two years of formal training in general agriculture, including crop and livestock production.
RESULTS
In the first part of this section, the results for the Process Net-Map exercises for clinical services are presented for both pastoral and intensive livestock production systems. In the second part, the results for the preventive services are presented. The average influence level and its range were computed for each actor and type of service in each district. The results are shown in Table 2.
Table 2. Mean and range of influence scores of actors involved in veterinary service provision.

Source: authors:
The average is computed by summing the ranks from the two groups and dividing the sum by 2. The mean value was rounded to the nearest whole number. The range is the difference between the largest and the lowest actor's influence level in the provision of a particular service in a given production system.
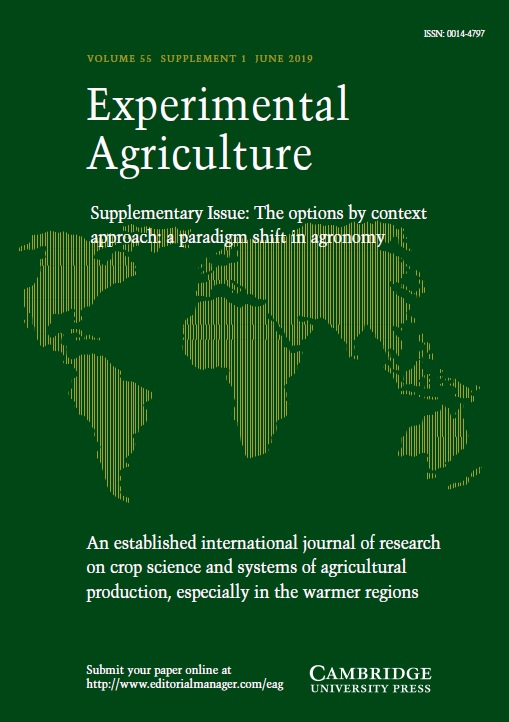
In the pastoral livestock production system, the description of the process of the clinical treatment of endemic diseases presented here is based on interviews with the following respondents: three CAHWs, District Veterinary Officer (DVO), 15 farmers and one animal health assistant for each Net-Map group interview. The respondents identified East Coast Fever (ECF), anaplasmosis, heart water, red water and tryponamiasis as the most common diseases. In the intensive systems, the description of the process of treatment of endemic disease control is based on interviews with the following respondents: government veterinarian, three paravets, two private veterinarians and 10 livestock farmers for each Net-Map group interview. The main endemic livestock diseases identified by these respondents were ECF, anaplasmoisis and tryponamiasis. Using the Process Net-Map tool, a total of nine actors were identified as the main actors in the treatment of endemic diseases in the pastoral system. In the intensive livestock production system, the respective number of actors was seven (see Figures 1a and 1b respectively). According to the interviews, the actors play the following roles in the process:
-
1. Herdsmen
In the pastoral system, the herdsmen are mainly the children of livestock keeping households who have the task to herd animals on a common grazing land. They are the first actors to note that an animal is sick. They typically report this first to their mother and later to their father or head of household. These were ranked as the most influential actors in ensuring that an animal gets treated. They received the average score of eight because they are close to animals and monitor the status of animal on a daily basis. If they fail to recognize or report a sick animal in time, the animal is likely to die. Moreover, they influence decisions made by their parents regarding the sick animal.
As in the case of pastoral areas, the herdsmen in the intensive system observe the sickness and report the cases to livestock owners. In the intensive system, herdsmen are, however, mainly the hired individuals. They were given an average score of five because they are close to the animal and are always able to monitor the situation of animal and report it to the livestock owner. Also, during the follow-up, the service provider interacts mainly with the herdsman rather than with the owner of animals (see Figure 2). The hired herdsmen are seen to be less influential than the herdsmen who are family members because they have less influence on decisions made by livestock owner.
-
2. Livestock owners

Figure 2. Network of actors involved in the treatment, prevention and surveillance of endemic diseases.
When a herdsman in the pastoral system reports a case to his mother, it is a common practice for her to first use local drugs to treat the animal. If the animal does not respond to the treatment, she would usually report the case to her husband. It is an important practice in the pastoral system that households sell small ruminants (typically a goat) to be able to pay for drugs and veterinary services for their cattle. Only the head of the household can authorize the sale of a goat or sell the goat himself to buy drugs. Sometimes, the wife may sell chicken in the local market or use the income from milk to buy drugs for cattle. The respondents noted that the influence of women in livestock keeping households on the outcome of the treatment process mainly stems from the use of traditional medicine and monitoring animal's health status. Together with the herdsmen, women are involved in the milking, and while milking, they closely observe the animals. In addition, because of the polygamous family structure in the pastoral areas of Uganda, the animals are divided among different spouses, and each spouse has her own animals to provide food for her children. Women have a strong incentive to oversee animals’ health status because if an animal dies, it is the woman who suffers most, as she loses an important source of milk and income. Because of these reasons, women in livestock keeping households were ranked to be more influential than men. They received an average score of seven, as shown Figure 1a. The influence of men comes from their role in the mobilization of resources for the treatment of animal. Although the management of animals’ welfare rests with women, men have the authority to decide whether or not to sell a small ruminant to finance the treatment, or to sell the animal itself. Therefore, men received an average score of six. When funds are mobilized, the drugs are bought and self-administered by either the herdsmen or their fathers with the help of their mothers. Rarely do the pastoral livestock keepers seek the services of CAHWs.
In the intensive livestock production system, livestock is kept mainly for commercial purposes. Therefore, any disease outbreak is taken seriously because it threatens the livelihood of livestock owner. When livestock owners receive reports of a sick animal from herdsmen, they always seek the services of a paravet, private veterinarian or a government veterinarian. The respondents identified livestock owners as the most important actors because they are decision makers, control finances and occasionally treat their animals themselves.
-
3. Middlemen
Middlemen were considered to be one of the key actors in pastoral areas and were ranked as more influential than drug shops and CAHWs. They buy animals from livestock keepers. Therefore, they are the source of money used to buy drugs from drug shops, and seek services of CAHWs. In addition, middlemen help farmers to dispose of a sick animal when treatment fails. The middlemen buy sick animals at a lower price than healthy animals, treat them and later resell them at a higher price. Because of these reasons, the middlemen received an average score of six, equal to that of the heads of households in the pastoral system. The challenge arising from the middlemen is that some of the animals are slaughtered and consumed before the waiting period after a treatment is observed. Consumers often eat meat of treated animals that are slaughtered before the mandatory waiting period of seven days, which increases the risk of developing antimicrobial resistance (Kariuki et al., Reference Kariuki, Onsare, Mwituria, Ngetich, Nafula, Karimi, Karimi, Njeruh, Irungu and Mitema2013; McEwen and Fedorka-Cray, Reference McEwen and Fedorka-Cray2002).
Middlemen were not considered as the most important actors in the intensive livestock system, mainly because animals are predominantly kept for dairy products rather than beef, and the breeds kept are exotic or crossbred, which are very valuable. Thus, livestock owners have an incentive to seek the services of qualified service providers rather than to sell sick animals.
-
4. Service providers
In the pastoral system, farmers mainly buy drugs from drug shops and treat their animals themselves. They typically seek the services of CAHWs only when an animal fails to respond. Consequently, drug shops were ranked as more influential than CAHWs with an average score of four, as shown in Figure 1a. In some cases, nongovernmental organizations (NGOs) give drugs to CAHWs, who then offer services to farmers at subsidized rates. If the cases handled by CAHWs fail to respond, then CAHWs who have better education and can speak English will consult a veterinarian. Others give up, and the farmer is forced sell the sick animal. When a government veterinarian is consulted, he may either give advice or visit the site if it is accessible. If the animal still fails to respond, livestock keepers often sell the animal at lower prices, as indicated above.
In the intensive production system, paraprofessionals are the most commonly approached service providers because they are more easily accessible as compared with veterinarians. If the animal is treated by paraprofessionals and fails to respond to the treatment, then paraprofessionals often refer the case mainly to private veterinarians, but in rare cases to government veterinarians. The paraprofessionals were regarded as the second most important actors to livestock owners with an average score of seven because they are available and easily accessible to farmers. Although there were only two active private veterinarians in district B, they were ranked to be more important than government veterinarians, who were eight in total. They received an average score of six compared with government veterinarians, who received an average score of four. The reason indicated for the higher rating of private veterinarians was that they were able to work well with paraprofessionals. In addition, they own drug shops and charge lower fees than the government veterinarians. Paraprofessionals refer cases to private veterinarians and use animal drug shops of private veterinarians as contact point with farmers. They often consult private veterinarians and provide business by referring farmers to them. One private veterinarian commented that ‘we do work with paravets because they create business for us, especially when they refer a farmer to us, but at times our interaction makes paraprofessionals insecure’.
According to the respondents, government veterinarians are perceived to be treating paraprofessionals as subordinates. That is why there is always less interaction between paraprofessionals and veterinarians. Moreover, most of the government veterinarians are working with the National Agricultural Advisory Services (NAADS) programme as coordinators, a position which pays well and takes most of their time. They do not have time to handle cases referred to them, and have no incentives to work closely with paraprofessionals since they have an assured income and do not need to cooperate with paraprofessionals. The law does not mandate government veterinarians to work with paraprofessionals either, or to provide clinical services to farmers as they are supposed to concentrate on preventive services. However, government veterinarians can offer clinical services to farmers on private basis. Most often, government veterinarians pass on cases referred to them to private veterinarians.
The drug shops attendants were considered to be relatively least influential actors, receiving a score of two. Drug shops constitute a link between farmer and service providers. Farmers noted that if an animal is sick, they just have to go to a drug shop and are sure to be able to meet at least one paraprofessional or private veterinarian associated with the shop. If they find a veterinarian in the drug shop, farmers who treat their animals themselves are able to get advice on drug use and general animal health management.
-
5. Nongovernmental organizations
Like middlemen, NGOs are only recognized as influential in pastoral areas. They train and support CAHWs and provide extension services through the so-called ‘pastoral farmer field schools’ (PFS). The main skills disseminated through PFSs are disease control and deworming. One of the farmers stated: ‘The PFS provides us with knowledge on spraying, animal health hygiene and diseases. In our PFS, we have experimented with hand picking of ticks against spraying, and we tested different accaricides; we compared local herbs with the use of modern veterinary medicines; feeding animals using salt grass, which is diluted during the rainy season, with the use of mineral licks made from animal bones and soil’. These experiments were mainly conducted under the supervision of CAHWs. However, the challenge is that most NGO programmes are short-lived and when the projects end, the PFSs also fail to perform. That is why NGOs were only given an influence score of one, as shown in Figure 1a.
Challenges regarding the treatment of endemic diseases
The results from the Process Net-Map exercise revealed a number of key problems involved in the treatment and control of endemic animal diseases in Uganda. These are discussed in detail in the following:
-
1. Delay in reporting of disease cases
Delay in reporting was found to be a main problem in pastoral areas because of the following three reasons: First, livestock keepers prefer local medicine to modern medicine. By the time a case is reported because the animal did not respond to local medicine, the disease has already progressed. Second, even if a farmer wants to buy modern medicine, he usually has to sell a small ruminant to buy drugs, as explained above. Moreover, distance to the market to sell an animal and to buy drugs is very long. The main means of transport are walking or riding a bicycle. Farmers noted that it sometimes takes two to three days of walking to reach the nearest drug shop. Third, as observed by one of the respondents: ‘The pastoralist culture is such that, unless the animal falls down or fails to walk, a livestock farmer will not seek the service of service provider’. This is probably the case because the owners are only convinced that they have failed to handle the case if animal falls down.
-
2. Drug misuse
In the pastoral system, drug misuse occurs because of the following reasons: (1) Farmers tend to treat their animals themselves, yet most of them have no formal education. Farmers are, therefore, not able to read labels on drug and thus are not able to know how to apply the drug correctly. (2) The low level of education of CAHWs as well as language differences limits interaction between CAHWs and veterinarians. As a result, CAHWs often overuse drugs or administer wrong drugs based on incorrect diagnosis. When the animal fails to respond, farmers refuse to pay them for their service, and hence they lose the incentive to seek services of CAHWs. (3) Presence of many drug shops opened by businessmen without animal health qualification is a problem as well. Their objective is simply to sell drugs. They do not advise farmers on the use of drugs, and sometimes they sell expired drugs. There is a so-called ‘Happy Cow’ drug shop owned by the Catholic Church, which is an exception. The personnel running this shop often give advice to farmers on the correct usage of drugs for particular diseases based on the clinical signs of sick animal.
In the intensive system, drug misuse is also common among paraprofessionals and farmers. Following are the reasons for drug misuse among paravets: First, the paraprofessionals are often trained by unaccredited institutes. These institutes do not have the facilities to adequately train paravets, and thus paraprofessionals are ill-equipped. Second, many of the paravets are trained in crop science or general agriculture, but because of the existence of a market for veterinary services, paraprofessionals trained in crop production have joined the veterinary market. Third, paravets are driven by desire to make profits and tend to over- and under-dose animals in order to increase sales and revenues. Over-dosing occurs if paraprofessionals believe that a farmer can afford a larger than the necessary dose, and under-dosing occurs if a farmer is not able or not willing to pay for correct doses. Paraprofessionals then decide to give lower doses equivalent to the fee a farmer is able to pay. One of the veterinarians remarked that ‘paraprofessionals always come up with wrong diagnosis and prescription and overdose the animal. When the animal fails to respond, they come running to us to save their image before the farmer. For example, paravets under-dose goats with albendozole and when the goat fails to respond, they come to us. Then you shift the treatment to trodax, the animal usually gets well. Then you know that the animal has become drug-resistant’. The problem of drug resistance is so severe that most of the paraprofessionals in both pastoral and intensive livestock systems expressed their frustration about animals not responding to treatment. One of the CAHWs said: ‘My son, we have a problem, we treat the animals, but they are not getting better. Is the problem [with] us, or are the drugs not strong enough?’ Similar sentiments were expressed by paraprofessionals with emphasis that the current drugs are weak and not useful anymore. The increase in drug misuse also has significant effects on human health (Bogaard and Stobberingh, Reference Bogaard and Stobberingh2000; Byarugaba, Reference Byarugaba2004; Finch, Reference Finch2003). A recent study in Uganda by Byarugaba et al. (Reference Byarugaba, Kisame and Olet2011) found a high-level resistance against erythromycin, gentamycin and tetracycline in commensal bacteria in food of animal origin. The effects of this problem have increased the number of deaths, complications, additional expenses, prolonged hospital stay and additional toxicity in humans (Collignon, Reference Collignon2012).
-
3. Limited qualified staff
In both production systems, there are relatively few veterinarians and paravets who are properly trained in veterinary medicine. In pastoral areas, the problem is more pronounced. In district A (pastoral area), there was only one veterinarian with a university degree. He is occupied with administrative work and cannot be reached easily. In fact, all farmers who participated in the Process Net-Map exercises stated that they had never met or heard about this veterinary officer. One of the CAHWs remarked: ‘Our problem is that we have only one veterinarian in the district, and he is busy with administrative work, attending workshops. He is always out of station. At times, some of us have to consult him on the phone’. The DVO admitted that it is true that he does not get to the villages and communities because he is the only veterinarian in the district. The veterinarian also cited poor accommodation, lack of transport and security problems. Most areas are not easily accessible and his department does not have a car. Sometimes, it takes him one week from the capital Kampala to reach his work station, either because roads are cut off due to flooding during the rainy season, or because the trip is insecure. Frequently, he delegates government duties to CAHWs. Occasionally he conducts consultations over the phone, but since he does not know the local language, only CAHWs and farmers who are comfortable with English and have phones can consult him over the phone. In the intensive production system, the situation is somewhat better. Still, out of 10 veterinarians available in the district, only two are involved in providing veterinary services.
Actors involved in the treatment and control of epidemic diseases
Results from the Process Net-Map tool in pastoral areas showed that 13 types of actors are involved in the prevention of epidemic diseases in pastoral communities. The key services in the prevention of epidemic diseases are disease surveillance, reporting and vaccination. As in the case of endemic diseases, and as shown in Figure 2a, the herdsmen and their mothers are the first to note a disease and report it to the head of household. If the disease is unfamiliar to them or if they are not able to handle it, they report this to CAHWs. The CAHWs then report the case to government veterinarian (DVO) and the NGOs staff. The government veterinarian in the case study area then reports the case either to a laboratory operated by the Italian Development Cooperation (C&D) or a laboratory operated by the National Animal Disease Diagnostics and Epidemiology Centre (NADDEC). After receiving reports from the veterinarian, C&D staff meets the veterinarian and CAHWs to seek assistance in mobilizing local communities to take samples from sick animals. Samples of blood, stool, skin scrapings and lymph nodes, among others, are then tested at the C&D laboratory, and the results are presented to donor partners and the local governments, which are responsible for the dissemination of results to communities. Sometimes, radio programmes are organized by C&D, and government veterinarians are invited to disseminate the confirmed results to livestock owners.
When the results from the surveillance are available, quarantines are issued by the Commissioner for Livestock Health and Entomology (CLH&E), the local authority in charge, through DVO. Vaccinations are given for the diseases for which vaccines are available. Vaccines for epidemic diseases are usually procured by government, but occasionally NGOs and the Food and Agriculture Organisation (FAO) procure them through the government, as well. The government agency in charge is the MAAIF, which provides vaccines free of charge, but it does not always provide the local government with the logistical support required for conducting vaccination campaigns. The NGOs, therefore, typically come in to provide transport, fuel, training and mobilization of CAHWs and livestock farmers. They register communities, provide the cold chains required for the vaccine and meet the costs for carrying out vaccination campaigns. DVOs perform a coordinating and supervisory role in vaccination, but the actual vaccination is given by CAHWs.
The respondents identified the Ministry of Finance Planning and Economic Development (MFPED) as the most influential actor regarding the treatment of epidemic diseases because it is this ‘Mr. Money’ who was given an average score of eight (see Figure 2). The respondents noted that the main challenge regarding vaccination and surveillance is always the financing of these services. Active surveillance is not always done because of financial limitations. Budgeting and release of financial resources are handled using ‘a fire fighting’ approach. Funds are only released when there is an outbreak, rather than conducting routine vaccinations. The second most influential actors identified by the respondents are NGOs and development partners, such as the FAO and the Italian Cooperation. They received an average score of seven because of their financial power (see Figure 2a). Government veterinarians, commissioner, and the verification team were ranked as important as the NGOs and development partners due to their role in coordinating these activities and in providing technical guidance. The male members of livestock owning families were ranked to be more influential than the CAHWs. They received an average score of six mainly because they help in restraining animals and also control finances in case they are asked to share some of the costs. Moreover, they are the ones who report the outbreak of disease to CAHWs. The CAHWs received an average score of five because they are involved in mobilizing farmers and in conducting the vaccination. Middlemen, drug shop owners, herdsmen and female members of livestock owning households are perceived to be the least influential actors because vaccines are procured by the government, and surveillance and vaccination services are offered by either NGOs, development agencies or the government. The role of female household members and herdsmen is limited to the identification of diseases. Middlemen and drug shop owners play a role in spreading information about the outbreak of diseases.
In the intensive production system, a total of 12 actors were identified as influential regarding the control of outbreak of epidemic diseases. In the case of outbreak of an epidemic disease, such as foot-and-mouth disease (FMD), the livestock owner typically reports the outbreak to paravets or private veterinarians, who then report it to DVO. The latter then reports the outbreak to the CLH&E under MAAIF. After receiving such a report, the CLH&E mobilizes a team from NADDEC to visit the affected district and carry out epidemiological investigations. The team also collects samples for confirmatory diagnosis. The samples collected are tested at the NADDEC laboratory and once the case is confirmed, the team reports the results to CLH&E for the action to be undertaken. Based on the results, quarantine will be instituted by CLH&E as an immediate control measure. This will be followed by a vaccination campaign for diseases for which the vaccines are available. Once the disease has been controlled, the DVO of the affected district is required to officially request the CLH&E to lift the quarantine. The CLH&E usually sends a team from the ministry to take samples to confirm the absence of the disease. Based on the results, the CLH&E issues a letter with the instruction to lift the quarantine.
Although it is the responsibility of the central government to provide vaccination services, farmers often seek vaccination services from private veterinarians, who get the vaccines from private firms like ERAM Limited, Quality Chemicals and other suppliers of pharmaceuticals. In case of a routine vaccination organized by the government, vaccines are provided to paravets and private veterinarians, but the farmers are charged a fee to cover labour and transport costs of service providers. Fees vary depending on the disease. For example, the fee is 1000 UGX (US$ 0.3) for rabies, 1500 UGX (US$ 0.45) for FMD and 2500 UGX (US$ 0.9) for lumpy skin disease. The farmers involved in the exercise noted that all service providers (government veterinarians, private veterinarian and paravets) charge the same price. Vaccination is often done at farmer's home or farm.
Just as in the case of the pastoral system, the respondents in the intensive production system identified the Ministry of Finance to be the most influential actor with regard to the control of epidemic diseases. This ministry received a score of eight, as shown in Figure 2b. The reason is that the Ministry of Finance decides on whether or not funds are to be released. As in the case of pastoral areas, the respondents noted that the challenges regarding vaccination and surveillance always consist in financing these services. Active surveillance is not always done because of financial constraints, and even if a routine vaccination is scheduled, the Ministry of Finance often refuses to release funds until an outbreak occurs. The second most influential actors, who were ranked as important as the DVO, include the CLH&E under MAAIF and the National Surveillance Team. Due to their coordinating role and the technical guidance provided by them, they were given a score of seven. The livestock owners were ranked to be more influential than paravets and private veterinarians because they are close to animals and can easily recognize that an animal is sick. They also report disease to service providers, which on the average result in a score of six. Private veterinarians were ranked to be more influential than paravets/paraprofessionals because they have technical expertise and are linked closely with government veterinarians, who are the more central actors in coordinating the control of epidemic diseases at district and national levels. The private veterinarians were given a score of five, and paravets a score of four, on the average. Herdsmen and drug shop owners were given a score of two each for their role in reporting disease outbreaks (see Figure 2b). Herdsmen were rated to be more influential in the detection of endemic diseases than epidemic diseases because epidemic diseases are highly contagious, spread rapidly and are more easily noticeable than endemic diseases.
Problems in the treatment and control of epidemic diseases
The key challenges identified by the respondents regarding the implementation of disease control services, such as vaccination and quarantine, are discussed in the following:
-
1. Inadequate supply of vaccines and insufficient budgetary allocations
The respondents frequently noted that the vaccines procured for vaccination were not sufficient to vaccinate all animals in the respective region or area. According to the respondents, this problem was caused by inadequate budgetary allocations to preventive service delivery. As a result, some animals are not vaccinated, which later infected other animals. One veterinarian stated that ‘the persistence of FMD in the Teso region in 2010, even after the implementation of the vaccination exercise, was due to inadequate supply of vaccines. Out of the 50,000 units of the vaccine required for vaccination, only 10,000 were availed, rendering the containment of FMD disease difficult’. Since the amount of vaccines supplied is usually insufficient, local governments depend on NGOs to implement successful vaccination campaigns. As remarked by one of the government veterinarians: ‘In the pastoral areas, NGOs are indispensable. If the NGOs pull out, the government's position is very weak. In recent massive vaccination exercises to combat the goat plague and contagious bovine pleurapneumonia (CBPP) in cattle in the Karamoja region, most of the logistical and financial support was provided by NGOs. The government could only contribute the vaccine. The government's NAADS programme does not finance veterinary services, yet livestock is the main agricultural sector in Karamoja’.
As the respondents noted, budgetary allocations from the government are inadequate and unpredictable, limiting the ability of DVOs, verification teams, and other government departments to implement vaccination tasks. When MAAIF procures vaccines, it is expected to provide logistical support to the local government staff for the implementation of vaccination campaigns. However, MAAIF does not provide such logistical support and therefore the government veterinarians are compelled to charge farmers for each animal vaccinated to recover such costs. The advantage in the intensive production system is that farmers are able to pay for these services. Even though government veterinarians pass on the vaccines to private veterinarians, the latter are able to recover their costs by using them.
The respondents identified other governance issues as well. In particular, they noted that veterinarians also ‘capture’ funds meant for paying paraprofessionals, including CAHWs. The respondents observed that some veterinarians are corrupt and embezzle funds that are allocated for particular activity. They mobilize paraprofessionals to carry out the work, but later refuse to pay them, or pay a fee that is lower than what they are supposed to pay. This results in a poor response of CAHWs to vaccination exercises. This problem also creates a poor working relationship between veterinarians and CAHWs.
More generally, the respondents also noted that budgetary allocations to animal health and entomology are often low and unpredictable. This observation is supported by findings from a study of the Economic Policy and Research Center (EPRC), which revealed that the funds received for animal health services are less than the allocated funds. Moreover, the allocated funds are less than the originally budgeted total expenditure (Economic Policy and Research Center, 2009).
-
2. Political interference
The second problem identified by the respondents is local political interference, mainly in the implementation of quarantine services. The respondents noted that when quarantines are instituted, veterinarians often cannot enforce them. When livestock markets are closed, the politicians typically make ‘a lot of noise’ and some of them lift the quarantine on their own, without seeking approval from MAAIF. In one district, it was reported that local politicians sent veterinary officer on forced leave so that they were able to lift the quarantine. The main reasons why politicians lift quarantines are to avoid loss in revenue that would be generated when livestock markets are open. Moreover, quarantines are unpopular among livestock keepers and traders, therefore politicians have incentives to lift quarantines to avoid political losses or gain political support. Farmers want to sell livestock for school fees and other needs. The implementation of quarantine is therefore perceived to affect farmers’ welfare and it is seen as a sign of failure of politicians to provide services. To avoid political fallout, politicians have therefore incentives to lift quarantines. Apparently, the need for quarantines is not well understood. Moreover, as argued by Leonard (Reference Leonard1993) and Otte et al. (Reference Otte, Nugent and Mcleod2004), there is a coordination failure and a collective action problem with regard to quarantines because incentives and interests differ at farm or community level and at the decentralized government level. At the farm or community level, quarantines do not offer benefits to farmers or communities whose herds are being quarantined but rather deny them access to markets with better prices. Thus, they have no incentive in adhering to quarantines (Leonard, Reference Leonard1993). At the local government level, one of the respondents stated: ‘One challenge in implementing quarantines is that local governments have different priorities. When quarantine is issued in one local government, the neighbouring local government may not be willing to issue quarantine for fear of losing revenues from animal markets. Therefore, the disease (FMD) persists for a long time. This was the case in the Teso region’.
Following is the challenge that arises: Who should enforce quarantine? Even state intervention by the central government, as suggested by Leonard (Reference Leonard1993), is ineffective, since it needs to be enforced locally. As noted by the respondents, state intervention is ineffective for two reasons: (1) Markets with better prices are available during quarantine periods because of the failure of local governments to jointly implement quarantines. (2) The police, who are supposed to control movements, are easily bribed by traders who transport animals at night. Also, the respondents indicated that there is uncertainty on when quarantine will be lifted, which is also the reason why quarantines are not obeyed. One of the elders stated that ‘in previous times, quarantines would be issued and animals were vaccinated, and in three to four months the quarantines are lifted. But today it takes one to two years’.
-
3. Poor relations between government veterinarians and paraprofessionals
This was particularly a main problem in the intensive production system. Paraprofessionals rarely report disease outbreaks to government veterinarians even though this is mandated by the Animal Diseases Act of 1964 and its revised edition of 2005Footnote 1 . This Act regulates the prevention, control and eradication of animal diseases and requires that all outbreaks of epidemic animal diseases are to be reported to the nearest veterinary authority, who should in turn report the outbreak to CLH&E within 24–48 hours using the fastest means of communication. The relationship between paravet and government veterinarians is poor because government veterinarians perceive paravets as subordinates who are less qualified. Therefore, they tend not to cooperate with paravets when consulted. In addition, government veterinarians have no incentive to build good professional relationships with paravets since they have an assured government salary. Moreover, the Veterinary Surgeons Act is outdated and ineffective with regard to the strengthening of relations between veterinarians and paravets. The DVOs, therefore, only depend on reports from private veterinarians. The relationship between paravets and private veterinarians is good because paravets often consult them and consider them as colleagues irrespective of the level of training. This is mainly the case because private veterinarians need to generate sufficient business to prosper, and it is through networks with paravets that they get new clients.
-
4. Poor management of government veterinarians
A serious problem identified by the respondents is poor personnel management. One important personnel management problem is limited opportunities of promotion at the local government level. These opportunities are limited because of the following reasons: Opportunities for promotion depend on the availability of funds, and these are influenced by local politicians. Merit and academic qualification is not given priority as long as the applicant has a bachelor's degree in veterinary medicine. Veterinarians noted that it is common in Uganda to find a DVO with a bachelor's degree, while his subordinates (veterinary officers) have master's degrees. This has created challenges in the supervision of veterinarians by DVO. As a consequence, most DVOs do not assign duties to their subordinates and the latter are often absent from their duty stations. One of the government veterinarians stated: ‘I left my district to come to offer private services in another district because I have a master's degree and my boss has a bachelor's degree in veterinary medicine. He does not assign me any responsibilities. So I decided to make myself productive. I get a government salary for free, I am in good terms with my boss and my business is doing well’. One of the interviewed veterinarians pointed to another management problem: ‘Performance-based assessments are only done in Uganda if you are involved in opposition politics’.
-
5. Policy inconsistency
The creation of autonomous institutions such as the NAADS, which have their own governance structure, has resulted in the duplication of responsibilities and in a lack of clear lines of accountability. The NAADS programme was established by an act of parliament, the NAADS Act of 2001Footnote 2 , to spearhead the transformation of extension services from a public sector supply-driven model to a private sector demand-driven approach. Under NAADS, local governments have to hire NAADs staff on the one hand, and MAAIF staff for advisory services on both crop and livestock, on the other. These staff members perform the same tasks, but NAADS staff receives higher salaries and has more access to resources to perform their work. A NAADS staff member is paid 400 Euros per month, as compared to an ordinary worker under the local government, who receives only 135 Euros. This situation has undermined the traditional public service system because NAADS is running a parallel system, even though it is also under the central government, in particular under MAAIF. Also, under the decentralized governance system, technical and financial lines of management are separated because DVOs have to report to both the MAAIF for technical matters and the Ministry of Local Government and the district local government for administrative matters. This system has destroyed the chain of command from the center to the district, which is a key to animal disease control (Food and Agriculture Organisation, Reference Nick Honhold, Douglas and Arnon Shimshoni2011; World Organisation for Animal Health (OIE), 2011).
In this vein, one respondent stated that ‘decentralization and NAADs have broken the chain of command. Disease reporting and quarantine implementation has become problematic. The DVO reports to the chief administrative officer (the administrative head of district administration), who is head of all civil servants in the district. The DVO also reports to the district council and to political heads who are locally elected leaders. However, the DVO has no incentive to report disease cases to the central ministry. In fact, DVOs feel restrained from reporting the outbreak of certain disease because the local government officials would fire them or suspend them from office’. Another respondent noted the case of a district where the veterinarian was sent on forced leave to pave way for lifting quarantine. If quarantines are issued, politicians can indeed suspend veterinarians to lift quarantines because due to decentralization, veterinarians are appointed by the District Service Commission. Therefore, veterinarians need to serve the interests of local government leaders and cannot follow the technical leaders at MAAIF.
-
6. Exclusion of technical expertise in programme planning
Another problem cited by the respondents relates to planning and implementation of animal health programmes. The respondents noted that ‘the technical leaders of the department of Livestock Health and Entomology under MAAIF take only the third position in decision-making. Major decisions and policies are made in planning committees comprising economists and accountants without the technical expertise of the staff, who then have to implement the animal health programmes’. Most of the respondents cited the example of the so-called ‘Non-Agricultural Technology and Agribusiness Advisory ServicesFootnote 3 project (Non-ATAAS). In this programme, the provision of agriculture is planned based on commodities. The programme is a part of MAAIF's Agricultural Development and Investment Plan (DSIP), 2010/2011–2014/2015, which has the objective to pursue private sector-led and market-oriented agricultural development through a commodity approach (Ministry of Agriculture, Animal Industry and Fisheries, 2012). According to the respondents, the design of this project does not reflect the implementation structure of the ministry, and thus cannot be effectively implemented. The problem of exclusion of technical staff from MAAIF in agricultural policy reform is discussed in detail by Kjær and Joughin (Reference Kjær and Joughin2012), and has led to a lack of ownership of reforms and the development of inadequate implementation strategies (Bahiigwa et al., Reference Bahiigwa, Rigby and Woodhouse2005; Kjær and Joughin, Reference Kjær and Joughin2012).
SYNTHESIS, DISCUSSION AND POLICY RECOMMENDATIONS
Synthesis
The study has identified a number of actors who are involved in the delivery of veterinary services in Uganda. The number and type of actor depends on the type of service and production system. As the study has shown, CAHWs and NGOs/development agencies are involved in both curative and preventive services in the pastoral system, but not in the intensive production system. The main influence of NGOs and development agencies in pastoral communities is in the provision of preventive services. The study indicates that the influence of each actor depends on the following factors, irrespective of the type of service and production system:
-
1. Control of financial resources.
-
2. Closeness to animal.
-
3. Education level and availability of service provider.
-
4. Ability of veterinarians to communicate with paravets and farmers.
-
5. Relationship between paraprofessionals and veterinarians.
Table 3 shows the relationship between service type and production system and veterinary service delivery problems. Sign ☹ indicates that for that particular service in a given production system the problem is prevalent, and sign ☹☹ means that the problem is very severe.
Table 3. Service delivery problems by service type and production system.

Source: authors.
Clinical services: As shown in Table 3, drug abuse, delays in reporting, staffing problem and government staff absenteeism are the prevalent problems in pastoral communities. Low staffing levels and absenteeism of government veterinarians can mainly be attributed to poor infrastructure in pastoral areas. Also, language barriers between the veterinarians and CAHWs, as well as between veterinarians and farmers, were found to be a severe problem affecting the delivery of curative services in pastoral communities. In the intensive production system, the most important problems in the delivery of clinical veterinary services were drug misuse, personnel management issues and poor relations between paravets and veterinarians.
Preventive services: In the case of preventive services, delayed reporting of epidemic animal diseases, capture of resources by veterinarians, especially during vaccination exercises, political interference, especially in quarantines, and insufficient and unpredictable budgetary allocations were found to be the most important problems in both pastoral and intensive systems. Absence of good cooperation between paravets and veterinarians was considered to be a prevalent problem in the intensive livestock production system. Exclusion of veterinarians in decision-making at the ministry level was also found to be a major challenge for the delivery of preventive services.
Discussion and policy options
The emerging picture from this study is that challenges of veterinary service delivery in Uganda are linked to institutional pluralism in service delivery, decentralization and budgetary constraints, which limit the effectiveness of the existing institutions. Consequently, given the fiscal challenges, the key to improving animal service delivery in Uganda rests on getting priorities, policies and institutions right to make animal health services work. Creating an independent ministry responsible for livestock might be advantageous in advocating for better veterinary policy, legislation and education. Countries such as Tanzania and Kenya, which have – or had – independent ministries of livestock, managed to put in place a veterinary legislation that guides the provision of veterinary services. For example, Tanzania passed a Veterinary Act in 2003Footnote 4 , and Kenya in 2010Footnote 5 , but Uganda still depends on the Veterinary Surgeons Act of 1958Footnote 6 . Uganda too used to have an independent ministry of livestock industry and fisheries before 1992, but it was merged with the ministry of agriculture with the objective of rationalizing the use of public funds (Kuteesa et al., Reference Kuteesa, Magona, Wanyera and Wokadala2006).
However, this merger turned out to be counterproductive and has negatively affected the delivery of agricultural services, including veterinary services (Semana, Reference Semana2002). A number of other autonomous institutions, such as the National Agricultural Research Organization (NARO), NAADS (2001) and the Dairy Development Authority (DDA), were created to improve the delivery of agricultural service, including livestock (Lukwago, Reference Lukwago2010). However, the creation of these autonomous organizations instead increased public expenditure, and service delivery got stagnated or continued to decline.The programmes implemented by some of these organizations, such as NAADS, could be implemented by the public extension system instead of running parallel systems performing the same functions (Rwamigisa, Reference Rwamigisa2013). This could reduce the budgetary problems and the rivalry that exists between MAAIF and some of these institutions. In addition, it is important to ensure that the budget for disease control is released to MAAIF to ensure that routine vaccinations can be conducted. As argued by Morton (Reference Morton2007), vaccination campaigns are important in promoting animal health by preventing outbreaks of contagious diseases such as FMD, thus reducing the need for quarantines, which are, according to our results, even harder to enforce. Moreover, the findings from the EPRC (2009) study cited above show that the main problem is the limited allocation and delayed release of funds. Provision of services by private sector suffers from a collective action failure, as some livestock farmers prefer to be free-rider, since the benefits of vaccination will accrue to all (Leonard, Reference Leonard1993; Otte et al., Reference Otte, Nugent and Mcleod2004). One solution might be the provision of vaccines by the government, whereby farmers are asked to pay for the labour of service providers administering vaccines. De factor, this is already happening to some extent. Another challenge regarding the provision of veterinary services identified by this study is the limited number of active veterinary professionals and difficulty in attracting and retaining veterinary staff, especially by local governments in marginal areas.
This paper proposes three strategies to ensure the availability of sufficient qualified veterinary staff in Uganda: First, re-centralizing the management of veterinary staff. Administrative decentralization was aimed at empowering farmers and local leaders to supervise and monitor the extension staff. The findings of this study show that this is not appropriate for veterinary services because these services require an efficient chain of command to ensure quality and avoid political capture. As the results show, local leaders and farmers do not appreciate the importance of quarantines, and government veterinarians have divided loyalty. They are inclined to listen to local leaders who have political incentives to avoid quarantines. Veterinarians are not able to prevent this against their better professional judgment if they want to save their jobs. This finding suggests that decentralized administration of veterinary staff interrupts the chain of command and reduces the responsiveness of veterinary system, a finding that is in line with the literature (Petitclerc, Reference Petitclerc2012).
Second, there is a need to recruit at sub-county level staff with adequate formal training in veterinary sciences, such as diploma holders, rather than restricting such positions to degree holders with university training. Veterinarians with this level of training are difficult to retain and motivate, especially in pastoral areas with limited infrastructure. Moreover, they require higher wages as compared to paraprofessionals, who hold diplomas in veterinary medicine (see also Leonard et al., Reference Leonard, Koma, Ly and Woods1999). The study indicates that there are limitations to rely solely on CAHWs with low levels of training, who had, so far, been promoted as the only alternative service providers in pastoral areas.
The third strategy is supporting veterinary training and education. Without appropriate funding for this cause, it is impossible to have enough qualified veterinary staff with both diploma and degree to offer veterinary services in all the regions of Uganda. Funding of veterinary education also needs to specifically target students from pastoral areas. This target group is more likely to stay in pastoral areas after completing their education, and they can also resole the language problem. What would be needed is a government scholarship similar to the scholarships fund of the Ministry of Health aimed at training medical personnel from priority areas that are hard to reachFootnote 7 . Such a scholarship fund would be very beneficial for improving animal health services. As argued by Bellemain and Coppalle (Reference Bellemain and Coppalle2009) and Fanning et al. (Reference Fanning, Whyte and O’Mahony2009), veterinary education is a key to improving governance of veterinary services and reducing animal diseases and health risks.
CONCLUSIONS
The study has shown that multiple actors play a role in the delivery of veterinary services in Uganda. They have different levels of influence on the outcome of service delivery. The study also identified a range of governance challenges in provision of veterinary services, which vary according to region and type of service. The results indicate that the influence of actors depends on their closeness to animals, their ability to control financial resources, their education level and the availability of service providers in the respective production system. In pastoral areas, a major problem in the provision of clinical services was the inability of veterinarians to understand the local language. The main problems in the delivery of disease prevention measures, such as vaccination and quarantines, included financial constraints, political interference, poor legal environment, low staff levels, staff absenteeism, delayed reporting and capture of resources provided by the government. These problems have been exacerbated by decentralization, since local governments seem to be more prone to political pressure, e.g. for lifting quarantines. In addition, the exclusion of technical staff from the decision-making process has greatly affected the provision of veterinary services. To improve veterinary service provision in Uganda, the government needs to get its policies right. The governance structures need to address the above-identified governance challenges. In particular, the government needs to realign NAADS programme within ministry structures to avoid duplication of tasks and improve personnel management, strengthen the veterinary legislation to support veterinarians and their relations with paraprofessionals and invest in veterinary education and training for both veterinarians and paraprofessionals. In addition, the government should reconsider the policy of hiring only veterinarians with university degrees at lower levels of government. Last, but not least, there is a need to create more opportunities for candidates from pastoral areas to become paravets and veterinarians so that they can help to overcome the specific challenges of animal health service provisions in their home regions.
Acknowledgments
This research was funded by the Fiat Panis Foundation and the PhD scholarship program of the Food Security Center at the University of Hohenheim. This program is supported by German Academic Exchange Service (DAAD) and the German Federal Ministry for Economic Cooperation and Development (BMZ). We would like to thank all respondents for generously offering their time to participate in the interviews and in the Process Net-Map exercises. We would also like to thank anonymous reviewers for their insightful and constructive comments.






