Introduction
The definition of violence varies across cultural contexts. For example, what is understood to be violence today has no exact equivalent in medieval Norse law (Jansson, Reference Jansson, Österberg and Cronberg2006: 146). This concept involves a range of social behaviours that are intended to cause physical, psychological, sexual, or emotional harm and can be self-directed, interpersonal, or collective (Martin & Harrod, Reference Martin and Harrod2015). In this article, the discussion is limited to interpersonal physical violence in northern Europe during the Middle Ages.
Based on written sources, Pinker (Reference Pinker2011) suggests that violence has decreased over time. Scandinavia in general is considered to have been more violent in medieval and early modern times than today (Lindström, Reference Lindström, Body-Gendrot and Spierenburg2008). Representative homicide rates in Europe fell from 20–40 killings per 100,000 during the late Middle Ages (thirteenth–fifteenth centuries) to only 0.5–1 killing per 100,000 by the mid-twentieth century (Lindström, Reference Lindström, Body-Gendrot and Spierenburg2008). In Scandinavia, a major decline in homicides took place in the seventeenth century (Eisner, Reference Eisner2001). Lesser violence, such as assaults, was even more common than homicide in late medieval Sweden (Österberg & Lindström, Reference Österberg and Lindström1988: 153; Ekholst, Reference Ekholst2014: 108).
What are considered to be socially acceptable uses of violence are context-specific and highly variable (Brickley & Smith, Reference Brickley and Smith2006). In medieval Nordic society, there was a normative acceptance of violence as a way to solve conflicts and define gender and social status (Ekholst, Reference Ekholst2014: 77–78). The master and mistress of a household were expected to beat children and servants to discipline them, but in moderation, not to the extent that a victim would ‘turn blue or bloody’ (Ekholst, Reference Ekholst2014: 104). In monastic houses, corporal punishment was practised. Administered in the right spirit, it was considered an act of love, aiding the development of humility and obedience. The sufferings of the body were part of penance, leading to spiritual purity (Smith, Reference Smith2009). Violence in defence of self, kinswomen, property, and personal honour was also socially accepted (Clark, Reference Clark2012: 123). Honour was of the utmost importance, as a man without honour was unable to participate fully in social and economic life (Lindström, Reference Lindström, Body-Gendrot and Spierenburg2008). In feuds, verbal insults and violence were used as means to resolve conflicts and restore honour (Þorláksson, Reference Þorláksson and Opsahl2007). From the eleventh century onwards, monarchs with growing power in the Nordic countries attempted to limit this private settling of conflicts, but private feuding continued throughout the Middle Ages (Þorláksson, Reference Þorláksson and Opsahl2007). Those involved in violent acts were usually socially well-established and able to pay fines or reach settlements (Lindström, Reference Lindström, Body-Gendrot and Spierenburg2008).
Though medieval women practised violence, exposure to violence and access to weapons were closely associated with men (for a brief review of contemporary weapons and military organization, see Supplementary Material S1), and the use of violence played a prominent role in masculinity in medieval northern Europe in general (Liliequist, Reference Liliequist and Berggren1999). Previous studies on skeletal collections from medieval Scandinavia have shown that weapon-related trauma (WRT hereafter) was primarily associated with men (Arcini, Reference Arcini1999; Sellevold, Reference Sellevold2001; Mollerup, Reference Mollerup, Gregersen and Jensen2003; Kjellström, Reference Kjellström, Regner, von Heijne, Kitzler Åhfledt and Kjellström2009; Milner et al., Reference Milner, Boldsen, Weise, Lauritsen and Freund2015). In early medieval Sigtuna, for instance, 7.1 per cent of men and 2.8 per cent of women were affected by trauma associated with interpersonal violence (Kjellström, Reference Kjellström, Smith and Knüsel2014: table 13.2). While gender differences are important, differences have also been found between groups of men. In the cemetery of Hamar Cathedral (Norway), 8.3 per cent of males displayed WRT. Most of them were tall and buried in prestigious areas, and hence they have been interpreted as noblemen, possibly the bishop's troops or bodyguards (Sellevold, Reference Sellevold2001: 210–11). In the Cistercian monastery of Øm (Denmark), 5.7 per cent of males had cranial sharp-force trauma (SFT) or blunt-force trauma (BFT) (Mollerup, Reference Mollerup, Gregersen and Jensen2003: 162). Again, WRT was associated with high-status male warriors such as knights and squires (Mollerup, Reference Mollerup, Gregersen and Jensen2003: 162). In the Augustinian monastery of Æbelholt (Denmark), 11.2 per cent of male crania had lesions mostly caused by violence, most frequently among males buried in the church and interpreted as warriors (Møller-Christensen, Reference Møller-Christensen1982: 217–18). In the Gilbertine priory of St Andrew in York in England, 19.2 per cent of males buried in high-status areas had perimortem WRT, in contrast to 2−7.6 per cent among other groups of males (Sullivan, Reference Sullivan2004). The association of WRT with males of high social status interpreted as warriors is thus a recurring pattern.
There are also examples of clerics with WRT, e.g. one male with perimortem WRT among the canons of St Andrew's priory, York (Sullivan, Reference Sullivan2004). Males with WRT were also identified in low-status groups in Æbelholt (Mollerup, Reference Mollerup, Gregersen and Jensen2003), Øm (Møller-Christensen, Reference Møller-Christensen1982), Hamar Cathedral (Sellevold, Reference Sellevold2001), and York, St Andrew (Sullivan, Reference Sullivan2004). In a study comparing six sites in medieval London, Krakowka (Reference Krakowka2017) found that violent trauma to the cranium was more common among males of lower social status. This is consistent with studies in England and the Nordic countries showing that the lower classes in large cities were frequently involved in violence, while in smaller towns and rural areas those of high and middle social standing were more exposed (Ylikangas, Reference Ylikangas and Lappalainened1998: 25). These results suggest that not only gender but also status and social context must be considered when explaining patterns of WRT.
The osteological analysis of skeletal assemblages from two Nordic medieval monastic sites, Skriðuklaustur in Iceland and Västerås in Sweden, provides an opportunity to study patterns of violence. Both religious houses belonged to mendicant orders (Augustinian and Dominican, respectively), and their cemeteries have been fully or almost completely excavated. These different settings complement each other. The aims of this study were: 1) to identify patterns of WRT in relation to sex, age, socio-economic, and religious status; 2) to investigate how different groups of men used interpersonal violence to enact masculinity. The hypothesis was that the different ideas about the use of violence identified in previous research on medieval masculinities (see below) would be reflected in varying frequencies of WRT among groups of men.
Medieval Masculinities and Violence
The concept of masculinity is used to refer to qualities associated with men. Although not necessarily a trait of all or even the majority of men, or exclusively a male attribute, these qualities are still perceived as masculine (Connell, Reference Connell1995). Masculinity is not essential or absolute; it is context specific, varies among societies, and changes over time. There can be a great diversity of masculinities within a society, but the concept might lack relevance altogether in other contexts (Alberti, Reference Alberti and Nelson2006): for example, medieval Europe had no exact equivalent for the modern term masculinity (Fletcher, Reference Fletcher, Arnold and Brady2011). Yet, scholars have found that, used with caution, the concept of masculinity can be a useful analytical tool for studying medieval gender relations (e.g. Hadley, Reference Hadley1998; Karras, Reference Karras2003; Lees et al., Reference Lees, Fenster and McNamara1994; Thibodeaux, Reference Thibodeaux2010). In her classic work, Masculinities, Connell (Reference Connell1995) defined masculinity as a configuration of practices. In this sense, masculinity is not merely an identity or a role but something one does. In enacting masculinity, the male body often plays a prominent role and can be used to gain status (Coles, Reference Coles2009; Shilling, Reference Shilling2016). Understanding masculinity as performed and stressing the importance of the body can usefully inform an osteological study. The body is plastic, and at least some activities and habits leave traces in the skeleton, potentially allowing us to identify gendered practices through osteological analysis (Sofaer, Reference Sofaer2006). Interpersonal violence is one such practice associated with the enactment of medieval masculinities and, in some cases, it can be identified in skeletal material.
Physical strength and courage were central to the masculinity of medieval northern Europe, and the ability to defend oneself and one's dependents had great importance (Liliequist, Reference Liliequist and Berggren1999), but different ideals of behaviour and diverse ideas of masculinity applied to different groups of men (Karras, Reference Karras2003). Violence was crucial to the masculinity of the lay elite but had to be practised in a controlled manner (Karras, Reference Karras2003: 163). Although not always followed, rules governed acceptable aggression, and a chivalric code of knightly behaviour existed. Chivalry was not opposed to violence; indeed, violence was vital to it. Elite warriors interpreted their violent way of life and dominance in society as the will of God and viewed their capacity for violence as a divine gift essential to their masculinity (Kaeuper, Reference Kaeuper2001: 50, 143). Hence, the concepts of social status, masculinity, and violence intersect. Ideas about personal honour, for instance, were deeply rooted in the aristocracy of sixteenth-century Europe and were considered to distinguish nobles from commoners. Feuding and participation in conflicts were, however, not reserved for the elite. Wealthy farmers often engaged in violence and conflicts and led riots and rebellions (Koskinen, Reference Koskinen and Koskinen2016). Violence, of course, was also central to the identity of men such as mercenaries who practised it professionally. In Sweden, landowning farmers and townspeople were expected to own weapons and be prepared to use them to defend the realm. These men were not full-time, professional warriors but were mobilized when needed (Neuding Skoog, Reference Neuding Skoog2018: 351–52, 360; see Supplementary Material S1).
Violence was more problematic in the clerical world. Self-control and non-violence were ideals for the medieval clergy, who nevertheless sometimes committed violent acts. Karras (Reference Karras2003: 161) suggested that this behaviour was an acceptance of lay masculine ideals or possibly a lack of self-control. Records from medieval Iceland show that clerics could be both aggressors and victims of violence even in the late medieval period, though the number of clerics who met a violent end decreased in the thirteenth century (Sigurdson, Reference Sigurdson2016: 136–46). For example, at the Dominican priory of Västerås, Brother Johannis Petri sought absolution at the Apostolic Penitentiary for killing a man in self-defence in 1500 (Risberg & Salonen, Reference Risberg and Salonen2008: 389). Monks saw themselves as spiritual warriors with the same virtues as knights, including loyalty, bravery, and physical endurance, and the clergy's spiritual labour was described in martial metaphors of leading battles against the material world, the Devil, and the desires of the flesh (Thibodeaux, Reference Thibodeaux2006 Smith, Reference Smith2011). Conversely, knights saw their martial lifestyle as a form of constant penance, and chivalry as a road to salvation (Keen, Reference Keen1984: 14; Kaeuper, Reference Kaeuper2001: 50).
Hybrid forms of warrior and clerical masculinities also emerged. In the Nordic countries, it was not unusual for bishops to fight in battles, an activity their contemporaries generally accepted (Waśko, Reference Waśko, Kotecki, Maciejewski and Ott2018: 475, 481). The military orders combined war and pilgrimage. For the success of crusades, humility, devotion, and chastity were required and were just as essential as bravery and prowess on the battlefield (Holt, Reference Holt and Thibodeaux2010: 197). In addition, many men lived their early life as warriors before joining religious orders (Smith, Reference Smith2011). At least ideally, this transition entailed a change in the way masculinity was performed. Violence thus had a more ambiguous status in clerical than lay masculinities but was not an unfamiliar phenomenon.
The Assemblages Examined
Human skeletal remains from two monastic sites, Skriðuklaustur in Iceland and Västerås in Sweden, were examined (Figures 1−2). Inclusion in the sample studied required bone preserved well enough for age and sex estimation. Consequently, the following groups were excluded:
(1) Children and adolescents with undeveloped secondary sex characteristics
(2) Individuals with poor bone preservation or representation
(3) Comingled remains.

Figure 1. Map of the Nordic countries with locations of Skriðuklaustur and Västerås.
Figure 2. Plans of the burials at Skriðuklaustur and Västerås. Skriðuklaustur: grey outline: graves not included in the study; black outline: graves included in the study; solid black: graves with WRT. Västerås: general plan (locations of individual graves only identified in Area A but not marked on the plan).


The Augustinian monastery of Skriðuklaustur dates to ad 1493−1554. It was founded in a rural area in eastern Iceland, c. 150 m from the farm at Skriða, and functioned as a hospital and guesthouse. The entire site was excavated between 2002 and 2012, revealing 298 graves (Kristjánsdóttir, Reference Kristjánsdóttir2015). The buried population included about 150 patients of the hospital, 130 laypeople and up to twenty benefactors and brethren (Kristjánsdóttir, Reference Kristjánsdóttir2015). These groups were buried in different areas and were identified from archaeological and osteological findings (Kristjánsdóttir, Reference Kristjánsdóttir2012). In this study, 128 individuals met the inclusion criteria.
Medieval Västerås was a bishop's seat and a harbour town by Lake Mälaren in Sweden. The Dominican priory dates to ad 1244−1528. The population buried there included members of the religious community and laypeople, both local and non-local (Ahlin Sundman, Reference Ahlin Sundman2018). The priory was excavated in the 1950s, partly by non-professionals, and some of the documentation is limited (Folin, Reference Folin1985; Lundberg, personal communication). Assuming similarities between comparable sites, the church and cloister (Areas A−D in Figure 2) were interpreted as areas of higher social status than the cemetery (Area E; for a discussion, see Ahlin Sundman, Reference Ahlin Sundman2018, with references). Friars were expected to be buried separately (Gilchrist & Sloane, Reference Gilchrist and Sloane2005), but their burial sites have not been identified. The number of excavated graves has been estimated to be more than 2000 (Folin, Reference Folin1985), but many were intermingled; only 342 met the criteria for inclusion in this study.
Methods
Sex and age
Standard osteological methods were used to analyse the material. Sex estimations were based on the morphology of the pelvis and cranium (Phenice, Reference Phenice1969; Buikstra et al., Reference Buikstra, Ubelaker, Aftandilian and Haas1994; Bruzek, Reference Bruzek2002). Age estimations were based on the pubic symphysis (Brooks & Suchey, Reference Brooks and Suchey1990), auricular surface of the iliac bone (Lovejoy et al., Reference Lovejoy, Meindl, Mensforth and Pryzbeck1985), cranial suture closure (Meindl & Lovejoy, Reference Meindl and Lovejoy1985), fusion of epiphyses (Scheuer & Black, Reference Scheuer and Black2000), dental development (Moorrees et al., Reference Moorrees, Fanning and Hunt1963a, Reference Moorrees, Fanning and Hunt1963b; Ubelaker, Reference Ubelaker1989), and attrition (Brothwell, Reference Brothwell1981). The following age categories were used: adolescents 12−20 years old; young adults 20−35 years old; middle adults 35−50 years old; and old adults 50+ years old.
Trauma and violence
Fractures result in partial or complete discontinuity of a bone (Ortner, Reference Ortner2003: 120). They may be caused by direct and indirect trauma or be secondary results of pathologies (Lovell, Reference Lovell1997). Consequently, only fractures interpreted as WRT (i.e. direct trauma to the bone intentionally caused by external force) are discussed here.
Antemortem trauma occurs before the time of death and can be distinguished by signs of bone remodelling due to healing or secondary inflammation. Perimortem trauma occurs in fresh bone around the time of death, and no bone remodelling can be observed (Lovell, Reference Lovell1997; Sauer, Reference Sauer, Bass and Reichs1998). To distinguish perimortem trauma from postmortem damage, the fracturing pattern, fracture surface characteristics, and colour of the bone surface were used (Sauer, Reference Sauer, Bass and Reichs1998; Boylston, Reference Boylston, Cox and Mays2006). Weapon-related trauma was classified as BFT or SFT. For BFT, the following criteria were used: an impact site with radiating fracture lines, often in combination with concentric fractures; bevelling on the inner aspect; and bone fragments still attached to one another. When healed or in the process of healing, a depression of the outer (and, in more severe cases, also the inner) tablet could also be observed (Sauer, Reference Sauer, Bass and Reichs1998; Boylston, Reference Boylston, Cox and Mays2006; Krakowka, Reference Krakowka2017). SFT has a well-defined linear cut; a flat, smooth, polished kerf wall, sometimes showing striae; an opposite surface showing flaking and roughening; and possibly associated radiating fractures with fresh bone characteristics (Novak, Reference Novak, Fiorato, Boylston and Knüsel2000; Boylston, Reference Boylston, Cox and Mays2006). When healed, the lesion appears as a linear trauma with rounded edges or a long, depressed gutter fracture (Boylston, Reference Boylston, Cox and Mays2006).
Determining whether trauma was caused by intentional violence or accident is challenging and sometimes impossible. In this study, SFT, facial fractures, and BFT above the hat brim line were interpreted as caused by violence and discussed along with WRT, although other causes cannot be ruled out (Guyomarc'h et al., Reference Guyomarc'h, Campagna-Vaillancourt, Kremer and Sauvageau2010; Krakowka, Reference Krakowka2017). For example, nasal fractures are often caused by accidents, and whether to include them in studies of WRT has been the subject of discussion (Brickley & Smith, Reference Brickley and Smith2006; Redfern, Reference Redfern2017a, Reference Redfern2017b: 81). Postcranial fractures have also been recorded and, although they may be caused by violence (Brickley & Smith, Reference Brickley and Smith2006; Waldron, Reference Waldron2009; Milner et al., Reference Milner, Boldsen, Weise, Lauritsen and Freund2015), they are not discussed further here, as it is difficult to determine the cause of injury in individual cases. Analyses of WRT often identify the victim rather than the perpetrator, though certain injuries such as metacarpal fractures are associated with committing acts of violence (Brickley & Smith, Reference Brickley and Smith2006; Waldron, Reference Waldron2009: 151). Moreover, the victims of interpersonal violence often engage in violent situations as perpetrators.
Trauma was identified by visual inspection of cleaned bones. For each lesion, location (affected element and side), size, and characteristics were recorded. All measurements were made with a sliding calliper. The crude prevalence (the number of individuals affected regardless of preservation) was estimated to compare frequencies in individuals grouped by sex, age, and status. True prevalence (based on preserved elements) was estimated for males to compare the different elements affected, including elements where at least seventy-five per cent was preserved.
Statistical analysis
To test the differences in the distribution of WRT by sex and burial areas, χ2 tests were performed (SPSS statistical software package version 23), and p values <0.05 was considered to be significant. To test the differences between age groups, Kruskal−Wallis tests were performed.
Results
A complete list of the WRT identified in the materials from Skriðuklaustur and Västerås will be found in the Supplementary Material (S2). The bone elements affected are listed in Tables 1 and 2, while the individuals affected are listed in Tables 3 and 4. The distribution of cranial WRT is shown in Figure 3, along with ten examples of WRT in Figures 4 and 5.

Figure 3. Distribution of WRT in Västerås and Skriðuklaustur. Lines = SFT; ovals = BFT; grey = antemortem trauma; black = perimortem trauma. The hat brim line is indicated as a black band behind the crania.

Figure 4. Examples of WRT. A: E341 (Västerås), BFT antemortem; B: SKR81 (Skriðuklaustur), SFT perimortem; C: E56 (Västerås), projectile antemortem; D: B9 (Västerås), BFT antemortem; E: B157 (Västerås), BFT and SFT antemortem; F: SKR187 (Skriðuklaustur), BFT antemortem; G: B147 (Västerås), BFT antemortem; H: E200 (Västerås), SFT antemortem; I: E49 (Västerås), SFT antemortem, active healing.

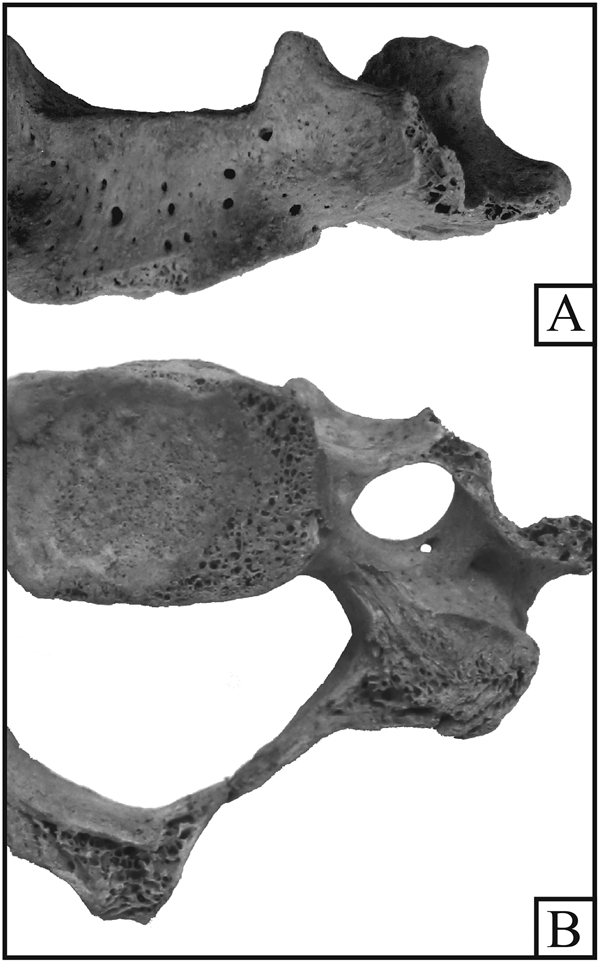
Figure 5. Grave E55 at Västerås, C5 with perimortem SFT. A: anterior view; B: inferior view.
Table 1. Distribution of WRT among males based on bone elements (true prevalence) at Skriðuklaustur.

Table 2. Distribution of WRT among males based on bone elements (true prevalence) at Västerås.

Table 3. Distribution of WRT by sex, age, and social group (crude prevalence) at Skriðuklaustur.

Table 4. Distribution of WRT by sex, age, and social group trauma (crude prevalence) at Västerås.

Skriðuklaustur
Seven (5.6 per cent) individuals had signs of WRT (BFT n = 6 and SFT n = 1). Except for the SFT, all the injuries were healed. The mandible was the most commonly affected bone (n = 4, 3.3 per cent). There was no difference in the frequencies between the sexes. WRT was identified in three (5.9 per cent) males, three (4.7 per cent) females and one (7.7 per cent) individual of undetermined sex (Table 3). The highest prevalence was found in the oldest age group, though the differences between the age groups was not significant (K-W, p = 0.293). There were no injuries related to violence in the small groups of benefactors and Augustinian canons. In the lay community, two individuals, both female, had WRT (6.1 per cent), and so did five hospital patients (6.0 per cent). A single case of SFT was found on a female skeleton among the lay sisters, which consisted of two parallel perimortem cuts to the right side of the frontal bone. Pathological changes including osteitis/osteomyelitis in the mandible, right humerus, both ulnae, radii, femora, tibiae, and the right fibula indicated that she suffered from a severe non-specific infection.
Västerås
WRT was identified in fifty-five individuals (16.1 per cent), of whom forty (72.7 per cent) had BFT and nineteen (34.5 per cent) had SFT. Four individuals (7.3 per cent) displayed both BFT and SFT. Most WRT was well healed, but there were eight cases of perimortem WRT (six SFT and two BFT) and two of SFT with active healing, indicating that these injuries were sustained only a short time before death (Figure 4, E49). Among the BFT, the frontal bone seemed especially exposed (n = 29, 80.6 per cent of BFT), while SFT was evenly distributed over the crania and found in four postcranial bones (see Supplementary Material S2). Injuries to the facial and frontal bones affected both sides equally, but injuries to the parietal bones were more than twice as common on the left than the right side (Table 2). SFT also mainly affected the left side of the crania (see Supplementary Material S2). Most cranial injuries (n = 48, 78.7 per cent) were found above the hat brim line (Figure 3), but there were also facial fractures, BFT, and SFT in the orbital region. Five individuals had multiple injuries. Four of them (E49, E56, E200, and E341) had injuries in different stages of healing, and one (B157) had all healed injuries.
Comparing the sexes, fifty-one males (19.6 per cent), three females (4.5 per cent), and one individual of undetermined sex (6.3 per cent) had WRT. Only males had SFT and perimortem injuries. Healed WRT was identified in all age categories. The frequency was higher in the older age groups, suggesting an accumulation of injuries over the course of life, but the difference was not statistically significant (Table 4; K-W, p = 0.511). The young adult group had the highest frequency of perimortem trauma, which was absent among the old adults. The frequency of WRT was similar in the high-status group (Area A−D: n = 28, 16.4 per cent) and the low-status group (Area E: n = 27, 15.9 per cent). When comparing only males, again there was no significant difference in WRT between the high-status group (n = 27, 20 per cent) and the low-status group (n = 24, 19.2 per cent; X 2(1df) = 0.037, p = 0.848).
WRT was especially common in two groups of males: those buried in the northern part of the church (Area B), where thirty per cent of the males displayed WRT, and those buried in one part of the cemetery (Graves E47−57). This pattern was especially true for SFT, as ten of the nineteen males with recorded SFT were buried in these areas, but BFT was also frequent in these males. The males buried in Area B had a significantly higher frequency of WRT than those buried in the rest of the high-status area (X 2(1df) = 3.856, p = 0.05). In the sequence of graves E47−57, seven out of eight males had WRT, including two with multiple injuries, three with perimortem trauma, and two with active healing WRT. The lowest frequencies of WRT were found in Area A, particularly the eastern nave and choir, where only three (10.7 per cent) males had WRT.
Discussion
While females at Skriðuklaustur and Västerås displayed similar frequencies of WRT (4.7 per cent and 4.5 per cent, respectively), there was a greater contrast between the males in Skriðuklaustur (5.9 per cent) and those buried in Västerås (19.6 per cent). Further differences emerged between various groups of men at the two sites. No WRT was detected in any of the males identified as Augustinian canons or lay brothers in Skriðuklaustur, in line with the more limited use of violence expected in clerical masculinity. The three males with WRT were found among the hospital patients. In Västerås, the males buried in the eastern section of the nave and the choir had the lowest frequencies of WRT. The proximity to the high altar made this the most sacred burial place (Andrén, Reference Andrén2000), suggesting that it was an area reserved for Dominican friars and the uppermost echelon of the lay elite, possibly those with a special relationship to the priory, such as benefactors. The three males with WRT buried in the eastern section of the nave were all buried in brick tombs, suggesting that they were of high status (Andrén, Reference Andrén2000: 17).
In earlier studies on monastic sites (Møller-Christensen, Reference Møller-Christensen1982; Mollerup, Reference Mollerup, Gregersen and Jensen2003; Sullivan, Reference Sullivan2004), high frequencies of WRT were found among males interpreted as warriors. The association between warriors and WRT, especially SFT, is most obvious in battlefield mass burials (Novak, Reference Novak, Fiorato, Boylston and Knüsel2000; Ingelmark, Reference Ingelmark, Thordeman, Nörlund and Ingelmarkeds2001; Kjellström, Reference Kjellström2005). Although SFT could be sustained in different circumstances, battle was a likely setting. In Västerås, SFT was common among the males buried in the northern section of the church (Area B), suggesting that they had battle experience and were possibly warriors. In this group of males, thirty per cent had WRT, mostly antemortem. WRT, particularly SFT, was also common in the sequence of graves E47–57 in the cemetery. Sven Drakenberg (Reference Drakenberg1970), director of the excavations in Västerås, has proposed that men fallen in the battle of Västerås in 1521 were buried at the priory, which might account for the observed frequencies of WRT among males.
Death in battle is, however, not believed to be the main reason for the high frequency of WRT in Västerås. Instead, most of the injuries were probably sustained off the battlefield, though by the same group of males who participated in warfare. The number of healed cranial injuries is extraordinary and interesting as these injuries have usually been reported only sporadically in cemetery collections (Knüsel & Smith, Reference Knüsel, Smith, Knüsel and Smith2014: 4). The relative frequency of 19.4 per cent (forty-five out of 232 male crania) can be compared to, for example, the victims of the Battle of Good Friday (fought in 1520 in Uppsala, less than 70 km from Västerås), where four per cent (two out of fifty-two crania) exhibited antemortem lesions (Kjellström, Reference Kjellström2005). The recurring position and large number of healed traumata to the forehead of the Västerås males cannot be explained as accidental. Instead, they can be interpreted as signs of a specific, possibly socially accepted use of violence in the performance of masculinity. It can be compared to the trauma pattern of nasal and metacarpal fractures seen in American and British males in the eighteenth–twentieth centuries (Brickley & Smith, Reference Brickley and Smith2006; de la Cova, Reference de la Cova2010). Inspired by the popularity of boxing, fist fighting replaced armed duelling as a masculine way of settling conflicts and defending honour in these contexts (Brickley & Smith, Reference Brickley and Smith2006). The pattern of WRT in Västerås is quite different and points to another practice of directing violence mainly towards the forehead, not the face. Although the lethal nature of these injuries is difficult to assess, the trauma pattern could indicate a premeditated, non-lethal intent in which thrusts or the weapon of choice harmed but did not kill the victims. At least the external cranial tables were fractured in these individuals, indicating the use of objects harder than fists. The trauma pattern could have resulted from hand-to-hand combat, but no side bias was observed. The low occurrence of trauma to the occipital bone implies no attempts at escape or attacks from behind. This trauma pattern can perhaps be associated with battle practice or non-aggressive but physically intense games. Healed BFT was most frequent among males buried in the church, interpreted as members of the elite who possibly received formal training in battle techniques by professional fighting masters or their like (Knüsel, Reference Knüsel, Knüsel and Smith2014). In these situations, the men expected physical encounters and may even have sought out these meetings to brag about the scars sustained. Researchers have called for studies that distinguish warfare from other types of violence (Knüsel & Smith, Reference Knüsel, Smith, Knüsel and Smith2014: 4), and we believe that the trauma pattern in Västerås can be used for this purpose.
One reason why men with WRT were buried in monastic cemeteries was that they were treated for their injuries there. Skriðuklaustur functioned as a hospital, and many individuals buried in the cemetery displayed pathological changes. There were also findings of surgical instruments, and pollen and seeds from medical plants (Kristjánsdóttir et al., Reference Kristjánsdóttir, Larsson and Åsen2014). All three males with WRT buried in Skriðuklaustur are interpreted as patients. In Västerås, a hospital existed next to the priory, and patients could have been buried in the cemetery (Kumlien, Reference Kumlien1971: 174, 176). It is worth noting that two males (E49 and E50) displayed signs of active healing of WRT, in both cases SFT to the cranium. These men were probably treated for their injuries at the hospital but did not recover.
The impacts of injuries are difficult to estimate, but cranial trauma can have significant neurodegenerative consequences, including behavioural changes, memory loss, and impaired motor control. Clinical studies of professional boxers have shown that the cumulative effects of repeated blows to the head can lead to chronic brain damage (Lovell et al., Reference Lovell, Echemendia, Barth and Collins2004: 237, with references). Another study (Boldsen et al., Reference Boldsen, Milner and Weise2015) found an increased mortality risk in men with healed cranial trauma in medieval Denmark. Some of the individuals buried in Skriðuklaustur and Västerås might have become permanently impaired, while others recovered at least enough to engage in violence again—as indicated by four individuals (Graves E49 II, E56 I, E200 I and E341 I) with WRT in different stages of healing.
WRT could also have had consequences for an individual's masculinity. Jónsbók, the medieval Icelandic law code, defined a disabling wound as one that rendered a person less capable than previously or could not be concealed (Schulman, Reference Schulman2010: 69). Such changes in ability and appearance could have caused what Shilling described as a crisis of masculine identity in which habitual practices were no longer possible, leading to despair but also to new ways of acting to overcome obstacles (Shilling, Reference Shilling2004: 481). The importance of an able body highlights the fluidity of masculinities and the possibility for an individual's masculinity to change over his lifetime. Here, changes are only suggested, but studies using a life course perspective and the methods of the ‘bioarchaeology of care’ (Tilley, Reference Tilley2015) might evaluate the impact of WRT on individual masculine identities in more detail.
Conclusions
Previous research has shown that violence had a normative presence in medieval Nordic society, and the use of violence was important to performing masculinity. However, there was no single ideal applicable to all; while performance in battle was a defining feature of warrior masculinities, the use of violence was more limited in clerical masculinities. In this study, the hypothesis was that these different ideals of masculine behaviour led to different practices among clerics and laymen, to be reflected in the patterns of WRT. The results appear to agree with this. While no WRT was identified among the Augustinian canons buried in Skriðuklaustur, the males buried in the church of Västerås (Area B) had a frequency of WRT of thirty per cent. The SFT among these men indicated that at least some had battle experience, and it is suggested that they were laymen of high social status and warriors. Most of their injuries were however probably not sustained in battle, as healed BFT to the frontal bone was the most common injury type. Instead, it is proposed that the same group of high-status laymen who participated in warfare also used violence outside the battlefield. The recurring pattern of injuries suggests that they used violence in specific ways. The injuries could have been sustained during violent displays of masculinity, for example during games, martial training, and fights. The results indicate that Nordic society was not equally violent for everyone everywhere and suggest that, in addition to factors such as gender, status, and social context, ideals of masculinity contributed to this diversity. We are aware that our study is based on a limited sample, and hence further analyses including a wider range of material and injury types are desirable, as are studies on the impact of WRT on individuals and the wider community, only briefly considered here.
Supplementary Material
To view supplementary material for this article, please visit https://doi.org/10.1017/eaa.2020.20.
Acknowledgements
This work was supported by the University of Iceland research fund and Västerås stad. We thank Västmanlands Läns Museum, Þjóðminjasafn Íslands, and Steinunn Kristjánsdóttir for providing access to their skeletal collections and the anonymous reviewers for their feedback.