


Introduction
The consequences of stigma are dramatic and can significantly worsen the quality of life of people with mental illness. Stigma influences a range of life domains, including employment, romantic relationships, housing/accommodation, civil participation and education (Evans-Lacko et al. Reference Evans-Lacko, Brohan, Mojtabai and Thornicroft2012a ; Carrà & Clerici, Reference Carrà and Clerici2013; Lasalvia et al. Reference Lasalvia, Zoppei, Van Bortel, Bonetto, Cristofalo, Wahlbeck, Vasseur Bacle, Van Audenhove, van Weeghel, Reneses, Germanavicius, Economou, Lanfredi, Ando, Sartorius, Lopez-Ibor and Thornicroft2013; Grifiths et al. Reference Griffiths, Carron-Arthur, Parsons and Reid2014; Rüsch et al. Reference Rüsch, Corrigan, Heekeren, Theodoridou, Dvorsky, Metzler, Müller, Walitza and Rössler2014). Several studies have showed a close link between stigma and outcomes for people with severe mental disorders. For example, as a consequence of discrimination, people with psychiatric disorders have poor social networks, are socially excluded, have reduced job opportunities and experience difficulties in accessing appropriate mental health care (Yamaguchi et al. Reference Yamaguchi, Mino and Uddin2011; Gerlinger et al. Reference Gerlinger, Hauser, De Hert, Lacluyse, Wampers and Correll2013; Volpe et al. Reference Volpe, Fiorillo, Luciano, Del Vecchio, Palumbo, Calò, Piras, Signorelli, Filippo, Piselli, De Fazio, Gotelli, Bardicchia, Cerveri, Ferrari, Mulè, Ribolsi, Sampogna, De Rosa and Sartorius2014; Del Vecchio et al. Reference Del Vecchio, Luciano, Sampogna, De Rosa, Giacco, Tarricone, Catapano and Fiorillo2015); thus, stigma represents one of the most significant obstacles to mental health care. Although several attempts have been carried out worldwide to fight stigma against people with mental disorders (Sartorius & Schulze, Reference Sartorius and Schulze2005), the levels of discrimination and prejudice towards people with mental illness are still very high (Pingani et al. Reference Pingani, Luciano, Sampogna, De Rosa, Pinna, Volpe, Del Vecchio and Fiorillo2014).
Several instruments have been validated to assess various aspects of stigma across different contexts. To our knowledge, the Reported and Intended Behaviour Scale (RIBS) is the only validated questionnaire to analyse the presence of reported and intended stigmatising/discriminatory behaviours towards people with mental health problems in the general population (Evans-Lacko et al. Reference Evans-Lacko, Rose, Little, Flach, Rhydderch, Henderson and Thornicroft2011). The RIBS is a self-administered questionnaire developed to assess reported (past and current) and intended (future) behavioural discrimination among the general public against people with mental health problems (Evans-Lacko et al. Reference Evans-Lacko, Rose, Little, Flach, Rhydderch, Henderson and Thornicroft2011). This instrument has been used in several studies demonstrating its structural validity and versatility, including the evaluation of anti-stigma campaigns (Evans-Lacko et al. Reference Evans-Lacko, London, Little, Henderson and Thornicroft2010, Reference Evans-Lacko, Malcolm, West, Rose, London, Rüsch, Little, Henderson and Thornicroft2013a ), the assessment of interventions among specific populations (Friedrich et al. Reference Friedrich, Evans-Lacko, London, Rhydderch, Henderson and Thornicroft2013) and to verify the dynamics of the construct stereotype–attitude–behaviour (Rüsch et al. Reference Rüsch, Evans-Lacko, Henderson, Flach and Thornicroft2011, Reference Rüsch, Evans-Lacko and Thornicroft2012; Evans-Lacko et al. Reference Evans-Lacko, Henderson and Thornicroft2013b ).
The RIBS has been translated and validated into Japanese (Yamaguchi et al. Reference Yamaguchi, Koike, Watanabe and Ando2014); showing good results for the RIBS-J. The internal consistency was high (α = 0.83) and the test–retest reliability (ρc) was moderate (0.71). Moreover, confirmatory factor analysis is identified as a good model fit for the RIBS-J (χ 2 = 41.001, df = 19, p = 0.002, Goodness of Fit Index (GFI) = 0.956, Adjusted Goodness of Fit Index (AGFI) = 0.916, Comparative Fit Index (CFI) = 0.955, Root-Mean-Square Error of Approximation (RMSEA) = 0.072).
Several assessment instruments, such as the ‘Community Attitudes towards the Mentally Ill Scale’ (Buizza et al. Reference Buizza, Pioli, Ponteri, Vittorielli, Corradi, Minicuci and Rossi2005; Mannarini & Boffo, Reference Mannarini and Boffo2013), the ‘Opinions about Mental Illness Questionnaire’ (Magliano et al. Reference Magliano, Marasco, Guarneri, Malangone, Lacrimini, Zanus and Maj1999) and the ‘Attribution Questionnaire 27’ (Pingani et al. Reference Pingani, Forghieri, Ferrari, Ben-Zeev, Artoni, Mazzi, Palmieri, Rigatelli and Corrigan2012), are already available in Italian language; however, those instruments mainly explore knowledge and attitudes (two out of the three components of stigma), while a specific questionnaire on reported or intended stigmatising behaviours (i.e., the third component of stigma) is not yet available in Italian language. Indeed, mental health-related stigmatising behaviours can impact on different life-domains of people with mental disorders, such as interpersonal relationships, work and housing (Evans-Lacko et al. Reference Evans-Lacko, Rose, Little, Flach, Rhydderch, Henderson and Thornicroft2011), and are rarely assessed at population levels. The aims of the present paper are to translate and validate the RIBS into Italian language and to adapt it to the Italian context (RIBS-I).
Method
Sample
The questionnaire was administered to a sample of the general public (n = 447) via distribution in public places such as shopping centres, markets, squares, cinema and other gathering places. Questionnaires were administered by trained mental health professionals. Each possible respondent was provided with the following information: (1) purpose of the study; (2) institution that promotes the study (University of Modena and Reggio Emilia); (3) structure of the questionnaire; and its contents. We obtained participant consent from all individuals and assured participants that their answers would only be used for research purposes and protected by current Italian legislation on privacy. The approval from the relevant review board was received before the start of the study. The only inclusion criterion was that individuals had to be greater than or equal to 18 years of age.
Instrument description
The RIBS considers reported and intended behaviours across four different domains: (1) living with, (2) working with, (3) living nearby and (4) continuing a relationship with someone with a mental health problem. It includes eight items, four of them explore the prevalence of reported or actual behaviour and the other four assess intended future behaviour about the four domains described above.
There are three possible answers for items 1–4 (‘reported or actual behaviour’): ‘Yes’, ‘No’ and ‘Don't know’. For items 5–8 (‘intended behaviour’) responses are provided on a 5 point Likert scale (Strongly agree – Slightly agree – Neither agree nor disagree – Slightly disagree – Disagree) or by endorsing the response option ‘Don't know’. The total intended behaviour score is calculated by summing the answers for items 5–8. The response value of ‘Strongly agree’ is 5, whereas the ‘Don't know’ answer is coded as neutral (i.e., 3), a higher score indicates a higher level of intended behaviour and/or contact with someone with a mental health problem. The following socio-demographic characteristics were collected from all participants alongside the RIBS-I: age, sex, place of birth, marital status, education level (in years), employment status, participation in events related to stigma and possible knowledge of first- and/or second-degree relatives affected by a psychiatric disorder.
RIBS translation
The translation of the RIBS was carried out in two phases: (1) three native Italian researchers, who were also fluent in English, independently translated the RIBS into Italian. Following the discussion between the three researchers, the three different translations were collapsed into a single ‘Alpha version’ of the questionnaire in Italian language; (2) the ‘Alpha version’ was then back-translated into English by a professional translator. The author of the original questionnaire (S.E.L.) was then consulted to check the adequacy of the translation with the original questionnaire. Based on this consultation, a ‘Beta version’ was developed which has been used in this validation study.
Face validity
The ‘Beta’ version of the questionnaire was administered to a sample of 30 students attending the degree course in Psychiatric Rehabilitation at the University of Modena and Reggio Emilia in order to perform face validity and to test the comprehensibility of the instrument. The choice to involve these students was due to the fact that they are in close contact with patients with mental illness and have in their degree course the study of the sociological, historical and theoretical aspects of stigma (Pingani et al. Reference Pingani, Fiorillo, Luciano, Catellani, Vinci, Ferrari and Rigatelli2013, Reference Pingani, Evans-Lacko, Del Vecchio, Luciano, Catellani, Hamati, Rigatelli and Fiorillo2015). Students were asked to rate clarity and comprehensibility of each item and to provide suggestions on how to improve those items which were unclear.
Twenty-nine students returned the questionnaire. Items 3 (‘Do you currently have, or have you ever had, a neighbour with a mental health problem?’), 4 (‘Do you currently have, or have you ever had, a close friend with a mental health problem?’), 7 (‘In the future, I would be willing to live nearby to someone with a mental health problem.’) and 8 (‘In the future, I would be willing to continue a relationship with a friend who developed a mental health problem.’) were considered as fully understandable by 100% of respondents. Items 5 (‘In the future, I would be willing to live with someone with a mental health problem.’) and 6 (‘In the future, I would be willing to work with someone with a mental health problem.’) were considered as fully understandable by 93% of respondents (n = 27). Items 1 (‘Are you currently living with, or have you ever lived with, someone with mental health problem?’) and 2 (‘Are you currently working with, or have you ever worked with, someone with a mental health problem?’) were considered fully understandable by 90% of respondents (n = 26) and by 79% (n = 23), respectively.
During the validation process, some difficulties related to the translation of ‘mental health problems’ from English to Italian arose. In Italian language the term ‘mental health problems’ refers to several clinical and non-clinical conditions ranging from acute psychiatric disorders to stressful life conditions and psychological difficulties. Since the questionnaire evaluates (actual or intended) behaviours towards people with mental illness, we decided to translate ‘mental health problems’ to ‘psychiatric disorders’.
According to comments, the ‘Beta’ version was slightly modified, and sent to the author of the original questionnaire for approval (‘Gamma’ version). In the last phase of the study, the ‘Gamma’ version was then administered to the sample of the general population. (The Italian version is available from the authors on request.)
Reliability
Cronbach's alpha was used to calculate the internal consistency of the questionnaire using 0.6 as the cut-off value for acceptable internal consistency (Cronbach, Reference Cronbach1951).
Model fit
The model fit was assessed using confirmatory factor analysis and following these reference indices: GFI > 0.9, AGFI > 0.9, CFI > 0.9 and RMSEA < 0.1 (Barrett, Reference Barrett2007). A sample size equal to five times the number of questionnaire items, but as a minimum equal to 100, is considered necessary for confirmatory factor analysis (Hatcher, Reference Hatcher1994; Hair et al. Reference Hair, Anderson, Tatham and Black1998); for this study, a sample greater than 100 was considered sufficient.
The Statistical Package Social Science 13.0 (SPSS) (IBM, 2013) and AMOS 7.0 (Arbuckle, Reference Arbuckle2006) was used for data analysis.
Result
Sample characteristics
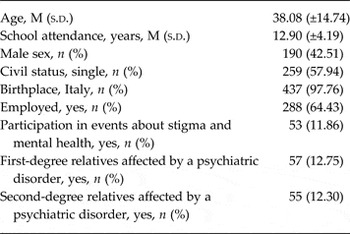
The study sample comprised 447 individuals. Table 1 describes the socio-demographic characteristics of the sample. The mean age was 38.08 (s.d. = ±14.74) with a range between 18 and 84. Fifty-seven per cent of the sample (n = 257) were female. The majority of the sample was born in Italy (437; 97.76%) and 64.43% (288) of the sample were employed. Mean education (expressed in years) was 12.90 years (s.d. = ±4.19) and 12.75% (n = 57) was reported having a first-degree relative affected by a psychiatric disorder.
Table 1. Socio-demographic characteristics of the sample (N = 447)
Distribution of participant responses
Table 2 describes the distribution of responses to the RIBS-I. For the first four questions about reported past or current behaviour, the answer ‘No’, indicating no contact with people with mental illness, was the most common response across all of the four items. The responses ranged from 83.89% (n = 375) for the first item (‘living with people with mental illness’) to 61.74% (n = 276) for the third (‘living nearby’). To items about ‘Working with’ and ‘Continuing a relationship’ with a person with mental illness the percentage of ‘No’ was 73.38 and 72.71. ‘Don't know’ was rarely endorsed; but, was most commonly indicated for items referring to the domains ‘living nearby’ (n = 50; 11.19%) and ‘continuing a relationship’ (n = 24; 5.37%).
Table 2. Distribution of participants’ responses

In the second part of the questionnaire, which explores respondents’ intended behaviours, a high percentage of participants agreed that they would be willing to work (n = 102; 22.82%), live nearby (n = 102; 22.82%) or have a relationship (n = 208; 46.53%) with someone with a mental health problem in the future (Table 2). Only 8.50% (n = 38) of respondents, however, were willing to live together with a person with a mental health problem in the future.
Internal consistency
The Cronbach's alpha of the ‘intended behaviour subscale’ was 0.83 and can be considered ‘good’ (Cronbach, Reference Cronbach1951). Removing an item of the subscale did not lead to an increase in the value of the Cronbach's alpha (Table 3).
Table 3. Internal consistency

Confirmatory factor analysis and model fit
The results of the confirmatory factor analysis are described in Table 4. The χ 2 = 23.60 (df = 19; p = 0.21) and χ 2/df = 1.24 demonstrate good model fit (p > 0.05 and χ 2/df < 2). All indices of model fit were above the reference values: GFI = 0.987 (GFI > 0.9); AGFI = 0.975 (AGFI > 0.9); CFI = 0.994 (CFI > 0.9) and RMSEA = 0.023 (RMSEA < 0.05). All items loaded significantly onto their corresponding subscale.
Table 4. Confirmatory factor analysis and model fit

*** = p < 0.001.
Discussion
The aim of this study was to validate the RIBS-I analysing its face validity, reliability and model fit. We found evidence that the RIBS-I is brief and easy to use among adult Italian members of the general public. Moreover, the psychometric properties of the RIBS-I are robust. The test of internal consistency was fully satisfied, as the overall alpha was 0.83, well above the minimum threshold of 0.6. Additionally, the proposed two models (reported and intended behaviour) were also verified by a confirmatory factor analysis which produced optimal indices and the value for the χ 2/df ratio (1.24) was above the reference value (2.0) further supporting model fit.
The Italian population reported lower levels of contacts with people with psychiatric disorders compared with the Japanese (Yamaguchi et al. Reference Yamaguchi, Koike, Watanabe and Ando2014) and English samples (Evans-Lacko et al. Reference Evans-Lacko, Rose, Little, Flach, Rhydderch, Henderson and Thornicroft2011), but higher levels of contacts compared with the people from Czech Republic (Winkler et al. Reference Winkler, Csémy, Janoušková, Mladá, Bankovská Motlová and Evans-Lacko2015), where the deinstitutionalisation process has started only recently and people with mental illness are still confined to the borders of the society. Moreover, compared with the Italian sample, the English and Japanese samples are more willing to have future contacts with people with mental illness. This discrepancy could be due to the fact that in Japan (Kadri et al. Reference Kadri and Sartorius2005) and in the UK (Evans-Lacko et al. Reference Evans-Lacko, London, Japhet, Rüsch, Flach, Corker, Henderson and Thornicroft2012b ; Livingstone et al. Reference Livingston, Tugwell, Korf-Uzan, Cianfrone and Coniglio2013) anti-stigma campaigns were specifically targeted to reduce reported and intended behaviours (Evans-Lacko et al. Reference Evans-Lacko, Malcolm, West, Rose, London, Rüsch, Little, Henderson and Thornicroft2013a ). In particular, anti-stigma campaigns carried out in the UK have facilitated a direct contact between people with and without mental illness, and actively involved mass media and personal testimonials of people with mental illness. On the contrary, anti-stigma campaigns carried out in Italy over the last 20 years have mainly focused on providing knowledge and information about mental disorders to the general population (Zoppei & Lasalvia, Reference Zoppei and Lasalvia2011).
Fifty-five per cent of respondents affirmed that they would be willing to work with a person with a psychiatric disorder in the future, and an even higher percentage (about 80%) reported that they would continue a relationship with a friend if he/she became ill; on the contrary, a low percentage of respondents reported that they would be willing to live with someone with a mental health problem (about 28%). These findings, which are similar to those reported by Evans-Lacko et al. (Reference Evans-Lacko, Rose, Little, Flach, Rhydderch, Henderson and Thornicroft2011) and Yamaguchi et al. (Reference Yamaguchi, Koike, Watanabe and Ando2014), are of interest given previous findings (Thornicroft et al. Reference Thornicroft, Brohan, Rose, Sartorius, Leese and Group2009; Lasalvia et al. Reference Lasalvia, Zoppei, Van Bortel, Bonetto, Cristofalo, Wahlbeck, Vasseur Bacle, Van Audenhove, van Weeghel, Reneses, Germanavicius, Economou, Lanfredi, Ando, Sartorius, Lopez-Ibor and Thornicroft2013), which highlighted that almost half of the individuals with a diagnosis of schizophrenia reported stigma or discrimination in the area of making or keeping friends.
This study has four relevant limitations: (1) the sample was a convenience sample and it was not ‘a-priori’ defined; (2) participants were recruited from only two geographic areas (urban centres in Northern and Southern Italy); thus, our findings are not fully generalisable to the Italian context and need replication; (3) concurrent validity, convergent/divergent validity and test–retest reliability have not been tested; (4) the results obtained in this study may be affected by ‘social desirability’: as described by Henderson et al. (Reference Henderson, Evans-Lacko, Flach and Thornicroft2012), online surveys or telephone interviews are preferred by respondents since they guarantee anonymity; (5) stigma towards patients with special needs, such as those living in prison or in forensic institutions, were not investigated (Carrà et al. Reference Carrà, Giacobone, Pozzi, Alecci and Barale2004).
RIBS-I represents a useful tool to: (1) assess (actual or intended) stigmatising behaviours in the general population via a short, reliable and validated questionnaire; (2) evaluate anti-stigma interventions (Pingani et al. Reference Pingani, Luciano, Sampogna, De Rosa, Pinna, Volpe, Del Vecchio and Fiorillo2014); (3) differentiate stigmatising behaviours from stigmatising attitudes and knowledge. Moreover, the RIBS-I should be used both to evaluate baseline levels of intended and reported stigmatising behaviours in the general population as well as to assess the effectiveness of anti-stigma campaigns.
Financial support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Conflict of Interest
S.E.L. currently holds a Starting Grant from the European Research Council and has received consulting fees from Lundbeck.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.




