


Disaster risk management (DRM) consists of 4 phases: mitigation and prevention, preparedness, response, and recovery. Reference Norige, Yenson and Elkin1 Preparedness is the most important phase in the process of the DRM. Preparedness is actions that take place beforehand to make sure of effective response. Reference Sheikhbardsiri, Yarmohammadian and Khankeh2,Reference Sheikhbardsiri, Yarmohammadian and Khankeh3 Among different variables in DRM, the health system as the most important organization can provide preparation plans and proper strategies to decrease casualty, social, and financial damage. Reference Savoia, Biddinger and Burstein4,Reference Thomas, Hsu and Kim5 In developed countries, most health centers must have a plan for preparedness and development of their skills for the response to the disaster, and this plan must be up-to-date, and all personnel must be aware of that. Reference Khankeh, Khorasani-Zavareh and Johanson6-Reference Rezaei, Maracy and Yarmohammadian8
One way to increase and maintain preparedness of health system is the implementation of disaster exercise. Reference Khankeh, Lotfolahbeygi and Dalvandi9,Reference Radi and McAdams10 Exercise in different units of the health system is one of the most important steps toward designing and implementing DRM plans, especially in the response phase. In exercise, the real situation is simulated to make people mentally and physically prepared and respond properly based on plans in case of the real situation. Reference Thang and Khuong11-Reference Jalou, Nouri and Rohani-Rasaf13 Disaster exercises can play a role in validity assessment of policies, plans, procedures, training of roles, personnel responsibilities, development of performance, and inter-organizational communication and cooperation. Reference Skryabina, Reedy and Amlôt14,Reference Savoia, Agboola and Biddinger15 There are 2 types of disaster exercise: (1) discussion-based and (2) operation-based. Reference Edwards and Goodrich16
Djalali et al. Reference Djalali, Carenzo and Ragazzoni17 conducted a study titled “whether disaster preparedness may predict hospital response performance over operational exercise” in Piedmont, Italy. The researchers stated that the relationship between hospital preparedness and responses to disaster required principle implementation of functional exercise following the Incident Action Plan (IAP). Sheikhbardsiri et al. Reference Sheikhbardsiri, Yarmohammadian and Khankeh2 in the study titled “an operational exercise for disaster assessment and emergency preparedness in the south of Iran” showed that the important goal of DRM and promotion of health system preparedness were necessary to develop and test operational response plans with the collaboration of all of the stakeholders through implementation of standard operational exercises.
Annually, most health-care system resources are spent on performing disaster preparedness exercises, but due to the lack of well-designed programs and guidelines for the standard implementation of these exercises, macro goals and outlined prospects in the health system preparedness for disasters have not been achieved or they do not have evaluation capabilities and necessary scientific measurement. Therefore, considering the importance of promoting health system preparedness through exercise, the present study aimed to identify and explain the components affecting successful implementation of preparedness exercises of the health system in disaster. The findings of this study can be considered as a guideline for the implementation of principle and standardized health-care system preparedness exercises.
METHODS
Study Design
This qualitative study was done in 2019, and a content analysis approach was used for conducting the study. Content analysis can be used with either qualitative or quantitative data and in an inductive or deductive way. This approach is useful when an existing theory or research literature on a phenomenon is limited. Reference Hennink, Hutter and Bailey18
Setting, Participants, and Data Collection
This qualitative study was conducted in Iran, as one of the most disaster-prone countries in the world. Study participants included 25 disaster experts, who had practical experience or theoretical knowledge about “design, implementation, and evaluation of health-care system preparedness exercises in a disaster” and had at least 1 experience in operation-based or discussion-based exercises. Participants were chosen using a purposeful sampling method with maximum diversity. Sampling was carried out until data saturation occurred, ie, when the researcher concluded that further interview would fail to provide new information. Participants included 7 prehospital directors, 4 hospital directors, 2 nursing experts in hospital incidents committee, 4 experts in emergency operation centers (EOC) in the University of Medical Science, 6 health experts working in disaster risk reduction office, and 2 deputies of the logistic of the University of Medical Science.
The interviews were conducted by H.S.H. face-to-face and individually. The process of data collection was under the supervision of D.H.K. The interviewees answered to a similar set of questions which began with “What is your experience about the implementation of preparedness exercises of the health-care system in disaster?”, “Describe the worst and best disaster exercises that you have experienced in the health-care system, “Based on your experience, what components and features should a standard discussion-based exercise have? What components and features should a standard operation-based exercise have? What requirements and functions should be considered for implementation of discussion- and operation-based exercises in disaster? Based on the above conduction, additional questions were raised during the interview and when authors found new concepts. Moreover, who, when, why, and how, were used for concept saturation as well as “Could you please give an example” or “Please explain more” for data and concept saturation. The interviews were taped and lasted from 25 to 90 min. The place and time of the interview were selected by agreement between the interviewer and the interviewee; field notes were written during interviews to describe and interpret the responses correctly.
Ethical Considerations
The study was approved by the Ethics Committee of Kerman University of Medical Sciences with code of ethics KMU.REC.1398.668. Informed consent was obtained orally and in writing before the interview after explaining the aim and process of the study. In addition, participants were informed about the purpose of the study, the interview method, confidentiality of their information, and right to withdraw from the study at any time.
Data Analysis
Qualitative directed content analysis was used to analyze the data. Systematic stages were followed and simultaneous analysis was undertaken: first, recorded interviews were transcribed verbatim. Then, before coding, the transcribed text was read several times for familiarization. In the initial coding process, the participants’ words were used and condense meaning units were formed; and then the codes were categorized into subcategories based on their similarities and differences. This process continued for all interviews until the formation of the main categories.
Reliability and Validity
This study used strategies recommended by Lincoln and Guba for reliability and validity of the tests. According to this recommendation, 4 criteria of creditability, dependency, conformability, and transferability are required to ensure reliability. Credibility was ensured through assigning sufficient time for data collection and analysis, prolonged engagement with the participants, constant comparison of participants’ expressions, understanding their experiences by the researcher and maximum variety of the participants. Conformability was achieved by member check, peer check, and expert check. Member check was done by returning the text of interview and summary of results to 4 participants for confirmation of the findings. The validity of data collection and analysis process was checked by 2 qualitative researchers in the research team (expert check and peer check).
RESULTS
Demographic of Participants
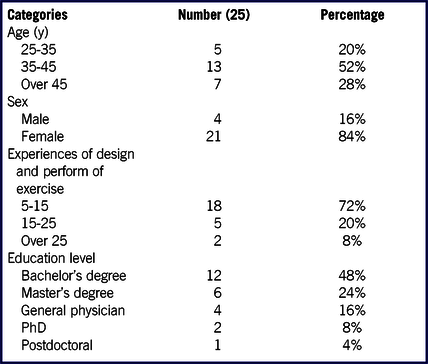
The participants included 4 females and 21 males with a mean age of 42.25 ± 4.8 y ranging from 25 to over 45 y. The mean work experience was 15.5 ± 3.4 y and all participants had more than 5 y of work experience in implementation of preparedness exercises of the health-care system in disaster (see Table 1).
TABLE 1 Demographic Characteristics of the Participants
Main Results
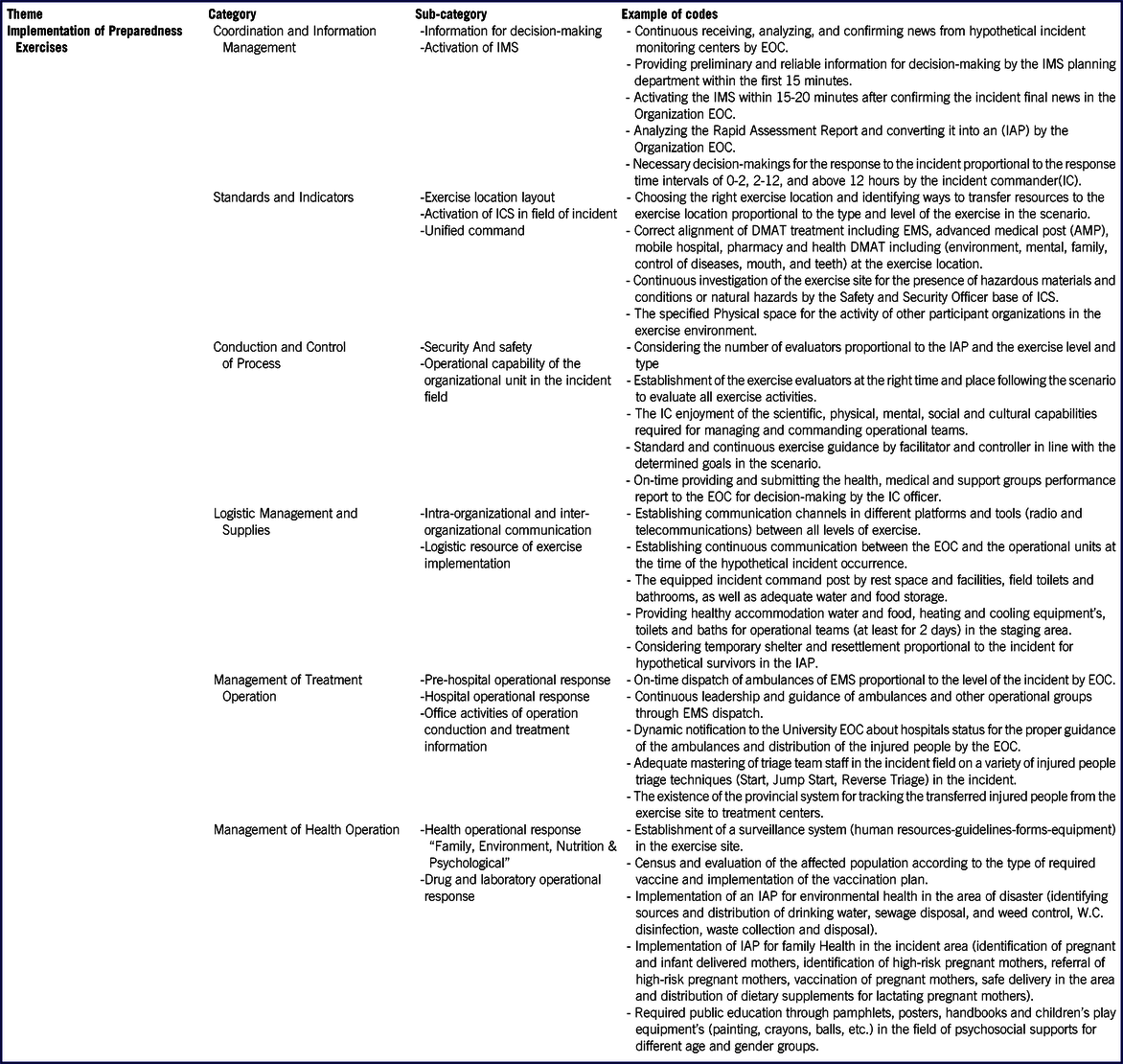
An original theme with the name of implementation of exercise, 6 main categories, 14 sub-categories, and 100 codes were formed: coordination and information management (with 2 sub-categories of information about decision-making and activation of Incident Management System [IMS], standards and indicators (with tree sub-categories of exercise location layout, activation of Incident Command System [ICS] in field of incident and unified command), conduction and control of process (with 2 sub-categories of security and safety and operational capability of the organizational unit in the incident field), logistic management and supplies (with 2 sub-categories of intra-organizational and inter-organizational communication and logistic resource of exercise implementation), management of treatment operation (with 3 sub-categories of prehospital operational response, hospital operational response, and office activities of operation conduction and treatment information), and management of health operation (with 2 sub-categories of health operational response including “family, environment, nutrition, & psychological” and drug and laboratory operational response) (see Table 2). The main categories and sub-categories are described in the following sections.
TABLE 2 Theme, Categories, Sub-categories of Components Affecting Implementation of Health System Preparedness Exercises in Disaster
Main Theme
Exercise Implementation
Implementing discussion-based and operation-based exercises in different parts of the health system is one of the important steps in providing and developing disaster risk management plans, especially in the response phase, and also, implementing disaster exercises can play a role in testing the validity of policies, plans, procedures, improving individual performance and inter-organizational communication and coordination.
Categories and Subcategories
(A) Coordination and Information Management
The early warning process must be effectively disseminated at the time of implementing the exercise to ensure concerted actions at the time of response to a hypothetical incident, and activate and operationalize the IMS after receiving and analyzing the incident information and dispatching rapid assessment teams to the incident area requires coordination and information management.
Information for Decision-Making
Providing accurate and on-time information to activate the IMS was one of the important and main issues that the participants emphasized.
“I think an organization manager should have the power of decision-making at the time of implementing the exercise and the actual incident after receiving on-time information. He/she should make necessary decisions to respond the incident proportional to different time intervals of 0-2, 2-12, and 12 hours” (P12).
“What we want to do well is receiving on time and reliable information from the incident but we can’t say how long after the incident I receive the information to make a decision as an official…” (P1).
Activation of IMS
IMS is one of the important structural pillars of DRM for an accurate and standard response to incidents at different levels. The important thing is that after receiving the incident information at the time of our response, the IMS should be activated in the university EOC headquarters, not the ICS; therefore, ICS is one part of IMS that must be established and activated in the incident field and this is true at different levels of the incident including the local, polar, and national levels.
“I think we have to go the direction, like other countries, to activate IMS at national, university, pole levels, and the ICS was active at the university level, now it is better to be activated in the incident field” (P9).
(B) Standards and Indicators
Many organizational preparedness factors in confronting with disaster through performing exercise are influenced by clear standards and indicators in the operational plan of the organizational response.
Exercise Location Layout
The order and placement of the participating organizational units at the exercise site play a significant role in coordinating the units in response to the incident at the time of implementing the operational exercises.
“At the time of the implementation of operational exercises, it is important to know where our AMPs (advance medical post) and staging area are located and to specify where the involved organizations are located at the exercise location and to what geographical area the participating organizations are required to operate” (P4).
“The exercise area zoning is one of the cases that we should consider at the time of implementing the exercise, for example, zoning based on specific techniques such as color ribbons …” (P12).
Activation of ICS in the Incident Field
Institutionalizing the ICS in the exercise executing organization is recognized as one of the most important items of the exercise indicators and standards and using the ICS to avoid confusion, uncertainty, chaos, and arbitrary works as well as shortening the time to respond to an incident and reducing its complications when occurring in health-care centers can lead to proper and productive DRM.
“The important thing that comes to my mind during implementing the exercise is that the incident command post (ICP) should be well-equipped according to our upstream documents and activated following the time sequence plan that the exercise planning team designed …” (P2).
“In addition to all staff in the exercise executing organization who should be familiar with the ICS chart as their main role, the staff of other organizations participated in the exercise should know it …” (P10).
Unified Command
Lack of a clear and unified command in the disaster is one of the reasons for disorganizations in the stricken area and was observed in past natural disasters of Iran that each organization had the separate commander for itself and there was no single commander who put all organizations under his control and took over the organization.
“As someone with years of experience in disaster, there is still no directive on how to designate a commander in any incident in Iran, and it is sometimes seen that some officials are using their positions to force organizations to obey them and get them to do things according to their tastes” (P12).
“The unified command topic has not yet settled, in fact, after some years we tried to tell the Red Crescent ambulances that the transportation of injured people is the responsibility of emergency medical system (EMS), or if you transport them, it must be under our control but still …” (P15).
(C) Conduction and Control of Process
Monitoring must be carried out to monitor the structure of the processes produced during the design phase of the exercise and this control must be implemented continuously and focused by the exercise evaluators or simulators.
Security and Safety
All the organizations that participated in the exercise must observe a set of principles for establishing and ensuring the safety and security of a hypothetical incident location that will contribute to the order and safety of the exercise, such as having identification tags or signs that help organizations responsible for incident scene safety.
“In the exercises, just like a real incident, the safety and security of all participants must be maintained, for example, in a real incident like the Kermanshah earthquake, they couldn’t secure the scene, the relief organizations’ staff were beaten, so it’s important to protect all the exercises’ sources well” (P22).
Operational Capability of the Organizational Unit in the Incident Field
One of the important and valuable subjects at the time of implementing the exercise is the individual and functional skills of the exercise staff, especially the exercise controllers, simulators and evaluators.
“It is very essential and important that all the individuals who are selected as the exercise evaluators have the necessary knowledge related to disaster and also have enough experience in evaluating disaster exercises in different levels to specifically evaluate the work done by other players participating in the exercises” (P17).
(D) Logistic Management and Supplies
The obtained findings from the present research analysis confirm the fact that no operation without proper support can achieve its goals, because logistic and supply of the incident scene needs is like delivering blood to living cells in the body because they will stop moving without blood and the rhythm of their lives will drop.
Intra-organizational and Inter-organizational Communication
Analyzing the obtained data from the interviews with the experts showed that the communication ways across the various radio and telecommunication platforms and social networks between all levels of the exercise should be existed properly and in a standard manner, and also radio communication and channels and social networks must be designed and established to communicate between all collaborating and supporting organizations in the exercise for greater coordination and synchronization of response to the disaster.
“I believe that one of the approaches for inter-organizational communication is virtual networks such as telegram, WhatsApp, etc., to send incident information from the incident scene, even early warning to prevention and send a scene-by-scene video to the IMS by the rapid assessment team to decide and activate the IMS in the form of the social network” (P23).
Logistic Resource of the Exercise Implementation
One of the major issues emphasized by the health experts in the field of disaster in Iran was the establishment of logistic staging areas proportional to incident level (local, polar, and national).
“One of the executive requirements of any exercise is to have the support and logistics that can include various forms of operational activities in the logistic staging areas, such as transporting and distributing essential goods, establishing channels of communication between intra- and extra-organizational units, health, water, food, shelter, and hygiene facilities for all participants of the exercise” (P15).
(E) Management of Treatment Operation
The main goal of the management of exercise treatment operation is to establish a coherent, integrated, and coordinated operational context to focus on therapeutic activities in response to disaster; in other words, the Emergency Operational Plan (EOP) describes the functions of health operations at the time of response to disaster divided into units and departments responsible.
Prehospital Operational Response
The prehospital emergency is among the first units of the health system in response to the disaster. This point is very important, that the role of the prehospital system in disaster conditions can prevent overcrowding in hospitals while providing services to most people with limited facilities in addition to effective scene management, prioritization of the injured people, triage and provision of emergency life-sustaining medical services, and transfer of the injured people from the scene to the treatment centers.
“Timing function is very important in prehospital operation because sometimes the EMS is known as the eye of the university of medical science, so it is important that the dispatch unit of EOC sends out ambulances according to the information obtained from an incident scene based on the guideline of Iran health system” (P11).
“Regarding the structure and activation of the prehospital emergency when responding to the disaster, which I think should be considered in the exercise as well as the actual incidents, we decide to consider its activation level in 3 levels of less than 10, 10 to 40, and more than 40 injured” (P9).
Hospital Operational Response
From the health experts’ point of view, in exercise, hospital operations in the disaster include functions such as rapid assessment, triage, surge capacity, activation of hospital Disaster Medical Assistance Team (DMAT), health-care delivery, inter-hospital transfer, evacuation, disinfection, and overcrowding management in the hospital.
“Important hospital departments in response to disaster are the emergency department and surgery room, because when an incident happens, many of the injured who are relatively good, come to the emergency department, so, it is very important for the hospital to have a surge capacity plan” (P4).
“One of the important issues to be considered in the disaster is the function of the mobile hospital, which some experts agree with its establishment in the incident field and some disagree.”(P3).
Office of Activities of Operation Conduction and Treatment Information
The office of operation conduction and treatment information of universities usually is located in a Disaster and Emergency Medical Management Center (DEMMC) and is mostly responsible for inter-hospital coordination based on the admission of patients and injured people between hospitals covered by the University of Medical Sciences; therefore, the role of this organizational unit is also significant at the time of response to the disaster.
“Office of operation conduction and treatment information has an important position in time of response to disaster, especially in providing information of the latest status of the hospitals, including the extent of the injured people admitted and the availability of equipment and personnel and other resources for the EOC. On the other hand, it can monitor the conduction of ambulances and the distribution of the injured people between hospitals, and these functions should be investigated during operational exercise” (P19).
(F) Management of Exercise Health Operation
Another main category of the exercise implementation phase that was obtained from the perspective of the disaster specialist was the issue of health operations and activities in the exercise to obtain necessary preparedness for the timely and appropriate response to the disaster.
Health Operational Response Included (Family, Environment, Nutrition, & Psychology)
One of the important activities in the time of response to the disaster was the response of the health organizational unit, including communicable disease management, noncommunicable disease management, environmental health, family and population health, nutrition, mental-social supports, and health education that must be investigated and evaluated in operational exercises.
“At the time of exercise, the functions of the health section must be evaluated parallel to those of the treatment section for exercise ‘hypothetical incidents’ that in this field we have a comprehensive and valid reference (EOP) that we can refer to and evaluate these functions proportional to the level of exercise” (P13).
“Generally, the position of environmental health can be one of the important dimensions of the health exercises, so that its final goal must be monitoring healthy drinking water providence required for affected area population and rescuers” (P11).
“One of the issues that must be considered as a health function is vulnerable people in incidents and disaster in terms of health that must be prioritized at the time of response to the disaster. These people include pregnant women, the elderly people, the disabled people, and children under 5 y, and it is good to involve these people in our hypothetical injured people at the time of exercise implementation to provide better services to these people in real-time” (P12).
Other important functions in the field of health in the disaster from the perspective of experts in the field of psychosocial supports included establishing a scientific advisory committee on training, executing, monitoring, and evaluating psychosocial supports interventions.
“People should have access to mental health and social services at the time of disaster so that they can reduce their social problems and illnesses caused by mental disorders and disabilities. The work that I have not seen in the exercises so far, is conducting cultural and religious ceremonies. Since we live in a religious and Muslim country, we need these issues to be considered in real incidents and in our exercises” (P14).
Drugs and Laboratory Operational Response
The most important specialized functions of laboratories services in disaster from the perspective of health experts include: assessing the status of laboratory services in the affected area and managing laboratory services.
“Laboratory services are not only required in the early moments in disaster conditions but also can especially become important over time” (P10).
Drug supply is one of the most important pillars in the response to disaster, the drug supply chain in disaster sometimes coincides with the drug supply process under normal circumstances, and the expected change is the speed of performing the process or financing.
DISCUSSION
Coordination and Information Management in the exercise was among the main categories that were extracted during the exercise implementation phase. Finding information for decision-making was one of the subcategories derived from an interview with health experts. This finding is consistent with the study of Comes et al., Reference Comes, Vybornova and Van de Walle19 Alamdar et al., Reference Alamdar, Kalantari and Rajabifard20 and Waring et al. Reference Waring, Alison and Shortland21 Providing appropriate information is a requisite for any kind of planning at different levels of incident management. Planning for obtaining preparedness and response requires adopting effective decisions based on correct and structured information that is quickly and easily accessible to decision-makers; therefore, it is obvious that the more desirable and timely the information, the more desirable the decisions are adopted and as a result, the losses and wastes resulting from the incident will reduce.
Standards and indicators of the exercise were one of the main categories extracted from the analysis of interviews with health experts. The findings obtained from the analysis of the present study confirm this fact, that many aspects of an organizational preparedness in response to disaster through implementing exercise are influenced by the existence of clear standards and indicators in the operational plan of the organization. The organization can practically engage its employees in response to the disaster and reduce the number of casualties caused by the disaster. According to health experts’ perspective, one of the important standards and indicators of the exercise is the existence of the ICS and its activation along with the ICP in the incident field. Different researches about this finding show that one of the strategies of health organizations to respond to disaster is the implementation of the ICS in the incident field. Reference Delshad, Fariba and Hamaidreza22,Reference Born, Briggs and Ciraulo23
Unit command is one of the subcategories derived from interview with health experts. From the health experts’ point of view, the integrated command is a very important issue in multi-agency or multi-regulatory DRM. This finding is consistent with the studies of Walsh, Reference Walsh24 Anderson et al., Reference Anderson, Compton and Mason25 and Annelli Reference Annelli26 called the national IMS as a multi-agency approach for the response to the disaster. They emphasized the need for a Multi-Agency Coordination System (MACS) as the basis for a unified command. This form of command provides guidance that enables organizations with different geographical and administrative responsibilities to coordinate, obtain shared planning, and effectively control the incident. Unfortunately, in Iran, we do not have a defined command unit in DRM, and organizations of passive defense, crisis management, Red Crescent, and EMS perform their duties at the incident scene, and there is no definite and managed coordination and synergy at the time of response to the disaster.
Conduction and control of the exercise process was one of the main categories derived from the analysis of data obtained from interview with health experts in disaster. Various studies have dealt with the importance of the 2 main categories, command and control, as the underlying principles for standard, correct, and on-time response to disaster. Reference Khankeh, Khorasani-Zavareh and Johanson6,Reference Vidan and Hogan27 These findings are consistent with our findings based on the necessity of standard evaluation and control for exercise implementation. Controllers monitor the order of events and incidents occurrence and the output of messages. Therefore, it is very important and essential that individuals selected as controllers and evaluators of the exercise have the necessary knowledge and expertise related to disaster as well as sufficient experience related to conducting and evaluating disaster exercises at different levels. In this way, they can investigate the actions performed by the respective staff of the organization and different organizations that participated in the exercises, with respect to the specified goals in the exercise design stage in a specialized manner, and finally identify the strengths and weaknesses of the performance of the exercise implementation for the future actions in the hot wash of the exercise.
Logistic management and supplies was another main category that was extracted in this study. The exercise logistic staging area is one of the key pillars of responsiveness activity from the interviewees’ perspective, without which no operation can be accomplished. They also believed that exercise support and logistics included a range of operational activities, including support, actions handling, transportation and distribution of essential goods, communication channels between the intra- and extra-organizational units in the exercise, health, water, food, shelter, and hygiene facilities for all of the participants in the exercise. This finding was consistent with results of several studies. Reference Cozzolino28-Reference Sheikhbardsiri, Raeisi and Nekoei-Moghadam31
Management of treatment operation of the exercise was another main category that was extracted in this study. From the participants’ point of view, the most important operational response functions of EMS in the disaster that must be assessed in the operational exercises include prehospital rapid assessment, prehospital operational groups’ dispatch and guidance, scene command, prehospital services, injured people triage, and primary medical search and rescue. This finding was consistent with the results of other studies. Reference Catlett, Jenkins and Millin32-Reference Sheikhbardsiri, Shirdel and Molavi-Taleghani34
From the researcher’s point of view, the observing agencies, the media, and the general public measure the overall performance of the responsible and involved systems in disaster based on their speed and rapid response to the incident, not based on the duration of their participation and presence in the incident field. Therefore, attention, development, and enhancement of the preparedness of EMS in unexpected incidents can be considered as a key component for success of the medical sciences universities.
Another main category of exercise implementation from the interviewees’ perspective was the issue of management of health operation in the exercise to obtain necessary preparedness for an on-time and appropriate response to the disaster. Ensuring establishment of proper shelter, waste and sewage disposal, access to safe water and food, and primary health-care services are the most important measures that lead to the health of natural disaster survivors. Communicable disease control is considered as a key component of the health system response stage and has a vital role in maintaining the health of the survivors. This affair requires coordination and cooperation among different systems at different local, regional, national, or international levels in the provision of health, water, food, and shelter. Reference HabibiSaravi, Seyedin and Rad35 It must be remembered that, at the moment of incidents and disasters occurrence, due to the stress and excitement caused by the incident, the individuals presented at the scene of the incident are confused and have lack of decision-making power and will not be able to make the right decision in the first few hours of the disaster and perform correct response operations. Reference Quinn, Hsiao and Truman7,Reference Blum and Paradise36
Strengths and Limitations
The strength of this study is the diversity of participants from different sections of the health system, including, prehospital, hospital, disaster risk reduction, health (environment, family, psychology, and exposure to diseases), and deputies of logistic, nutrition, and drug organization in the different universities of medical sciences in Iran. In addition, compared with quantitative studies, the low number of participants may be another limitation; however, the rich and well-saturated information from participants could overcome this manner.
CONCLUSIONS
This study provides a clear and obvious picture and rich, constructive information about the concept of health preparedness exercises in disaster. According to the themes obtained in this study, the Iran health sector is in the process of acquiring, maintaining, and upgrading its preparedness plan through the implementation of discussion-based and operation-based exercises. This requires the implementation of important steps from the predesign phase to the end of the exercise recovery phase, so that any ignorance and laziness in these steps will disengage those individuals and organizations from the process of preparedness and from the units within and outside of the organization that fail to have a standard response to the disaster. Therefore, the preparedness of the Iranian health sector in the face of disaster requires a proper understanding of the concept of exercise and the importance of the exercise implementation position as one of the most important issues of preparedness by the health authorities and policy-makers as process owners.
Acknowledgments
The authors thank all the disaster specialists who participated in this study.
Author Contributions
H.S. and H.K. participated in the design of the study; recruited, enrolled, and interviewed participants; coded their data; and drafted the manuscript. M.M. participated in the design of the study, helped code data, and drafted the manuscript. S.M. participated in the design of the study and helped draft the manuscript. H.K. have read and approved the final manuscript.
Conflicts of Interest Statement
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data
The data sets generated during the current study are available from the corresponding author.


