

On December 26, 2004, one of the strongest earthquakes ever recorded occurred beneath the ocean off Indonesia and generated an unprecedented tsunami across the Indian Ocean. The tsunami crashed into a dozen countries, including a 1000-km stretch of the coastline of the island of Sri Lanka. Waves ≥10 m high carrying dangerous debris reached hundreds of meters or more inland and devastated unsuspecting communities.1, 2 The total death toll exceeded 200,000, and in Sri Lanka more than 35,000 people were killed, 23,000 were injured, and 576,000 were displaced.3 Precise casualty figures for the tsunami will remain subject to conjecture because of the wide scope of the disaster, and the full cost of its psychological impact will take years to unfold and assess.4 From a public health standpoint, it is important to systematically evaluate the resulting psychological problems of a wide range of affected populations, the results of which will continue to be of vital importance to the recovery effort and future disaster preparedness.
The available literature on postdisaster psychological impairment points to a range of factors that suggest the vulnerability of an individual within a community to develop serious or lasting psychological problems. Sex, age, prior experience with similar events, ethnicity, culture, socioeconomic status, existing family structure and problems, severity of exposure, secondary stressors, predisaster psychiatric history and personality, and availability of psychosocial resources have been shown to play some role.Reference Norris, Friedman and Watson5 Among the range of possible psychological problems, the phenomenology of posttraumatic stress disorder (PTSD) has received widespread attention because of its recognized debilitating impact on affected subjects,Reference Foa, Stein and McFarlane6 and depression is found to be the most common comorbid condition associated with PTSD.Reference Brady, Killeen, Brewerton and Lucerini7
As defined in the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (DSM-IV), PTSD is an anxiety disorder precipitated by a traumatic event and characterized by symptoms associated with 3 areas: reexperiencing the trauma, avoidance and numbing, and hyperarousal.8 Each individual's experience of a disaster is unique, and the extent of exposure to the stressor is probably the most important risk factor for the development of PTSD.Reference Galea, Nandi and Vlahov9 It also has been found that when faced with a traumatic event, women consistently display greater vulnerability than men to developing PTSD.Reference Tolin and Foa10, 11 A risk profile of disaster victims is critical for mental health providers to help them identify, design, and implement mental health interventions. Given the literature supporting gender predisposition to PTSD and the importance of treatment to the recovery effort, the authors examined the prevalence and risk factors contributing to PTSD at the 6-month point postdisaster among subjects still living in temporary shelters.
METHODS
Study Design
The present study was conducted in June 2005, exactly 6 months into the recovery phase after the disaster. To reduce the likelihood that participants were exposed to unrelated indeterminate stressors before the tsunami, 5 adjacent coastal districts—Hambantota, Matara, Galle, Kalutara, and Colombo—in southern and southwestern Sri Lanka were selected for the study. Within these 5 districts, 7 temporary camps were selected by convenience sampling for the recruitment of subjects. At each campsite, 20 to 86 individuals were interviewed based on availability at the time of the visit, which varied randomly from 8 am to 7 pm. From each shelter with 1 family, 1 or 2 participants were enrolled.
Instruments and Data Collection
Posttraumatic stress disorder was measured using an adaptation of the PTSD Symptom Scale-Interview version (PSS-I). The PSS-I is a semistructured interview instrument with 17 items corresponding to the 17 symptoms of PTSD in the DSM-IV.Reference Foa, Riggs, Dancu and Rothbaum12 Each item consists of 1 brief question, and the participant's answer is obtained as “yes” for presence and “no” for absence of the respective symptom. To meet the criteria for PTSD, participants had to report the presence of ≥1 items of the reexperiencing criterion (B), ≥3 of the avoidance criterion (C), and ≥2 of the hyperarousal criterion (D).Reference Foa and Tolin13 PSS-I has been shown to have good validity when compared to the Clinician-Administered PTSD Scale, one of the most frequently used PTSD scales. PSS-I has been shown to be reliable as indicated by internal consistency, item–total correlations, intersubscale correlations, and total scale correlations.Reference Foa and Tolin13
Depression was measured by the widely used Center for Epidemiological Studies-Depression (CES-D) scale,Reference Thomas, Jones, Scarinci, Mehan and Brantley14 which is a 20-item scale. Each question has 4 levels ranging from 0 to 3.0, with 0 being “rarely or none of the time,” and 3 being “most or all of the time” or “five to seven days.” The total score ranges from 0 to 60, with the accepted cutoff for the presence of depression being 16.Reference Thomas, Jones, Scarinci, Mehan and Brantley14 The cut-score of ≥16 yielded a sensitivity of .95 and a specificity of .70 in predicting major depressive disorder.Reference Thomas, Jones, Scarinci, Mehan and Brantley14 This instrument has been validated in Sri Lanka and other countries in south Asia,15 as well as cross-culturally.16
Other covariates included age, sex, marital status, religion, education level, social support, employment status, self-rated health before and after the tsunami and magnitude of exposure to the tsunami, amount of thinking about the event during the past month, and history of any psychological counseling received since the trauma. Education level was assessed as a categorical variable of <10 years, 10 years, and >10 years of schooling, based on the fact that grade 10 examinations act as an entry point for pursuing further studies within the public education system.16 Social support was measured by a shortened version of the MOS Social Support Survey, a 35-point scale consisting of 7 questions of 5 points each, with higher scores indicating greater social support. This scale has been used previously in populations that have experienced acute trauma.Reference Jaycox, Marshall and Orlando17, Reference Marshall, Orlando, Jaycox, Foy and Belzberg18
Current health and health before the tsunami were measured by a self-rated health item, with responses ranging from 1 (very poor) to 5 (excellent). The magnitude of exposure to the tsunami was evaluated in 2 ways. First, exposure was recorded by asking respondents where they were located in relation to the ocean at the time of the tsunami, with 3 options: at the beach, location visible to the ocean, and a distance away from the ocean. These were collapsed into 2 categories: at or near the ocean and distant from the ocean. The second exposure variable was the number of people they knew who were lost in the tsunami, with 4 options: immediate family, relatives, others, or none. These options were collapsed into 2 categories: family or close relatives and others or none. Subjects also were asked if they had received any psychological counseling from anyone while living in the camp after the tsunami.
Ten preinternship medical graduates, who are Sri Lankan native-language speakers, were chosen as interviewers and trained to conduct the structured interview. They were made aware of the need for sensitivity while eliciting responses about traumatic experiences from the subjects. When the potential participants met the interviewers, they were first told of the study's objectives. They were informed that their participation was completely voluntary and confidential and would carry no rewards, and that their refusal or consent for participation would have no other material consequences. They were then asked to give consent to proceed to the interview phase. Our interviewers did not offer any medical advice, although they took efforts to facilitate medical care by referring participants to local physicians or hospitals whenever a need was identified. Face-to-face structured interviews were conducted during the day in private areas of the participants' shelters, and lasted up to 70 minutes each.
The survey instruments were translated from English to Sinhalese and then back-translated to English for verification before their administration. Human subjects' research approval for this study was obtained from the Griffin Hospital Institutional Review Board in the US and the Ministry of Health in Sri Lanka. Approvals and support were also obtained from local public health officials and community leaders from the places visited.
Statistical Analysis
Data was entered using Microsoft Excel and then imported to SPSS version 14 (SPSS Inc, Chicago) for analysis. Demographic characteristics were examined in the total population and by sex. For categorical variables, frequencies were used, and for the continuous and ordinal variables means were calculated. Males and females were compared by χ2/cross-tabulations and Fisher exact test for binary variables and analysis of variance for continuous variables. Prevalence of PTSD, its components, and depression were examined in the total study sample and in each sex.
Binary logistic analysis was used to determine the impact of the theoretically possible independent variables in predicting PTSD. All of the variables that were relevant or P < .05 in bivariate analysis was used in the multivariate model. Logistic regression with backward stepwise elimination and log likelihood ratios were used to obtain the best predictor model. This allowed the removal of explanatory variables that were not significantly associated with an outcome or those that did not change the odds ratio for more than 10%. Odds ratios and 95% confidence intervals were generated. Significance level was interpreted at the P < .05 level for this study
RESULTS
Demographics, Disaster Experience, and Self-rated Health
Our study population was among the most affected segments (100% of the population lost their properties partially or completely) of the population and living in temporary shelters set up by the Sri Lankan government at the time of the interview. Of the 273 people who were asked to participate, 264 consented to be interviewed (97% participation rate). Table 1 displays the demographics and socioeconomic status of the sample. Study subjects were 103 (39%) males and 161 (61%) females. Mean age of 38 years (standard deviation 14.5) of the sample was also the mean age for both males and females. Most subjects were married (81%) and were parents (73%). Most (90%) of the participants were Buddhists. A large proportion had left school after grade 10 (65.5%) and 19% had <10 years of schooling. A large percentage (65%) declared an occupation before the tsunami, and this was reduced to 27% after the tsunami, indicating a 37% drop.
TABLE 1 Demographic Information by Sex

Most of the study population (88%) was close to the ocean at the time of the tsunami. A large proportion (62.5%) of the sample lost ≥1 family members or close relatives. In the sample 28% had received some sort of physical injury, and 62% had attended ≥1 counseling sessions conducted by a local or foreign-based group. Average self-rated health in this study sample significantly decreased from 3.92 before the tsunami to 3.05 after the tsunami (P = .024). Females in the study reported lower mean scores for current self-rated health than males, as well as greater declines from before-tsunami to after-tsunami self-rated health. The self-reporting by females of repetitive thinking of tsunami events was higher to a statistically significant degree as compared with males. Mean social support score in this study population was 24 out of a possible 35.
Females and males did not differ significantly in age, religion, loss of property, loss of family members, physical injuries, education level, marital status, distance from the ocean at the time of the tsunami, amount of social support, and exposure to counseling since the tsunami. None of our participants reported previously diagnosed psychiatric conditions.
Prevalence of PTSD, Diagnostic Criteria, and Depression
In the study sample 147 (56%) individuals currently showed symptom profiles diagnosed as PTSD. As expected, females showed a higher level of prevalence (63.7%) than males (41.7%), and they had at least twice the risk for experiencing PTSD (χ2 10.23 and OR 2.27, 95% CI 1.37–3.76; P = .002 [Table 2]).
TABLE 2 Prevalence of PTSD, Its Components, and Depression Among Males and Females

Table 2 shows the prevalence of different components of diagnostic criteria for PTSD in this population. Reexperiencing the event was high, with 94% prevalence among males and females. Avoidance symptoms were present in 63% of the sample and hyperarousal symptoms were present in 81%. Females were significantly more likely than males to report avoidance symptoms and hyperarousal symptoms.
In the total study population 182 (69%) were positive for symptoms of depression, of which 117 (73%) were females and 65 (63%) were males. This difference was not statistically significant. When we examined the actual CES-D score difference between males and females, however, females did show a higher score than males to a statistically significant extent.
Risk Factors for PTSD
Table 3 shows multivariate logistic regression of the full model with relevant covariates. Posttraumatic stress disorder being the outcome, predictor variables were age, marital status, being a parent, loss of family members, distance from the ocean, self-reported current health, amount of social support, sex, education level, and depression. Only sex, education level, and depression had a significant association with PTSD.
TABLE 3 Risk Factors for PTSD (Multivariate Modeling), Full Model

Table 4 shows the adjusted multivariate logistic regression after backward elimination. Sex, education level, and depression had a significant association with PTSD and were kept in the final model. Females were twice as likely as males to show PTSD symptoms after adjusting for other variables (adjusted OR 214, 95% CI 1.21–3.80; P = .009). Lower education level was found to be marginally protective for PTSD, although with a wide confidence interval. People who left school at grade 10 or earlier had a slightly less risk for PTSD than those who studied beyond grade 10. Presence of depression was a significant predictor for PTSD. People with depression had >7 times the risk for PTSD than the people who were not depressed (OR 7.19, 95% CI 3.83–13.52; P < .001).
TABLE 4 Risk Factors for PTSD (Multivariate Modeling), Best Predictor Model

Risk Factors for Depression
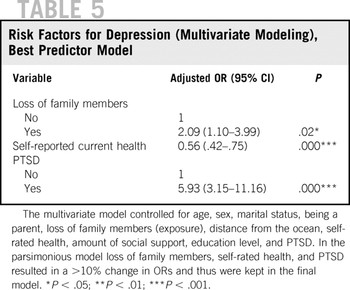
Table 5 shows the adjusted multivariate logistic regression with backward elimination in which depression is the outcome after adjusting for age, marital status, being a parent, loss of family members, distance from the ocean, self-reported current health, amount of social support, sex, education level, and PTSD. Self-rated current health, loss of family members, and PTSD had a significant association with depression.
TABLE 5 Risk Factors for Depression (Multivariate Modeling), Best Predictor Model
DISCUSSION
The tsunami of 2004, an event of extraordinary destruction, provides an observational window into the psychological effects of a major natural disaster on an unsuspecting population. PTSD is found to be correlated with negative outcomes such as marital instability, work impairment, unemployment, and increased use of outpatient care, which points at the burden to the society.Reference Kessler19 Although it is impossible to compare across different disaster events or study samples as discussed below, prevalence data remain a useful measure of trauma impact. Our results for PTSD prevalence among study subjects at 56% are higher than previously reported results for adult victims of this tsunami (12%–19% Reference Wickrama and Kaspar20–Reference van Griensven, Chakkraband and Thienkrua22). In other high-impact natural disasters such as earthquakes and floods where data are available, PTSD prevalence has varied from 15% to 67%,Reference Goenjian, Najarian and Pynoos23 although most of the studies have found prevalence rates between 15% and 40% range.Reference Cao, McFarlane and Klimidis24–Reference Sharan, Chaudhary, Kavathekar and Saxena29
The relatively high prevalence of PTSD in the present study may be related to the fact that these subjects may have been among the worst-affected survivors of the disaster, with 100% of the subjects reporting a significant loss of family, relatives, or possessions. This level of loss may not be representative of all of the victims of a massive and widespread disaster. In a disaster on this scale that exposes a large population to a shared trauma, it is difficult to categorize exposure levels and identify direct victims in a consistent manner.Reference Norris, Friedman, Watson, Byrne, Diaz and Kaniasty30 The wide range of exposure levels experienced by victims of natural disasters may explain some of the differences in prevalence rates across natural disasters and may make some contribution to the observation that natural disasters collectively report lower prevalence levels as compared with manmade disasters, in which victims may be more easily identified.Reference Galea, Nandi and Vlahov31
Another factor that may have affected prevalence data of PTSD in the present study is the use of a 2-point scale for recording responses on the PSS-I scale; this may have influenced self-reporting on some level. Similarly, there is a possibility that these results were also influenced by differences in self-reporting patterns between sexes (although it has been shown to be negligible for some populations),Reference Bogner and Gallo32 but our sex-uniform findings for depression prevalence suggests this may have been minimal for PTSD. Other factors, such as incidental stresses resulting from living conditions at the refugee camps, a greater risk for sexual harassment for women in confined living quarters, changes in substance abuse behavior, and ongoing uncertainty about material security, may have contributed to the psychological stress experienced by subjects.
Multivariate analysis also showed that females in this study were at a higher, approximately 2-fold increased risk of experiencing PTSD symptoms than males 6 months after the trauma. This higher risk in females has been demonstrated repeatedly in the scientific literature regardless of the type of the study, population, type of assessment, and other methodological variables.Reference Tolin and Foa10 The results obtained in this study confirm the previous findings and the need for greater public health outreach toward women in the aftermath of a disaster.
This study also shows that the reexperiencing and hyperarousal symptoms are much higher than avoidance symptoms for both males and females, a result that is consistent with previous studies,Reference McMillen, North and Smith33 and that females also reported statistically significant higher scores than males for avoidance and hyperarousal symptoms. This breakdown of symptoms, although not sufficient by itself, can be useful in structuring interventions, such as cognitive-behavioral therapies in treating people with PTSD.
The prevalence of depression in the study population was 68.9%, which is higher than the rates of depression after a natural disaster reported in previous studies. Reference Van Griensven, Chakkraband and Thienkrua34–Reference Chou, Su, Chou, Ou-Yang, Lu and Chien36 This higher rate may be a result of the atypical level of exposure in this population along with the same predisposing environmental factors as that for PTSD. The authors found that symptomatic scores for depression (CES-D scores) were higher in females compared with males, indicating a greater level of impairment in female disaster victims. It has been shown that females are more likely than males to be influenced by the perceptions of family members when reporting depressive symptoms, and this factor also may need to be considered when planning interventions in family settings.Reference Brommelhoff, Conway, Merikangas and Levy37 Depression is known to carry greater functional impairment in people with PTSD,Reference Foa, Stein and McFarlane6 and therefore it is important that this condition be addressed by health professionals who are knowledgeable about the effects of the comorbidity of depression and PTSD.Reference Vieweg, Julius, Fernandez, Beatty-Brooks, Hettema and Pandurangi38
After adjusting for other covariates, education level as defined by the number of years of schooling has a statistically significant relationship to PTSD. Subjects with 10 years or fewer of schooling were less likely to experience PTSD symptoms. This result appears to contradict the previously reported finding that socioeconomic status, including education level, is protective for psychological distress.Reference Norris, Friedman, Watson, Byrne, Diaz and Kaniasty30, Reference Armenian, Morikawa and Melkonian39 This result may be weakened by the fact that nearly two thirds of the sample belonged to just 1 category, those with 10-years of schooling, and the other 2 categories had small numbers of individuals, which led to wider confidence intervals. Sri Lanka has a relatively high literacy rate (90.7%) and women generally enjoy parity in education,40 therefore, overall socioeconomic status may be too homogenous in this particular sample for education level to have a measurable impact. Further study is necessary to draw conclusions about the influence of education and other culturally specific factors such as religion on PTSD.
In this study commonly known risk factorsReference Norris, Friedman and Watson5, Reference Galea, Nandi and Vlahov9 such as level of exposure, measured by distance from the ocean and the loss of family members, amount of social support, and family structure were not found to be significantly associated with PTSD. This may be due to the overall higher prevalence of PTSD and the uniformly high level of exposure in the sample. Also of note is the average social support score of 24 out of 35 in the population, indicating the presence of a support base for these tsunami victims. This suggests an additional factor that can be incorporated into the recovery efforts.
Our results showed no association between PTSD and history of psychological counseling, which 62% of our subjects had received in some form while they were living in the camps; this may suggest a level of difficulty in planning psychosocial interventions after a disaster. The study locations the authors visited had an established public health infrastructure, consisting of free government facilities and other providers, even before the disaster. Even with a high level of interest shown by concerned government agencies, mental health services remained inadequate after the disaster mainly because of the limited availability of trained mental health professionals. This gap was sometimes filled by local and foreign nongovernmental organizations, who often ran into cultural and logistical difficulties.41, Reference Chandra, Pandav and Bhugra42 Research and intervention practices that do not take into account local variations and existing capacities often raise questions about their ethical merit and ultimately prove unsatisfactory from the perspective of the affected populations,Reference Sumathipala and Siribaddana43 which highlights the importance of proper management of postdisaster psychosocial support systems that incorporate existing local conditions from the outset.
Other Strengths and Limitations
A large sample size with a high participation rate, a geographically dispersed population, minimal interviewer bias due to native language speakers, and the use of the validated CES-D scale strengthens the results of this study. This was a cross-sectional study using convenience sampling, which has an inherent potential to bias results. The authors attempted to mitigate this bias by recruiting subjects from a wide range of camps with representative populations. The comprehensive questionnaire, which took about 70 minutes, could have induced survey fatigue. Interviewers, however, consistently reported enthusiasm for participation by the subjects, reflected in the high participation rate, which may be attributed to the particular cultural setting of the study. The study subjects were not offered any reward for participation for fear of biasing the outcome in the confined environments of the camps. The surveys were carried out during the daylight hours from 8 am to 7 pm to minimize selection/participation bias because otherwise, subjects who were already were too distressed to travel outside may have been overrepresented. Another limitation the authors faced in evaluating the data is the lack of predisaster mental health statistics for PTSD for this population; the authors used self-rated health before the tsunami as a covariate. To minimize reporting bias encountered in cross-sectional studies, the authors used structured interviews in a uniform fashion while maintaining privacy during the interviews.
CONCLUSIONS
The results of this study suggest that PTSD is highly prevalent among subjects affected by the tsunami in Sri Lanka at the 6-months postdisaster interval, a time when some of the chronic and delayed-onset impairment may be present. Females especially are at higher risk than males for PTSD symptoms. Depression prevalence is also high in this group and it is an independent predictor of PTSD, suggesting a high level of comorbidity in these 2 debilitating psychological problems that are commonly seen after a widespread natural disaster.
Knowledge about risk factors for PTSD, especially the gender-influenced vulnerabilities in the symptom profiles of PTSD, will aid in identifying groups that are in greater need of systematic psychiatric interventions and will help in designing treatments for specific impairments. Ideally, longitudinal studies comparing different treatment options will need to be attempted to gauge their effectiveness in this population, requiring at a minimum a high level of empirical input from practitioners. To achieve an effective level of evidence-supported treatment practices, greater collaboration between practitioners and researchers has been advocated.Reference Norris, Friedman and Watson5 The findings of the present study will help other researchers to design prospective studies examining the long-term public health impact of disasters in these communities. This will help build a knowledge base for public health practitioners to effectively address the psychological consequences of disasters and to prepare for predisaster mental health planning.
Acknowledgments
Financial support for this study was made possible by a Stolwijk Fellowship from the Yale School of Public Health and a travel grant from the Griffin Center for Health and Human Rights, awarded to the first author. The authors wish to acknowledge Ramin Ahmadi, MD, MPH, Director, Griffin Hospital Internal Medicine Residency Program, for guidance in data gathering: Lisa Calvocoressi, PhD, Yale School of Public Health, for feedback on an earlier draft; and Pubudu Ranasinghe for assistance in editing. The authors are grateful for permission and support at the sites for the Ministry of Health of the Government of Sri Lanka, and all of the participants and local coordinators at the shelters who made the study possible.





