Various types of disasters and mass casualty incidences (MCIs) occur all over the world, namely chemical, biological, radiological, nuclear, and explosive events, as do conventional events including traffic accidents, fire accidents, mass gatherings, and natural catastrophes. 1 They tend to result in a high mortality of victims despite the availability of valuable medical resources in the affected area, unless they are adequately prepared.Reference Kuisma, Hiltunen and Maatta 2
The prehospital response time (PRT) delay is the crucial cause for treatment delay, related to the poor outcome for patients with multiple severe trauma, as well as for those with cerebrovascular diseases including stroke, myocardial infarction, and, ultimately, presumed cardiac arrests, which have a time window for carrying out the optimal definitive treatment.Reference Yanagida, Fujimoto, Inoue and Suzuki 3 , Reference De Luca, Suryapranata, Ottervanger and Antman 4 The PRT delay, especially, is well known to be one of the potent factors affecting the survival of out-of-hospital cardiac arrest (OHCA) patients.Reference Eisenberg, Bergner and Hallstrom 5 The PRT delay is well known to occur in MCIs according to many studies.Reference Park, Shin, Song, Hong and Kim 6 – Reference Martin, Lohse and Sztajnkrycer 9 In a previous study, the PRT of emergency medical services (EMS) was 2.5 times longer during MCIs compared with that during non-MCIs.Reference Schenk, Wijetunge, Mann, Lerner, Longthorne and Dawson 10 In addition, victims and even patients unrelated to MCIs had a longer waiting period for admission into receiving hospitals compared with the reference patients in non-MCIs.Reference Abir, Choi, Cooke, Wang and Davis 11
However, a previous study reported the PRT delay by simply comparing the response time in MCIs with that in non-MCIs, in which the spillover effect of MCIs could not be considered in the prehospital setting. Thus, on the basis of the hypothesis that PRT might also be delayed for usual emergency patients unrelated to MCIs in events of concurrent mass casualties due to the lack of EMS resource, we investigated the impact of MCIs on PRT by comparing the PRT of non-MCI-related emergency patients before and after MCI occurrences.
METHODS
Study Settings
The size of the territory of South Korea is ~99,720 km2, with a population of 51 million people. It consists of 8 provinces called “Doh”, similar to states in the United States. Each province is divided into municipal administrative areas called “Gu,” “Si,” and “Gun,” similar to counties in the United States. According to the population size, municipal counties (Gu) are segmented into administrative areas of the metropolitan city (eg, Seoul) with populations of more than ~500,000. The urban counties (Si) have populations of more than ~100,000, and the rural counties (Gun) have populations of less than ~100,000. Korea has 102 municipal, 66 urban, and 83 rural counties, and the median population sizes and population density were 50,220,000 residents and 501 persons/km2, respectively, in 2013. 12 Every county has municipal authorities and duties to serve the population of its jurisdiction to manage health-care issues.Reference Ro, Shin and Song 13
The Ministry of Public Safety and Security (MPSS) offers EMS to Korea and is dedicated to the management of various MCIs through the fire department-based system.Reference Ro, Shin and Song 13 This EMS system has 17 regional headquarters of the fire department with ~40,500 EMS providers and 1350 advanced ambulances providing single basic life support (BLS), basic trauma life support (BTLS), and two-tiered advanced life support (ALS) in certain areas to manage disasters and MCIs occurring throughout Korea.Reference Kim, Kim, Shin, Lee, Park and Sung 14 A single fire station is designated to operate EMS and MCI responses, covering 1 or 2 municipal administrative areas called “Gu,” “Si,” and “Gun.” In case of MCIs or disasters, the MPSS dispatches fire and EMS units not only from the affected municipal administrative area but also from the area nearest to the MCI.
Study Design
This study was a retrospective serial cross-sectional analysis based on MPSS administrative data from 2009 to 2013.
Participants
We enrolled all EMS-treated patients who were unrelated to the MCIs but were treated in the same affected municipal administrative area (“Gu,” “Si,” and “Gun”) within 3 hours before and after the MCIs.
We distributed these patients into 4 emergency patient groups according to the definition below.
OHCA Group: A patient whose chief complaint was coded as cardiac arrest or respiratory arrest in the EMS databaseReference Ahn, Shin and Suh 15 ; patients who received cardiopulmonary resuscitation during the transport were also included.
Severe Trauma Group Reference Lee 16 : Patients with non-presumed cardiac arrest, non-disease, and/or unstable vital signs including systolic blood pressure <90, respiration rate <10 or >29, and non-alert mentality.
Suspected Stroke Group Reference Lee 16 : Non-traumatic patients aged over 15 years with a chief complaint of headache, altered mentality, motor weakness, dizziness, or syncope. Patients were coded as suspected stroke in the EMS database.
Chest Pain Group Reference Lee 16 : Non-traumatic patients aged over 15 years with a chief complaint of chest pain.
Dyspnea Group Reference Lee 16 : Non-traumatic patients aged over 15 years with a chief complaint of difficulty in breathing, such as shortness of breath, exertional breath, or breathlessness; patients treated with oxygen, a nebulizer, and/or a bronchodilator.
Definition of MCIs
The definition of MCIs varies between researchers, research institutes, and countries. However, no international standardized definition exists for disasters and MCIs. Thus, on the basis of the Korean studies on terminology, feasible definition, and epidemiologic indices for disasters and MCIs,Reference Kim, Park, Park, Kim, Kim and Hong 17 an MCI was defined as an incident that involves more than 6 casualties, regardless of the affected area or number of deaths.
Definition of Time Interval
The PRT was defined as the time from call to arrival to the scene.
Data Source and Collections
Data were collected from ambulance-run sheets from January 1, 2009, to December 31, 2013, from the electronic EMS databases of MPSS, which is the national headquarters of fire departments. Ambulance-run sheets had patients’ general characteristics (sex, age, occupation, the scene address, etc.), medical status (chief complaint, vital signs, physical examination, etc.), prehospital medical treatment, and time intervals (call time, arrival time to the scene, arrival time to the receiving hospital). Collection and analysis of the data for this study was approved by the institutional review board.
Outcome Measure
The primary outcome was the comparison of the PRT of non-MCI-related emergency patients within 3 hours before and after MCI occurrences. To verify how long the spillover effect of MCIs lasted, we categorized them into subgroups such as 1 hour after MCIs, 1-2 hours after MCIs, and 2-3 hours after MCIs according to the elapsed time from occurrence.
The secondary outcome was the identification of the significant factors that caused the PRT delay after MCIs.
Statistical Analysis
Continuous data are presented as means ± standard deviation. The primary outcome is shown as mean and 95% CI. To compare the primary outcome between the reference group and the different subgroups, we used multiple linear regression analysis with correction for age, sex, population size (metropolitan versus urban), time of the day (6 am to 6 pm versus 6 pm to 6 am), time of the week (weekend versus weekdays), and the MCIs scale (number of patients =6 versus number of patients >6). P-value <0.05 was considered significant. For non-parametric, dichotomous data the χ 2 test was used.
The proportional single imputation method was used to manage the missing data of “sex” in 27 cases and “age” in 39 cases. The software SAS version 9.3 was used as the statistical analysis tool.
RESULTS
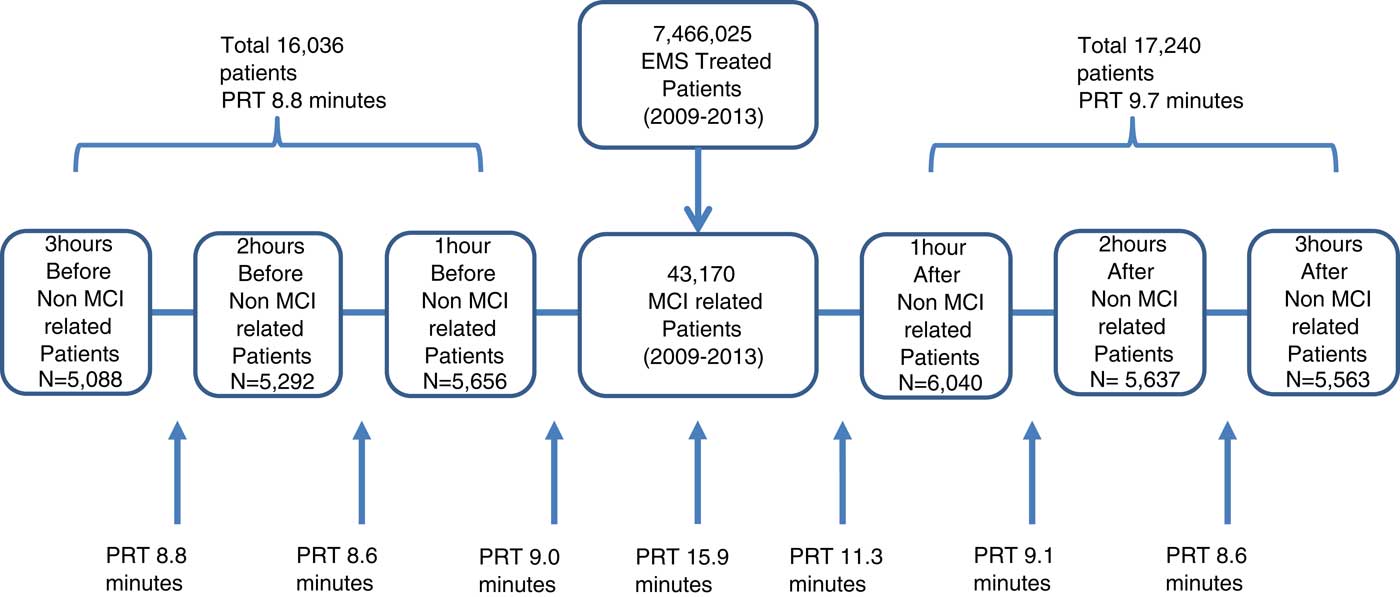
From 2009 to 2013, 7,466,025 patients were EMS treated. Of them, 43,170 patients were MCI related. A total of 33,276 non-MCI-related and EMS-treated patients were matched within 3 hours before and after MCI occurrences. Of 33,276 matched patients, 16,036 patients were classified into groups 3 hours before MCIs and 17,240 patients into groups 3 hours after MCIs, who were further categorized into 6040 patients of “1 hour after MCIs” subgroup, 5637 patients of “1-2 hours” after MCIs subgroup, and 5563 patients of “2-3” hours after MCIs (Figure 1).

Figure 1 Enrollment and Distribution of Participants. Abbreviations: PRT, prehospital response time; EMS, emergency medical service; MCI, mass casualty incident.
The average PRT for MCI-related emergency patients was 15.9 minutes±15.3 and the median was 12 minutes (7-20 minutes). The average PRT for non-MCI-related emergency patients within 3 hours before MCIs was 8.8 minutes± 8.2, which was used as the reference value. It was 11.3 minutes in the subgroup of 1 hour after MCIs (P<0.01), 9.1 minutes in the subgroup of 1-2 hours after MCIs (P<0.01), and 8.6 minutes in the subgroup of 2–3 hours after MCIs (P=0.13) (Figure 1).
The total number of MCI cases was 5304. In August, the maximum number of MCI cases (4360 cases, 10.1%) occurred. During the daytime (6 am to 6 pm), 28,720 cases (66.5%) of MCIs occurred (Table 1).
Table 1 Demographics of Patient-Related Mass Casualty Incidences (MCIs) and Non-MCIs

Abbreviations: EMS, emergency medical service; OHCA, out-of-hospital cardiac arrest
The multiple linear regression analysis revealed that PRT of all enrolled non-MCI-related patients increased significantly by 2.5 minutes (95% CI: 2.3-2.8) during the first hour after MCIs and also increased significantly by 0.3 minutes (95% CI: 0.1-0.6) during the second hour after MCIs (Table 2). In the 4 emergency patient groups’ analysis, the PRT of the OHCA group was delayed by 3.2 minutes (95% CI: 1.6-4.7) during the first hour after MCIs. The PRT for the suspected stroke group was also delayed by 2.0 minutes (95% CI: 1.3-2.6) during the first hour after MCIs, and by a further 0.7 minutes (95% CI: 0.1-1.4) during the second hour after MCIs (Table 3). In the chest pain group, no PRT delay was shown. In all emergency patient groups there was no PRT delay during the third hour after MCIs (Table 3).
Table 2 Prehospital Response Time in Events of Concurrent Mass Casualty Incidences (MCIs)

Abbreviation: OHCA, out-of-hospital cardiac arrest.
a Adjusted variable: gender, age, weekend/weekday, population size (metropolitan versus urban), time of the day (6 am to 6 pm versus 6 pm to 6 am), time of the week (weekend versus weekdays), and MCI scale (the number of patients =6 versus the number of patients >6).
Table 3 Prehospital Response Time According to Emergency Types of Concurrent Non-MCI-Related Patients

Abbreviations: MCI, mass casualty incident; OHCA, out-of-hospital cardiac arrest.
a Adjusted variables: gender, age, weekend/weekday, population size (metropolitan versus urban), time of the day (6 am to 6 pm versus 6 pm to 6 am), time of the week (weekend versus weekdays), an MCI scale (the number of patients =6 versus the number of patients >6).
In the multiple linear regression model, population size (P<0.01), time of the day (P<0.01), time of the week (P<0.01)), and MCI scale were significant factors that delayed the PRT.
DISCUSSION
It is necessary to place human and medical resources at the scene when an MCI occurs for timely response, in the absence of which MCIs can cause extensive and progressive damage in the community. Although it is essential to assess available resources and allocate them adequately according to the needs of the scene, the diversity and harshness of the circumstance of MCIs make it difficult. Failure in allocating the resource could waste valuable resources that might be necessary for immediate response to MCIs. Thus, prediction of the impact of MCIs on PRT would be useful for efficiency in allocation.
In this study, we intended to verify the PRT delay of non-MCI-related EMS-treated patients in the same areas as the MCIs. The spillover effect of MCIs could impact the PRT after MCIs and could last for 2 hours after MCIs. Even in the OHCA group, PRT delay had existed during the first hour after MCIs. The PRT delay could directly impact the survival of OHCA patients in events of concurrent MCIs because early BLS plays a key role in the survival of OHCA patients.Reference Eisenberg, Bergner and Hallstrom 5
Mahshid et al reported that MCI-related patients had a longer stay in the hospital than non-MCI-related patients, and also had higher hospital charges. Even non-MCI-related patients had a longer stay and higher hospital charges, similar to MCI-related patients, if they visited 1 week before and after MCIs.Reference Abir, Choi, Cooke, Wang and Davis 11 They analyzed this phenomenon as a “spillover” effect representing a lack of efficiency in the allocation of hospital resources due to the surge in admissions from the MCIs.Reference Abir, Choi, Cooke, Wang and Davis 11 In this study, we investigated the impact of MCIs on significantly delayed PRT. We believe that this delay would be a reflection of the disparity of resource allocation between patients, finally causing harmful damages to non-MCI-related patients. Therefore, measurement of the disparity of resources is mandatory in the predicted area. For example, EMS agencies must have a backup plan to support the nearby area where significant PRT delay might happen.
Several definitions can be applied to MCIs. Mahshid et al applied the MCIs definition of any event with a surge in patients occupying more than 5% of the baseline bed capacity of the hospital.Reference Abir, Choi, Cooke, Wang and Davis 11 In another study, an MCI was defined as an event in which there were more than 3 patients with Injury Severity Score more than 12 points within a maximum of 3 hours. We applied the definition of a previous study in which an MCI was defined as an incident that involves more than 6 casualties, regardless of the affected area or number of deaths.Reference Kim, Park, Park, Kim, Kim and Hong 17 Application of a different definition has the possibility of different demographics and characteristics of MCIs. However, we tried compensating for this limitation by analyzing the PRT according to the MCI scale in order to verify the effect.
Because of the retrospective evaluation of MCIs, there could be a recording bias in EMS data, especially in the time intervals. Although we analyzed the PRT correcting for age, sex, population size, time of the day, time of the week, and MCI scale, there could be another variable to be corrected for such as patient individual factor, traffic factor, and so on.
CONCLUSIONS
We investigated the impact of MCIs on PRT compared with that for non-MCI-related patients before and after MCI occurrences. We verified that the spillover effect of MCIs could impact the PRT after MCIs and, in our study, it could last for 2 hours after MCIs.
Support
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of Interest
The authors declare that there are no conflicts of interest in this study.