Government reports persistently indicate the intent of terrorists and hostile nations to acquire and “weaponize” nuclear materials to use in deliberate attacks on major US metropolitan cities. In response to this threat, cities’ preparedness efforts have largely focused on building internal surge capacity within the existing health care infrastructure (ie, hospitals, clinics, health departments, trauma centers and systems). This has been built upon a pattern of urban economic development that typically concentrates hospitals, clinics, and medical personnel within metropolitan centers.
Ironically these factors indicate the rationale for cities’ vulnerability to nuclear detonation. Damage caused by a nuclear detonation in a major city will result in a disproportionate loss of medical resources.1, 2 A study of surviving medical resources following a nuclear attack on London concluded that <20% of hospital beds would be accessible, with some 150 candidates for each bed.Reference Clark, Ehrlich and Gunn3
Casualty Distribution
The surge of patients competing for these diminutive medical resources will include trauma, radiation, and burn elements, often in combination.Reference Brooks, Evans, Ham and Reid4 These casualty surges are daunting, and the possibility of thousands of burn victims at one time in one location presents unique challenges.
Burns in nuclear warfare can occur from direct thermal radiation on the skin or from the ignition of substances from direct thermal radiation. More than 90% of the burn victims of the nuclear detonations in Hiroshima and Nagasaki in 1945 received their wounds from direct radiation, also known as flash burns.Reference Glasstone and Dolan5 Direct radiation burned exposed human skin up to 4 km from the hypocenter.Reference Glasstone and Dolan5 Modern thermonuclear weapons will deliver direct radiation burns more than 10 km from the hypocenter of a 550-kiloton detonation in a major urban area.2 Experts estimate that mortality rates approaching 100% would result in people with thermal injuries involving >30% of their body surface areaReference Becker, Buescher, Cioffi, McManus and Pruitt6 because of the probable lack of comprehensive care.
Nuclear Detonation
When a nuclear weapon is detonated, the energy released is dissipated in 4 main ways: blast (40%–60%), thermal radiation (30%–50%), ionizing radiation (5%), and fallout radiation (5%–10%), depending upon the design of the weapon and the detonation environment.
Blast effects from the explosion cause the most damage to buildings: they rapidly push away the air surrounding the buildings, creating high winds that knock them down. At 4 psi overpressure, most residential buildings collapse, causing many injuries and deaths. Additional injuries or deaths can result from flying- or fixed-object impact. Research suggests that populations that are subjected to 2 to 5 psi experience 45% injuries and 5% deaths; populations that are subjected to 1 and 2 psi are injured mainly by flying glass and debris.7
Thermal energy, or thermal fluence, is typically measured in calories per square centimeter. Approximately one third of the total energy generated in a nuclear detonation will be emitted as heat, producing fireballs that reach temperatures in the millions of degree Centigrade (the magnitude of the sun).Reference Barnaby and Rotblat8 Thermal energy travels directly from the fireball unless it is scattered or absorbed. The intensity and range of thermal effects increase proportionally with weapon yield.2
At thermal fluencies above 10 cal/cm2 a nuclear detonation can start large fires in urban areas,Reference Eden9 although there is much debate about the level needed for mass fires.Reference Binninger, Hodge and Wright10–Reference Daugherty, Levi and Von Hippel13 When a nuclear weapon is detonated if the resulting fireball is below the cloud cover, the thermal effect can double,Reference Eden9 or in extreme circumstances, increase 5-fold.14 Clouds above the fireball significantly increase the reflection of the thermal radiation, resulting in fewer radiation “shadows” from buildings. This in turn increases burn casualties and enhances the probability of fire ignition. Even a few large clouds in the sky could greatly increase the probability of local fires starting.
Prompt or ionizing radiation occurs immediately after the detonation. Fatal doses occur at 1500 m from the blast epicenter for 20-kiloton devices and about 2500 m out for 550-kiloton devices. Ionizing radiation drops off rapidly with increasing radii from the epicenter. These distances are within the mass fire zone for both of the detonations in our study.
Fallout radiation creates a conical-shaped plume that is blown downwind from ground zero. Dispersion is greatly affected by turbulence in the atmosphere, which in turn mainly depends upon land use, topography, vertical temperature, and wind structure.
Previous Models
Beginning in the 1970s, Brode worked for more than 20 years on predicting fire damage from nuclear detonations; his later work examined fire modeling and spread.Reference Brode and Small15 EdenReference Eden9 looked at progress in fire modeling and spread, including the Nuclear Weapon Fire Start Model.Reference Craver, Martin and Bacon16 In the early 1990s, funding for nuclear fire modeling was withdrawn,Reference Eden9 but was restarted in the late 1990s. Around 2000, the Defense Threat Reduction Agency (DTRA) funded fire prediction modeling with a view to incorporating the models within a modern computer modeling package such as Hazard Prediction and Assessment Capability (HPAC).Reference Binninger, Hodge and Wright10
The intent of this study is to model the morbidity and mortality of thermal casualties presenting from a nuclear detonation in 2 major metropolitan cities. We concentrate on the thermal impact on casualties that are radial from the hypocenter, or detonation point. This study also examines the nature and number of casualties with combination injuries. We use the model of the downwind radiation plume mainly to focus on the challenge of reaching these casualties in these downwind areas.
METHODS
Brode’sReference Brode11 work as modified by BinningerReference Binninger, Hodge and Wright10 was used to calculate thermal fluence, using thermal fractions discussed by Northop.17 EM-118 and WE19 were used to calculate blast effects. Fallout radiation was calculated using DTRA’s HPAC V404SP4,20 with “urban effects” turned on. The ESRI ArcView program21 calculated affected populations from 2000 US Census block-level data for areas affected by thermal effects.
Study Area and Size of Weapon
Two of the four largest cities in the United States, Los Angeles and Houston, were selected. Two sizes of nuclear weapon were simulated: a 20-kiloton tactical nuclear weapon and a common 550-kiloton Russian arsenal weapon. A fission fraction of 1 was assumed for the 20-kiloton device and 0.8 was assumed for the 550-kiloton device. The 20-kiloton device was assumed to explode at 20 m above the ground, and the 550-kiloton device exploded at 1 m above the ground; visibilities in both cases were 20,000 m. Detonations that occur closer to ground level cause greater thermal effects, which are somewhat offset by lower downwind fallout radiation amounts.18
Affected Populations
Detailed daytime population distributions for Los Angeles and Houston were not available, so US Census Bureau data were used for both cities.22 The US Census Bureau estimates that Houston experiences an increase in daytime population over nighttime population of 403,313 people due to commuters (the highest value of all US cities), whereas Los Angeles has an additional daytime over nighttime population of 127,877.22 Most of these commuters work in the downtown areas (Figs. 1 and 2). The organization HoustonDowntown compiled detailed block-level data for the central business district,23 which allowed us to perform daytime population analysis for the 20-kiloton Houston scenario. For the other 3 scenarios, we used block-level Census data of nighttime populations for analysis and referred to additional daytime commuters where appropriate.

FIGURE 1 Nuclear detonations for Los Angeles, with June median winds

FIGURE 2 Nuclear detonations for Houston, with June median winds
When thermal or radiation boundaries split a block, percentage estimates were used to assign that block level’s populations. Populations are assigned to the respective thermal or radiation class based on class area within the block. People were added to the Census block-level data, yielding a better estimate of daytime population for the Houston 20-kiloton detonation. We do not believe that this method offered significant improvement to the 550-kiloton analysis because of the larger affected area (155 mi2) and lack of spatial detail for the daytime data outside the 2-mi2 central business district, which is contained entirely within the 38 cal/cm2mass fire zone. Consequently, we performed the Los Angeles scenarios using only nighttime block-level population data, used daytime estimates for the entire 20-kiloton Houston scenario, and performed only limited daytime analysis for the Houston 550-kiloton scenario.
Weather and Climate Data
The impact of nuclear detonation is strongly affected by weather and climate. Wind direction greatly affects the resulting fallout cloud. A median 3-dimensional climate model from 30 years of data for a typical day in June for Los Angeles and Houston was computed by the DTRA, which was supplied by data from the HPAC20 program. HPAC computed the fallout radiation impact of the 4 nuclear detonations (20 and 550 kilotons for each of the 2 cities). The data for Houston show lighter winds and wider plumes than Los Angeles. The directions of the plumes for the 20 and 550-kiloton detonations for the cities are not identical because the larger 550-kiloton fireball has a much higher dust cloud with different associated wind directions.
Because this study focuses on the distribution of thermal injuries rather than fallout radiation, it was necessary to use only a typical month of data to get an idea of the size of the part of the entire thermal circle that also includes those with fallout radiation injuries (fallout wedge: Fig. 1B, C wedge is to the west; Fig. 2B, C wedge is to the north and northwest, respectively). We chose a light wind city in June (Houston) and a medium wind city in June (Los Angeles) for modeling.
Thermal Effects
The thermal fluences that are necessary for the 3 possible degrees of burns were taken from Glasstone and Dolan (see their Figs. 12.64 and 12.65).Reference Glasstone and Dolan5 A fire’s possible level was taken from the calculations of Eden,Reference Eden9 in which 10 cal/cm2 is a good first estimate of the range out to which a mass fire could be expected in an attack with a weapon the size of that used in Nagasaki and Hiroshima in 1945. This would correspond to roughly 15 cal/cm2 for a 550-kiloton detonation after application of the relevant power law (see below).
Values roughly corresponding to those of Binninger were applied for both single-family frame housing and multistory steel/concrete structures for the mass fires probable and mass fires highly probable values in Table 1. The 550-kiloton mass fires values are 1.5 times higher than the 20-kiloton detonation according to the thermal fluence equation Q1/Q2 = (W1/W2)0.12, where W1 and W2 are the sizes of the 2 detonations in kilotons, and Q1 and Q2 are the respective thermal fluencies.Reference Binninger, Hodge and Wright10 Thermal fluence values for third-, second-, and first-degree burns are 7.6, 5.0, and 2.5, based on previous modeling work2 and 9.4, 6.2, and 3.1 cal/cm2 for the 20- and 550-kiloton detonations, respectively. The thermal fluence values in the mass fires highly probable category corresponds to slightly more than 90% probability of ignition, whereas the mass fires probable level corresponds to slightly more than 50% probability of ignition. The mass fires possible category from EdenReference Eden9 and PostolReference Postol12 would correspond to a probability of ignition on the Binninger scale of somewhere between 10% and 50%. With clouds present above the fireball, radiation could double, causing 10% fire ignition probabilities to become 50%, and 50% probabilities to become 90% due to the log-normal nature of the fire ignition probability distribution. Typical exposure proportions of affected population actually receiving first-, second-, or third-degree burns range from 1% to 25% of those affected,7, Reference Openshaw, Steadman and Greene24 with the recent National Planning Scenarios25 assuming 15% as a reasonable average, which we have used in our calculations.
TABLE 1 Level of Thermal Fluence Necessary for Fires From 20- and 550-kiloton Weapons


RESULTS
The 550-kiloton attack in downtown Los Angeles resulted in 786,000 thermal casualties. Of these casualties, >185,000 burn casualties would have survived (40,700 third degree, 45,896 second degree, and 101,019 first degree). Combined casualties totaled 237,000; 13,086 would have radiation exposure <300 rem and would be more likely to survive (the 9 population figures indicated by bold type in Table 4).
TABLE 4 Los Angeles Nighttime Population Affected by Thermal Radiation and Fallout Radiation in the Thermal Zone From a Typical 550-kiloton Nuclear Detonation in June

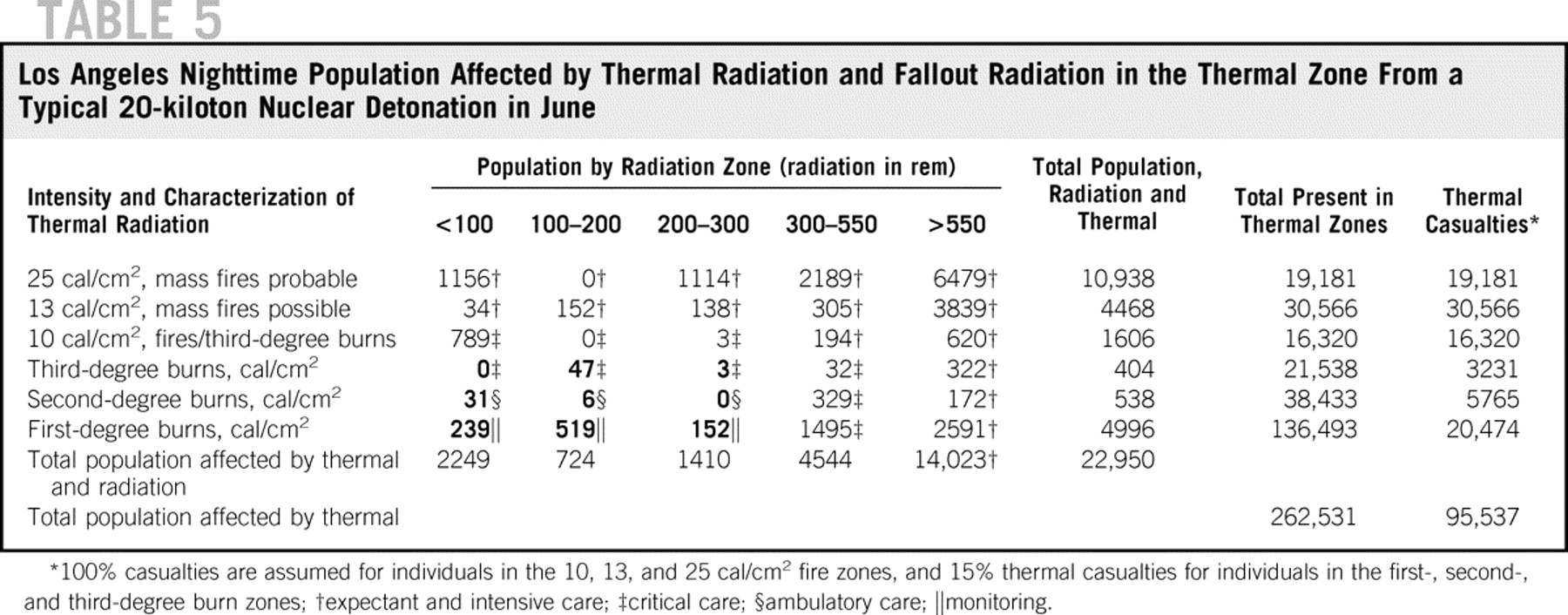
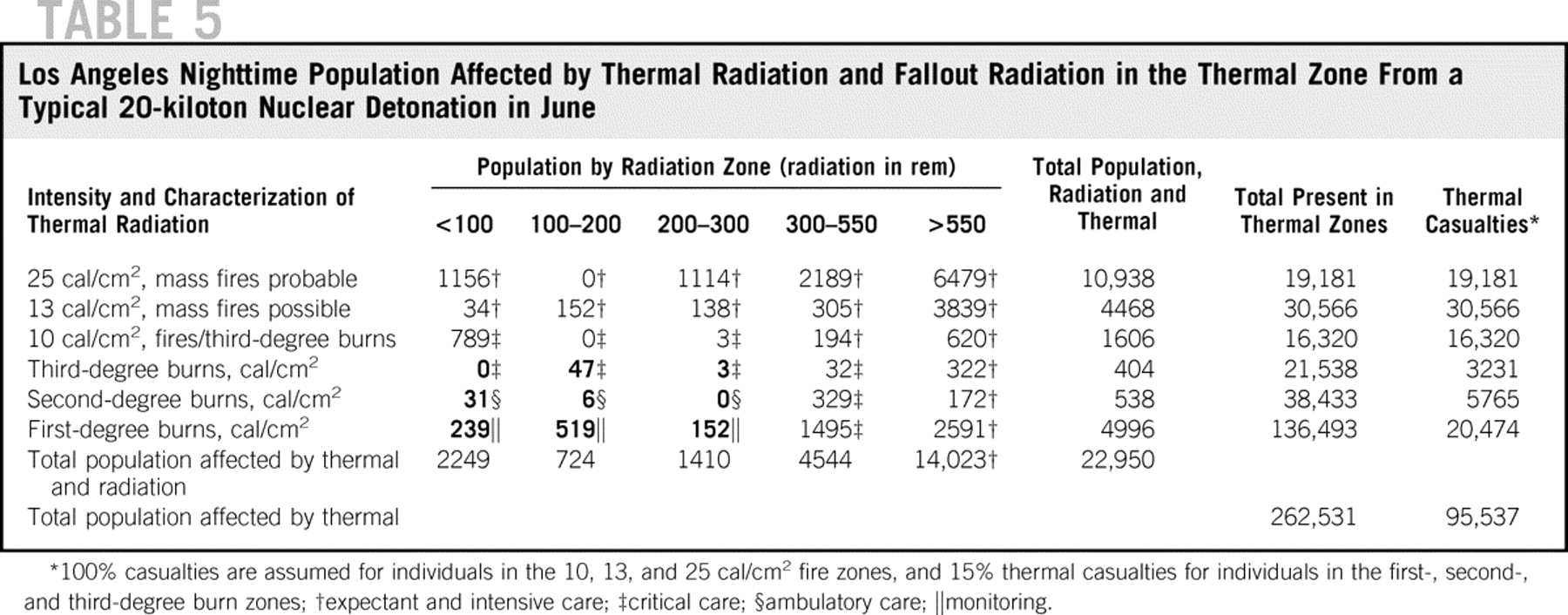
The 20-kiloton attack in downtown Los Angeles resulted in 95,537 thermal casualties. Of these casualties, >28,000 burn casualties would have survived (3231 third degree, 5765 second degree, and 20,474 first degree). Combined casualties totaled 22,950; 997 would have radiation exposure <300 rem and more likely survival (the 9 population figures indicated by bold type in Table 5).
TABLE 5 Los Angeles Nighttime Population Affected by Thermal Radiation and Fallout Radiation in the Thermal Zone From a Typical 20-kiloton Nuclear Detonation in June
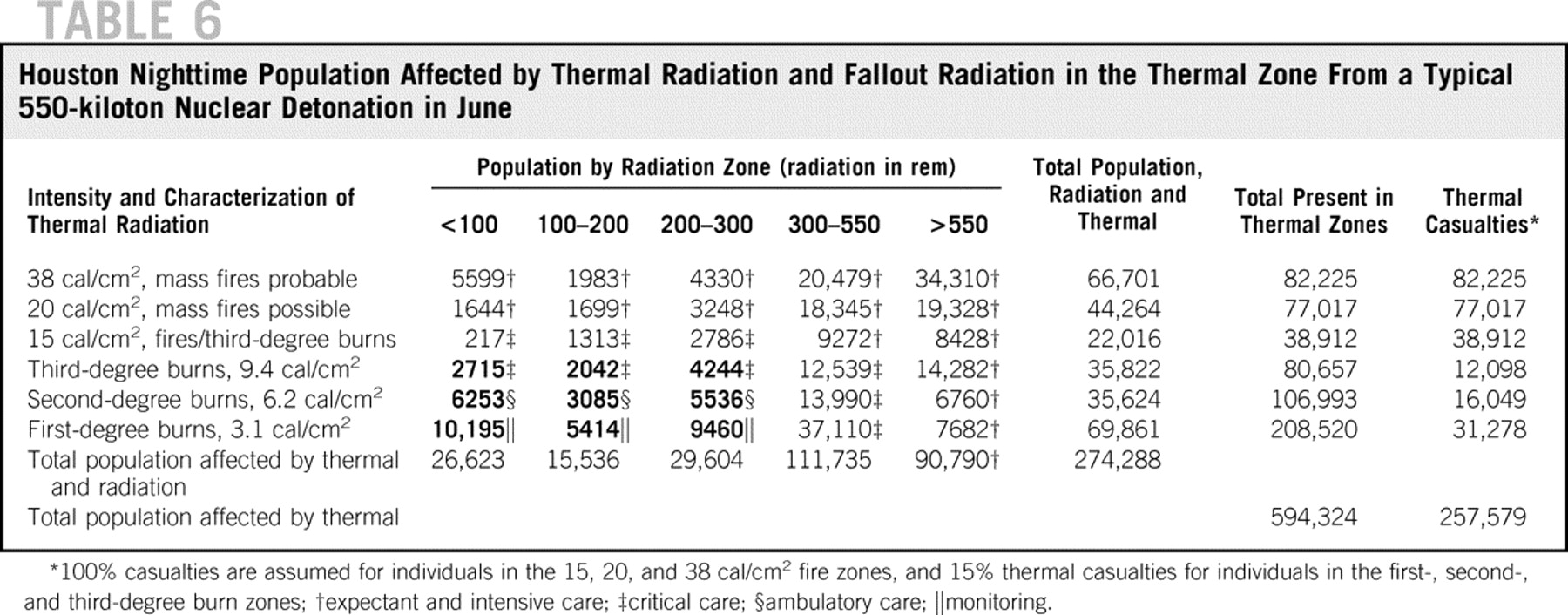
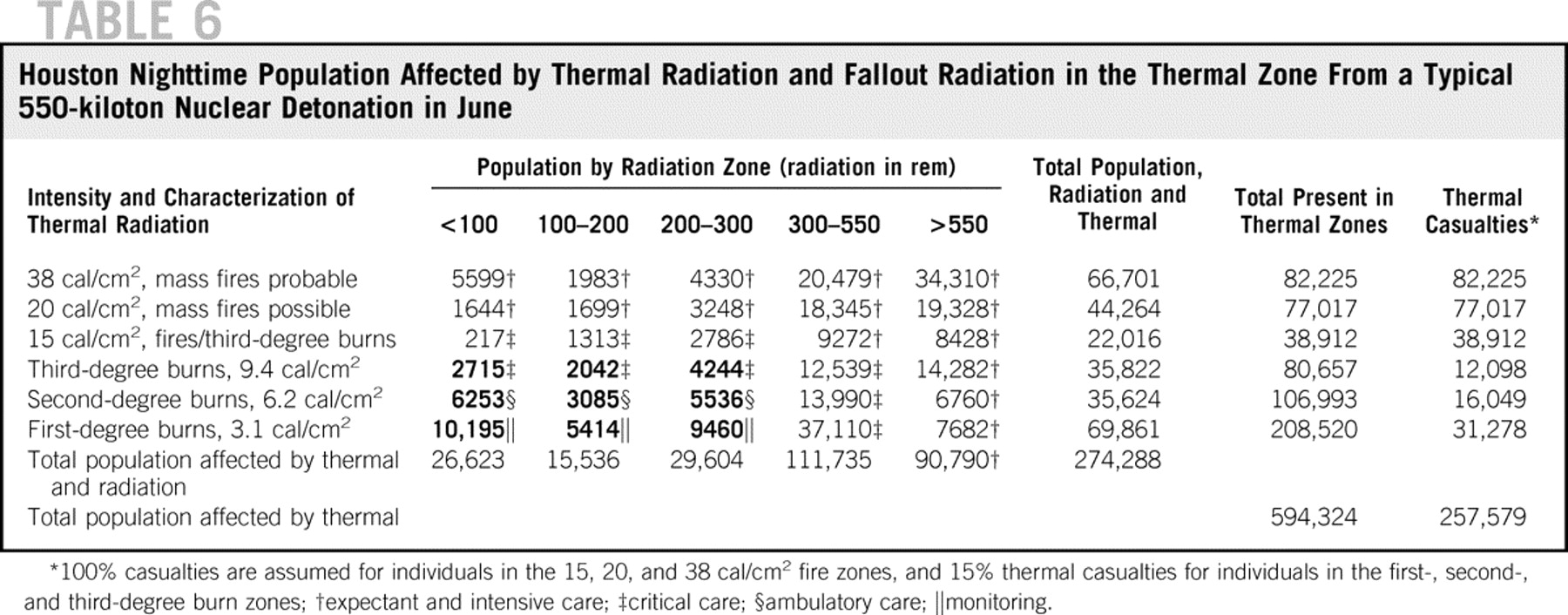
The 550-kiloton attack in downtown Houston resulted in 257,579 burn casualties. Of these, >59,000 burn casualties would have survived (12,098 third degree, 16,409 second degree, 31,278 third degree). Combined casualties totaled 274,288; 48,944 would have radiation exposure <300 rem and more likely survival (the 9 population figures indicated by bold type in Table 6).
TABLE 6 Houston Nighttime Population Affected by Thermal Radiation and Fallout Radiation in the Thermal Zone From a Typical 550-kiloton Nuclear Detonation in June
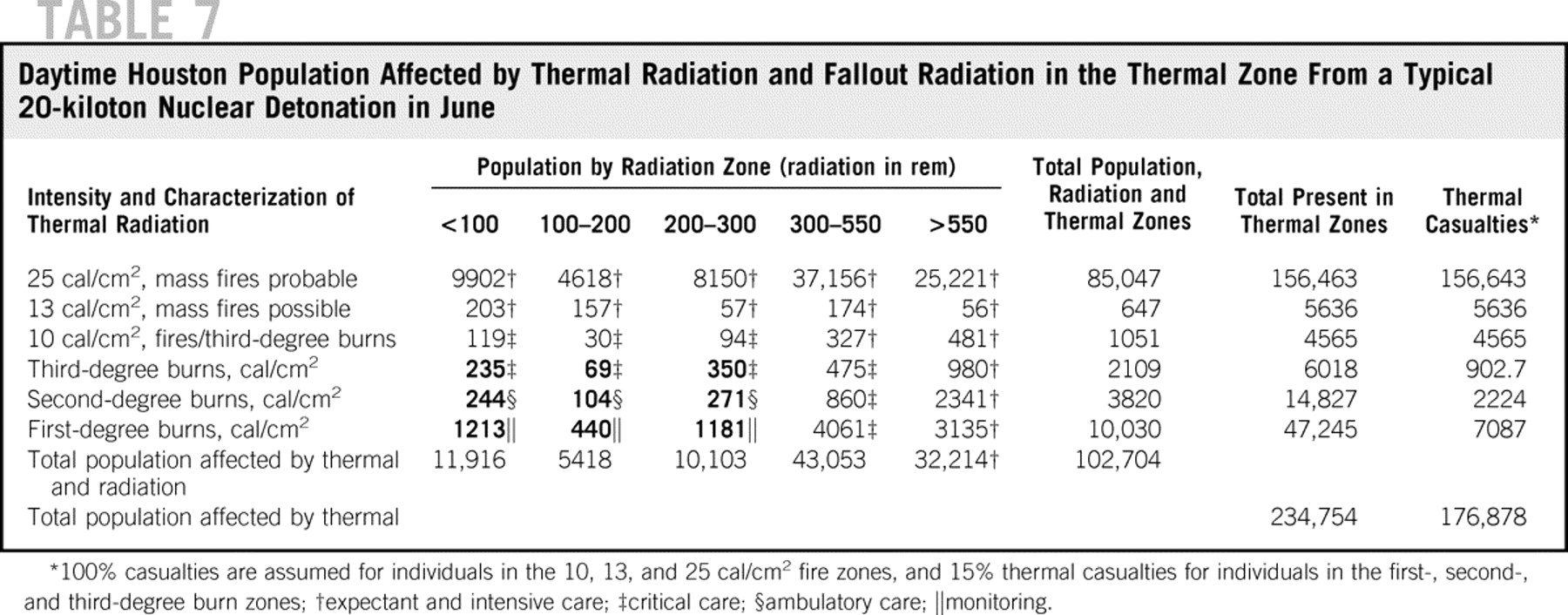
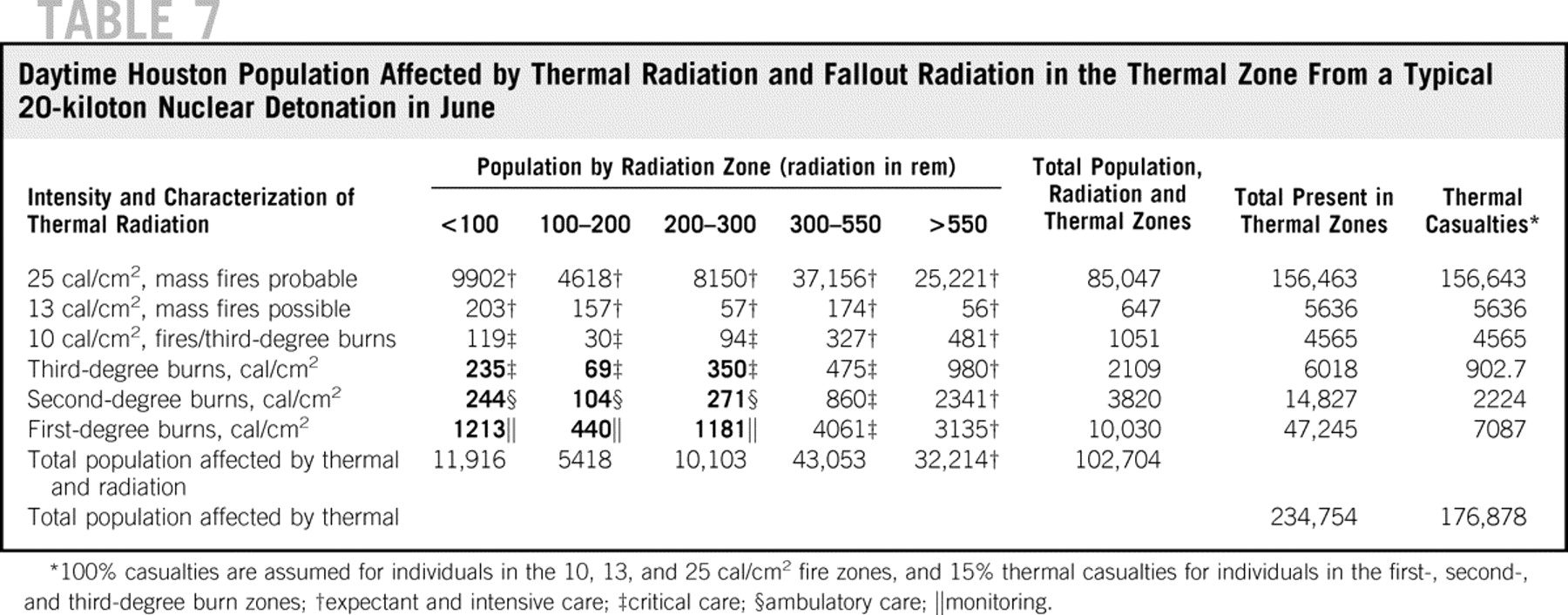
The 20-kiloton attack in downtown Houston resulted in 176,878 thermal casualties. Of these, >10,000 burn casualties would have survived (902 third degree, 2224 second degree, and 7087 first degree.) Combined casualties totaled 102,704; 4107 combined casualties would be in the <300 rem category with more likely survival (the 9 population figures indicated by bold type in Table 7).
TABLE 7 Daytime Houston Population Affected by Thermal Radiation and Fallout Radiation in the Thermal Zone From a Typical 20-kiloton Nuclear Detonation in June
DISCUSSION
The size of the populations affected by a 550-kiloton nuclear weapon detonated in Los Angeles and Houston is staggering: the thermal casualties that survived are estimated at 185,000 and 59,000, respectively. Even the 20-kiloton detonation in Los Angeles and Houston are significant; the numbers of survived casualties requiring care exceed 28,000 and 10,000 people, respectively.
The surviving health care community would be faced with an unprecedented burden of care for burn casualties. This burden would be compounded by the loss of physical (eg, hospitals, clinics) and human resources as demonstrated by all 4 modeling results. In addition, the complete breakdown of transport and communications infrastructures would further complicate the issue.
Combined Casualties
The generation of a radiation plume following nuclear detonation would ensure that a “wedge” of the circular distribution of thermal casualties would experience high levels of radiation exposure as well (Figs. 1B, 1C, 2B, 2C). In the 550-kiloton Houston simulation, the number of surviving thermal victims would decrease significantly because of this high degree of combined effects. Combined casualties with the most improved survival rates are the first-, second-, and third-degree burn zones with radiation <300 rem, which would account for 7300 thermal casualties in the 550-kiloton detonation.
The lower proportion of combined casualties in Los Angeles is interesting and is primarily due to weather conditions that narrow the scope of dispersion of the radionuclide contaminants relative to that which occurred in Houston in these simulations. As a result, there were 4 times the amount of combined casualties in Houston (4107 combined casualties) compared with Los Angeles (997 casualties) in the higher survival category of <300 rem for 20-kiloton detonation. Using the schematic for triage care categorization, the 20-kiloton detonation for Los Angeles also showed the high proportion for expectant/critical care with 19,305 and 2698, respectively.
The exact effect of the combination of radiation and thermal injury on mortality in humans is unknown,Reference Becker, Buescher, Cioffi, McManus and Pruitt6 therefore, it is difficult to give a definitive recommendation on the severity of the interaction of these 2 types of injuries on enhanced mortality. In animal studies it has been shown that as little as 25 rad given to animals with 20% burns resulted in significantly increased mortality over thermal injury alone.Reference Alpen and Sheline27 Likewise, 4 Gy of total body irradiation, which is 20% lethal in animals, resulted in 90% mortality in animals with 15% surface area burn, which was nonlethal by itself.Reference Baxter, Drummond and Stevens-Nesham28 The high mortality of burn patients from the 1945 detonations over Hiroshima and Nagasaki was also difficult to explain based solely on thermal injury.Reference Brooks, Evans, Ham and Reid4
Expansion of Mass Casualty Burn Care Personnel
These modeling results demonstrate the need for an expansion of properly trained personnel and for external regionalization outside any city to meet this extreme challenge. Consideration should be given to training ancillary discipline groups such as pharmacists, dentists, and veterinarians to provide care. Survival rates could be increased if ancillary health personnel and citizens in support roles were properly trained in limited but strategic roles such as burn triage, debridement of wounds, and administration of ameliorative short-term care.
Infection is another major problem in the treatment of burn victims, as are other communicable diseases that would proliferate after nuclear attack. Reference Abrams and von Kaenel29–Reference Munster31 The expanded ability to provide proper wound debridement that would be enabled by the expansion of appropriately trained medical personnel, and followed by the appropriate pharmaceutical intervention to prevent subsequent infection would significantly increase mass burn victim survivability. A security support role for these personnel would include protecting patients and marking the burn victim treatment site with a distinctive flag for further treatment as additional resources become available. Emergency community clinics would need appropriately trained staff, protected by local volunteer law enforcement personnel, such as Volunteers in Police Service32and the Medical Reserve Corps.33
The high probability of inner-city target areas means that there would be a remarkably high percentage of casualties who are minorities. Using block group data for Los Angeles, the 20-kiloton thermal effect area is 70% Hispanic and other minorities and 30% white, whereas in Houston, 60% are mainly Hispanic and/or black and 40% are white.34 It is essential that training of additional health care providers be targeted at minority groups who actually reside in these high-risk areas in the inner cities.
Monitoring Internally Displaced Populations
Among the issues related to all mass casualty medical care in the event of a major catastrophe is the thousands, or potentially millions, of people who would be displaced from their homes (ie, internally displaced citizens, or IDCs) for lengthy periods or who may require quarantine. These people would need shelter, food, potable water, nonfood items, and basic health care such as immunizations or medicine. Sufficient security must be provided to protect them from theft, black-market activity, and physical and sexual assault, all of which reach alarming rates during crisis situations.
Detailed instructions for laying out and extending housing/camps have been devised by the United Nations High Commissioner for Refugees, the Norwegian Refugee Council, and others. 35–37 Protocols can be established to allow for high volumes of burn patients to be triaged and treated without having a verified burn unit.Reference Leslie, Cushman, McDonald, Joshi and Maynard38 Systems to track large numbers of IDCs and refugees exist in many countries outside the United States and are administered by such United Nations agencies as the Office for the Coordination of Humanitarian Affairs and the High Commissioner for Refugees. These systems need to be adapted and be made ready for use in the event of an urban nuclear attack.
Adaptations of Pharmaceutical Stockpile Properties
A strategic national stockpile has been developed for radiological events,Reference Waselenko39 and a similar stockpile for mass casualty burns must be developed. Pre-positioning stockpiles of narcotics for use in mass burn care and training community workers would aid in the treatment of the thousands of victims of an urban nuclear attack, who otherwise would not receive these critical medications (especially for burn treatment) until much later. In the anticipated target areas, it could be useful to further develop plans for housing and secure stockpiles of narcotics for use in a nuclear attack. Narcotics are currently stored at hospitals and many clinics, and these efforts could be significantly expanded, although it must be borne in mind that hospitals may be hard to access in a crisis because of their concurrent health care delivery functions. In addition, these sensitive supplies could be stored at police stations, where significant security already exists.
Preparation for a nuclear event will require the development of a procedure for dispensing narcotics in the most efficient manner to serve mass burn casualties in crisis conditions. It will also be necessary to address legislation concerning record-keeping, access to medications, and Health Insurance Portability and Accountability Act regulations. Training programs for community preparedness to enact these changes in pharmaceutical interventions would include first aid courses, cardiopulmonary resuscitation, pain assessment, medication administration, incident command, and radio communications.
Regional Mobilization of Medical Resources and Personnel
In most high consequence events, and especially in a nuclear attack, medical personnel ingress and patient egress from the affected areas in urban environments will be severely constrained along land routes by panic evacuation; hazardous chemical, biological, or radiological conditions; building and road rubble distortions; and security and/or quarantine restrictions. The need to transport medical personnel from outside areas into the affected urban areas would be severely restricted, especially in the first hours and days after an event, when medical care is most needed, especially for burn care. Certain categories of equipment, such as ventilators, will also be in short supply.Reference Kumar and Jagetia40, Reference Rivara, Nathens and Jurkovich41
Many of these difficulties could be overcome with air transport and medical evacuation capabilities, if adequate landing and response areas were established in advance of a crisis. Medical air evacuation, when quickly rendered feasible, can be the best means of getting large numbers of patients with critical medical needs to distant medical facilities. The United States has the most extensive large airplane transport fleet in the world, which demands its incorporation into a credible urban medical transport response to high-consequence events.
The optimal operational locations for air transport exist in the “horseshoe” areas of Figures 1B and 2B. Limited air transport resources could be concentrated where the most treatable patients are and yet protect health care workers. A key element in all of these considerations is protecting responder personnel from radiation.Reference Gonzalez42
Limitations
As with any model, there are many sources of uncertainty with regard to input parameters. This is particularly true in the complexities of a city landscape. In this study, effort was made to use the most accepted input parameters and validated models to produce the results herein.
CONCLUSIONS
It is imperative that cities consider the catastrophic health consequences of a nuclear detonation and create plans that will account for such an extreme challenge. It is hoped that these 4 models have provided appropriate insight into the extreme challenges faced when responding to such a high-consequence event.