The influenza pandemic of 1968 emerged in southern mainland China and spread to Hong Kong before entering international air traffic and shipping routes and propagating globally. The virus responsible for the pandemic, A/Hong Kong/68 (A/H3N2), was isolated in Hong Kong in July and August 1968 during a period of substantial local media reporting on the crisis.
As was seen during the emergence of severe acute respiratory syndrome (SARS) in 2002 and 2003 in China, local media reporting describing a local public health crisis preceded international recognition and declaration of a potential global threat. During both the 1968 influenza pandemic and SARS in 2002–2003, Hong Kong was the geographic point of recognition of an emerging global threat introduced from southern China. Unfortunately, in both instances preemptive communication of public health crises in southern China did not occur early enough to enable effective warning before the pathogens entered the international air and oceanic shipping grid. The present article reviews local media reporting in the context of A/H3N2 in Hong Kong before and during international recognition of the imminent threat of a pandemic.
METHODS
Four major Chinese-language newspapers and 1 major English-language newspaper published in Hong Kong in 1968 were identified through the University of Washington Library and Seattle Public Library systems in microfilm format (Table 1). Daily articles from these 5 newspapers between July 1 and August 31, 1968 were manually reviewed in native vernacular Chinese and English for all references to the presence of respiratory disease or influenza in southern China and Hong Kong.
TABLE 1 Local Media Sources Used in the Analysis of the Outbreak of A/H3N2

All of the issues of the World Health Organization’s (WHO) Weekly Epidemiological Record from July 1 to August 31, 1968 were reviewed for reference to novel changes in global influenza surveillance data to document public declarations of international community awareness of a possible shifted strain of influenza in southern China and Hong Kong.
RESULTS
On July 11 (day −5), Ming Bao reported the spread of influenza in Guangzhou, China, and nearby cities in Guangdong province, as well as the lack of medication in Guangzhou due to the public’s buying up and hoarding all of the available stock in pharmacies. Primarily due to civil unrest in the context of China’s Cultural Revolution, unburied bodies were “piled everywhere” in Guangzhou and nearby cities, and the hygiene situation was worsening. There were reports of rioting and robbing of restaurants and grocery stores of food, which prompted the closure of local businesses out of fear.1
Based on this information, the Hong Kong Medical and Health Department released a statement that they were reinforcing inspections of food, animals, and people coming from mainland China at customs, ports, and bus stations. As of July 11, officials in Hong Kong indicated no evidence of transmissible disease at the ports of entry to Hong Kong from the mainland.1
Subsequent media reports in Hong Kong on July 22 and 27 (days 6 and 12, respectively, of Hong Kong’s involvement) supported the assertion that Guangzhou and surrounding areas were experiencing an influenza epidemic as far back as May 1968 that infected nearly 60% of Guangzhou citizens and caused extreme shortages of medications.2, 3
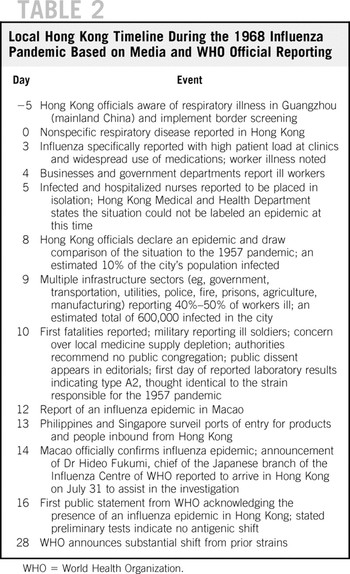
Hong Kong officials first noticed a dramatic increase in reports of influenza-like illness to the Hong Kong Medical and Health Department Epidemiological Office during the week of July 7–13, and samples were acquired for testing that later were found to be positive for influenza. Table 2 displays key time points in the local Hong Kong event evolution process.4–56 The abrupt, rapid progression of multisector infrastructure compromise seen in the table was due to worker absenteeism. As shown in Figure 1, local Chinese- and English-language media provided robust coverage of the 1968 influenza pandemic. Influenza was not a notifiable disease in Hong Kong at the time; however, daily reporting of the situation was comparable to increased reporting of influenza-like illness (by week).Reference Wiebenga, Chang, French and Woolridge57
TABLE 2 Local Hong Kong Timeline During the 1968 Influenza Pandemic Based on Media and WHO Official Reporting
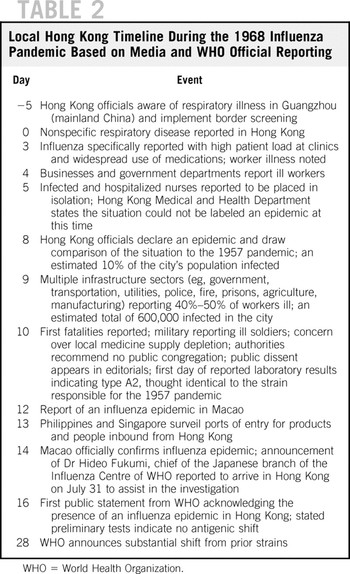

FIGURE 1 Chinese-language and English-language media article counts (excluding advertisements) over time providing coverage of the 1968 influenza pandemic in Hong Kong. We hypothesize day 0 for media-derived information was July 16, with mention of influenza-like illness in the community and influenza-like illness reported to Hong Kong officials lagging by at least 3 days.
Hong Kong media reported introduction of the virus to Japan in week 4,46 to Singapore in week 5,47 and to the Philippines in week 6. 53–55
DISCUSSION
Based on local media reporting, A/H3N2 appeared abruptly in Hong Kong and within 1 week began to affect the functioning of the health care sector as well as civil infrastructure due to worker infection and absenteeism. Other contemporary reports of the 1968 influenza pandemic have also suggested that abrupt reporting of multisector absenteeism was a prominent early feature.Reference Matlof, Murray, Kamei and Heidbreder58–Reference Lee, Wong and Tambyah61 Local recognition of a grossly unusual disease event was revealed as officials addressed comparisons to the 1957 pandemic on day 8. These observations preceded laboratory diagnosis confirming the presence of a shifted influenza virus on day 28.
There were delays in local recognition of unusual respiratory disease present in the community from days 0–5. We propose that this was due to the difficulty in distinguishing nonspecific clinical findings of typical seasonal influenza from those of a shifted strain. Although Hong Kong officials expressed an awareness of unusual respiratory disease in Guangzhou and subsequent reports of influenza-like illness present in the community, it is unclear what decision points were driven by this information. Despite the initial delay in recognition, it was still another 20 days before definitive laboratory confirmation could be achieved. This is an important comment about the emphasis placed on laboratory diagnostics that alert the public health community to a rapidly emerging infectious disease threat, especially one that was associated with a high transmission efficiency as a shifted influenza strain. Figure 1 presents an interesting argument for the integration of syndromic surveillance and local media monitoring, in which tracking of influenza-like illness and local social indicators may reveal a more complete picture of a nonroutine biological event affecting the functioning of a community. Entities providing early warning of pandemics must embrace an integrated approach that includes local media reporting of unusual respiratory disease with an understanding of cultural norms. We emphasize the possibility that abrupt, multisector, and broad age range absenteeism may represent a critical early indicator for pandemic surveillance.
Hong Kong officials were able to present limited options, through periodic situational awareness provided to the media, for countermeasures to their community such as general contact avoidance recommendations and the extension of hours of operation at government-run clinics. It was, however, quickly acknowledged little else could be done to mitigate the situation. Fatalities were reported late (day 10), followed by the first wave of public dissent in the form of editorials in the media. These editorials later criticized officials for not taking more aggressive countermeasures to protect the public. Multisector infrastructure effects that peaked in week 2 revealed the disruption of social processes that are vital to maintaining community integration, and the resolution of diagnostic uncertainty regarding the cause of the virus itself was delayed until nearly 1 month into the situation. It is remarkable that more social anxiety and dissent was not recorded given the residual social sensitivity to the 1957 pandemic. We hypothesize that social concern in the form of dissent was triggered primarily by reports of fatalities versus perceived failure on the part of local officials to present viable countermeasure options. We propose that the relatively short time period of infrastructure impingement and low number of fatalities reported mitigated increasingly worse public reaction to the situation.
Direct ground observation of event features during crises and disasters represents the ideal in data collection. Given the historical nature of this study, however, the media remained a primary source of this information. This represented a limitation in this study, and we were unable to control for possible exaggeration in reporting or missed event features. Finally, precision in regards to what day constitutes “day 0” of this event is debatable given that influenza was not a notifiable disease at the time in Hong Kong and surveillance and laboratory test data were incomplete.
A similar social awareness pattern was documented during the 1957 influenza pandemic, in which local community awareness of atypical respiratory disease in southern China preceded the appearance of the causative virus, A/H2N2, in Hong Kong. It was not until after spread of the virus to Singapore that the WHO was aware of this possible imminent threat to the world. Unfortunately, the virus had already entered the global transportation grid. With some degree of chagrin, the WHO in 1958 stated:
The first reports to reach WHO were from Singapore early in May to the effect that an extensive outbreak of influenza was occurring and that it appeared to have been introduced from Hong Kong. Later, information was received that the epidemic began in continental China about the third week in February and according to Chu (1958) it originated in Kweichow Province between Kweiyang and Kutsing, which is in Yunan Province. In early March the outbreak had spread to Yunan Province and by the middle of March it had spread all over China. The virus was first isolated in Chanchung by Chu et al. (1957) and in Peking by Tang and Liang (1957) and it is clear that they recognized most of the important features of the virus which have since been described elsewhere. It is unfortunate that this information did not reach the rest of the world until the epidemic was already spreading widely. If it had we should have had two more months in which to prepare [emphasis added].Reference Payne62
As noted in this study, the influenza pandemic of 1968 was associated with a similar social awareness and initial pattern of spread as the 1957 pandemic. The observation by the WHO in 1969 was likewise similar:
We are dependent on a single newspaper report that the outbreak in Hong Kong was immediately preceded by an epidemic of acute respiratory disease in southeastern China. There is no information on the etiology of this outbreak in China but its close temporal relationship to subsequent events makes it possible that it was due to the Hong Kong strain. It will have escaped none of the members of the Conference that the 1957 pandemic first came to light in southern China, and the experience in 1968, though very tenuous, adds a little more information to the often-expressed hypothesis that strains of influenza virus which have the capacity to spread widely and rapidly often arise in that part of the world. Unfortunately contact between health authorities in China and other countries is even more difficult than in 1957 and it is impossible to obtain information on the possible origin or behavior of the epidemic prior to its appearance in Hong Kong [emphasis added].Reference Cockburn, Delon and Ferreira63
During the emergence of SARS in 2002 and 2003, Hong Kong officials became aware of atypical respiratory disease in Guangdong province through media reports; unfortunately, the disease had already entered Hong Kong. It was clear that there was local social awareness of atypical respiratory disease in Guangdong province, China, for months before Hong Kong officials became aware. Unfortunately, delays in communicating with Hong Kong resulted in delays in prompting investigative scrutiny, which ultimately resulted in substantial delay in notifying the world of a global public health threat.Reference Wilson, Polyak, Blake and Collmann64 This point was emphasized by the WHO with the statement, “as many times occurs with emerging and reemerging infectious diseases, national surveillance mechanisms failed to identify and respond to the emerging outbreak of SARS early enough to prevent its toll of sickness, death, and international spread.”65
This highlights an important and persistent 50-year-old pattern when considering rapidly alerting the next influenza pandemic, should it appear in southern China. In all 3 scenarios, social awareness began in southern mainland China, followed by Hong Kong, and then the international community, with official public notification declaring a global public health threat occurring well after the respective viruses entered the global traffic grid.
Hong Kong is no longer a gateway to southern China. The explosive economic growth of China has resulted in a corresponding expansion of air traffic connectivity between the mainland and rest of the world, as shown in Figure 2. From 1989–2006, the number of passengers flying to and from China increased by a factor of more than 33. In 1989, there were 5 Chinese cities with outbound flights to the rest of the world; in 2006, there were 36. The growth of air traffic connectivity between China and the world represents both a volumetric and nodal expansion.

FIGURE 2 Bidirectional air traffic connectivity between China and the world, by annual total passengers. The notch in the curve corresponding to 2003 was the result of travel restrictions during the SARS outbreak. SARS = severe acute respiratory syndrome.
When considering the growth of air traffic connectivity between Guangzhou and the world, a similar pattern is noted, as shown in Figure 3. From 1989–2006, bidirectional air traffic between Guangzhou and the world increased by a factor of nearly 980. Guangzhou was connected to 2 international cities in 1989; by 2006, this number had increased to 28 cities.66

FIGURE 3 Outbound air traffic between Guangzhou and the world, by annual total passengers. The notch in the curve corresponding to 2003 was the result of travel restrictions during the SARS outbreak. SARS = severe acute respiratory syndrome.
Proactive social awareness can make a difference in mitigating the effects of an inbound emerging infectious agent. During the emergence of SARS in 2003, the British Columbia Centre for Disease Control was able to issue multiple advisories ahead of WHO official global alerting on SARS. This enabled proactive surveillance for severe respiratory disease in travelers returning from China and Hong Kong. This procedure resulted in the rapid identification and isolation of what was the index case of SARS in Vancouver, Canada.
In contrast, the city of Toronto, Canada, did not make proactive use of situational awareness. By the time WHO issued a global alert, there were 14 infected individuals in Toronto. The virus was introduced by a traveler returning from Hong Kong unrecognized as the threat she represented. Rapid recognition of foreign biological threats and proactive communication of that information are key to mitigating the potential damage sustained by communities that may be connected to that threat by air traffic, cultural diaspora, or commerce.Reference Skowronski, Petric and Daly67
Several nonprofit and academic entities, such as the Global Public Health Intelligence Network,68 ProMED,Reference Madoff and Woodall69 HealthMap,Reference Freifeld, Mandl, Reis and Brownstein70 and Argus,Reference Wilson, Polyak, Blake and Collmann64 have attempted to address media-based global monitoring of disease events via an emphasis on computer automation with varying degrees of human oversight. However, a robust analytic discipline is required to provide the appropriate cultural context and experience when interpreting the complex interaction between disease hazards and socioeconomic vulnerability.71
Conclusions
Media reporting in all 3 of the above-mentioned international public health threats involving respiratory viruses preceded public health threat assessments using epidemiological and laboratory data, thus emphasizing the need to contemplate global warning even if a clear clinical profile and a laboratory diagnosis are uncertain. When considered in the context of a China that is increasingly connected to the world through direct, nonstop air traffic, creative reconsideration of the global approach to early warning of pandemic influenza is a necessity.
Authors' Disclosures
The authors report no conflicts of interest.
Acknowledgments
This work was supported through internal funding by the Office of the Chief Scientist, Veratect Corporation. The authors wish to acknowledge the assistance of Mr Kevin Berardinelli in acquiring the air traffic data used in this study.