Public health emergencies often have an unprecedented scale and time span.Reference Nelson, Lurie, Wasserman and Zakowski 1 The incident command system (ICS) provides a common structure to control and coordinate the response to complex, large-scale, or unpredictable emergencies in a clear, consistent, and effective manner.Reference Moore, Mawji, Shiell and Noseworthy 2 It has become the standard model for use during the response to public health emergencies in most Western countries.Reference Burkle, Hsu and Loehr 3 The lessons learned from application of an ICS for large-scale infectious disease outbreaks with person-to-person transmission are documentedReference Burkle, Hsu and Loehr 3 ; however, there is scant evidenceReference Kirrage, Hunt and Ibbotson 4 on the application of an ICS to manage a local multiagency response to a disease cluster with environmental health risks.
Infection with Legionella pneumophila is of public health concern, because of the organism’s ability to cause large outbreaks and high mortality in vulnerable groupsReference Guest and O’Brien 5 . Legionnaires’ disease is largely preventable through well-established environmental risk management strategies. L. pneumophila are transmitted through infectious aerosols and outbreaks are commonly associated with contaminated water systems, such as cooling towers.Reference Guest and O’Brien 5 In the state of New South Wales (NSW), Australia, Legionnaires’ disease is a notifiable condition under the Public Health Act, 2010. 6 In NSW, building occupiers are responsible for the installation, maintenance, and cleaning of water-cooling systems on their premises and are required to register those systems with their relevant local council. 7 Local council or government Environmental Health Officers (EHOs) undertake routine inspections of water-cooling systems, whereas Public Health Unit (PHU) EHOs are responsible for managing any environmental health risks associated with these water systems during outbreaks.
The Sydney Local Health District (SLHD) PHU in NSW was notified of 5 cases of Legionnaires’ disease during a 2 week period in May 2016. All cases were of people who had spent some time during their exposure period (ie, 2-10 days before symptom onset) in at least 1 of 3 local councils (ie, local government area, municipality, or county) in SLHD: Burwood, Canada Bay, and Strathfield. If there were 2 or more cases with similar exposure locations within a 3-month period, a local cluster investigation was initiated according to NSW Health guidelines. 6
In the preceding months, NSW Health, the state health department, had been investigating several Legionnaires’ disease clusters in metropolitan Sydney, and these had already attracted a high level of media interest.Reference Aubusson 8 Although the epidemiological aspects and outcomes of this investigation are published elsewhere,Reference Dowsett, Quinn and Gupta 9 this paper focuses on the lessons learned from using an ICS structure to manage the environmental health field response associated with this disease cluster.
INCIDENT RESPONSE
Governance and Communication
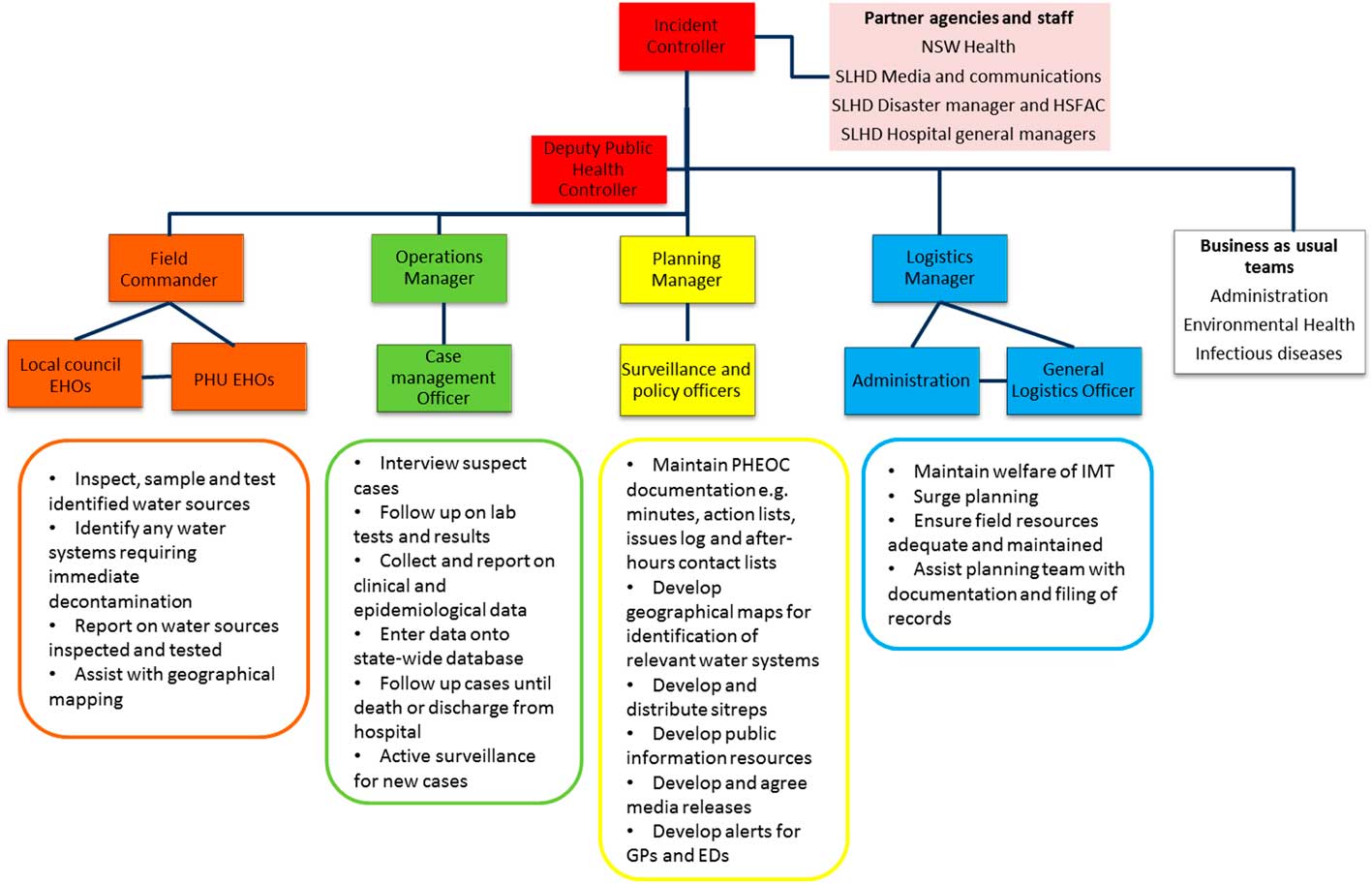
On 17 May, the PHU Director, as Incident Controller (or Manager), established a local incident management team (Figure 1), consisting of representatives from the 3 local councils as well as PHU staff. The field team consisted of PHU staff and local council EHOs and was located off-site in each of the council offices, whereas the Operations, Planning, and Logistics teams were located within the PHU (Figure 1). The PHU Emergency Operations Centre was designated as the central point of communication for the local incident management team and partner agencies. Twice daily (17-24 May) and daily (25-31 May) briefings were conducted in the PHU Emergency Operations Centre via teleconference and involved other response partners. Operational issues were discussed and the resulting action items were delegated to the appropriate team leader in the ICS. Partner agencies involved in the briefing meetings included hospital general managers, the NSW Health and the SLHD Media and Communications Director, the Disaster Manager, and the Health Services Functional Area Coordinator.
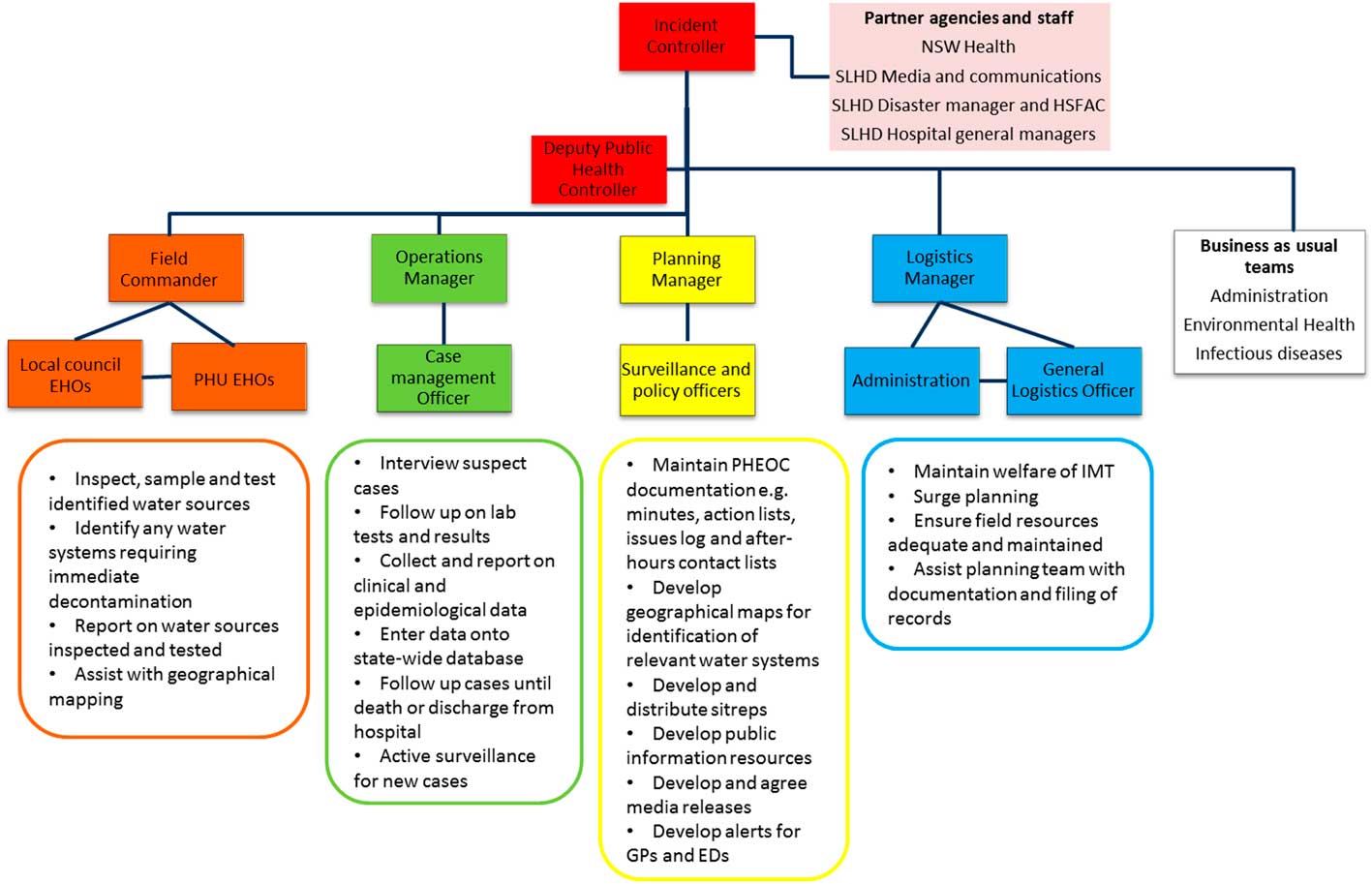
Figure 1 Incident Command System Structure and Functional Roles for the Response to the Legionnaires’ Disease Cluster Investigation in Sydney Local Health District, NSW, Australia, May 2016. EDs, emergency departments; EHOs, environmental health officers; GPs, general practitioners; HSFAC, Health Services Functional Area Coordinator; IMT, incident management team; PHEOC, Public Health Emergency Operations Centre; PHU, Public Health Unit; SLHD, Sydney Local Health District.
Functions and Roles of the Incident Management Team
The structure and responsibilities of functional teams within the incident management team are shown in Figure 1. It is important to note that the field team initially focused their inspections on water systems within the Burwood local council area as the first 3 cases had been there during their exposure period. However, after further review of mapping of exposure histories from the additional 2 notified cases using geographical information systems, the investigation area was expanded on 19 May to include Canada Bay and Strathfield local council areas. Although the field team was subsequently re-deployed to these areas, a local Emergency Operations Centre at Burwood was maintained for all communications with the PHU Emergency Operations Centre. NSW Health provided technical support to the field teams for the transport and analysis of water samples at the state reference laboratory. Partner agencies and staff (Figure 1) reported directly to the Incident Controller to maintain the chain of command during the investigation.
Lessons Learned: The Field Investigation and Use of ICS
Once the investigation was concluded, a structured face-to-face debriefing meeting was held in June 2016 and attended by 26 of the 44 (60%) individuals invited from all 5 response agencies. Participants were organized into small groups to discuss and report back on lessons learned. The key lessons are described below in relation to the application of an ICS for the field response.
Governance, Function, and Roles in the Incident Management Team
The allocated ICS structure and roles were appointed early and considered helpful, particularly for PHU staff, while routine functions were also maintained (Figure 1). The ICS structure was robust for coordination of the field team and for communication with the incident management team, despite the team being re-deployed to 3 different areas during the investigation. The ICS had clear leadership from the Incident Controller; however, sometimes, the chain of command required further clarification with external partner agencies for understanding their role within the ICS and also for establishing contact points for the staff leading the functional teams in the structure. This briefing can be verbal, but all partner agencies should also receive a copy of the ICS structure (Figure 1).
Coordination and Communication with Partner Agencies and the Public
As identified elsewhere, the use of an ICS helped to ensure clear communication channelsReference Rebmann, Carrico and English 10 within the incident management team and with other partner agencies, particularly with regards to the incident management team briefings and any resource requests or issues that needed remedial action. The existence of good working relationships between the PHU, local councils, and NSW Health was critical for the successful field investigation. In particular, there is an annual agreement or operational plan between the PHU and all 8 local councils within SLHD, which outlines how PHU and local council staff will work together to prepare for and respond to any local emergency. Although it is a mandatory requirement that all NSW Health staff are trained in the use of ICS, 11 the practical application during this response was a good exercise for both PHU and local council staff working together in an incident management team.Reference Biddinger, Savoia, Massin-Short, Preston and Stoto 12 As previously noted,Reference Kirrage, Hunt and Ibbotson 4 Legionnaires’ disease outbreaks can generate intense media and public interest, because of the potential for rapid spread of the disease if not contained and because of deaths occurring in at-risk groups. At the time, media interest in Legionnaires’ disease in Sydney was already high because of a previously reported but unrelated cluster of several cases in the central business district of the city.Reference Aubusson 8 Therefore, in order to ensure accuracy, consistency, and timeliness of information reported to the media to maintain public confidence in the local response, all media requests were centrally managed between the Incident Controller and NSW Health.
Control and Prevention of Any Environmental Health Risks
Local councils were able to quickly locate cooling towers, negotiate access to them with their occupiers, and jointly inspect and sample them with staff from the PHU. NSW Health was also able to rapidly arrange for transport and microbiological analysis of large numbers of water samples at the state reference laboratory. The field teams responded quickly to water systems that were not operating under legislative requirements – that is, by ordering immediate decontamination and further monitoring of systems. These 3 aspects were critical for the incident management team being able to control any ongoing environmental health risk in the field during the investigation. It was agreed that, in future, proactive maintenance of the local council register for water-cooling systems would be shared between the PHU and local councils.
Supporting Surveillance and Planning Functions
The use of Geographical Information Systems mapping was key to being able to identify water systems within a 500 m radius of common exposure locations in near real-time for inspection and testing as per NSW Health guidelines. 6 Geographical Information Systems are becoming a popular tool for analyzing spatial data during outbreaks of Legionnaires’ disease.Reference Bull, Hall, Leach and Robesyn 13 Standard processes for using Geographical Information Systems would assist staff with the rapid and consistent identification of water sources most at-risk for transmission of L. pneumophila during future investigations.
DISCUSSION
Some evaluations of the use of ICS for management of large-scale disasters (eg extreme weather events or terrorism)Reference Buck, Trainor and Aguirre 14 , Reference Moynihan 15 and infectious disease emergencies (eg, pandemic influenza)Reference Burkle, Hsu and Loehr 3 , Reference Bone 16 have been published. However, little has been documented regarding the use of ICS for a local multiagency response to a disease cluster with environmental health risks.Reference Kirrage, Hunt and Ibbotson 4
The occurrence of five confirmed cases of Legionnaires’ disease within 2 weeks is unusual for SLHD, and with the evolving uncertainty around the potential extent of the outbreak, the early and judicious use of ICS was warranted.Reference Burkle, Hsu and Loehr 3 , Reference Bone 16 Although previous evaluations have criticized the hierarchical nature of the ICS,Reference Moynihan 15 this system worked well in the current investigation because of the strong working and shared power relationships between response agencies, which had been established over many years, fostering trust and enabling rapid agreement on response strategies. Although training in the use of ICS can improve awareness and knowledge of these systems, it was the practical application of this system during this investigation that response partners felt increased their skill, confidence, and capacity to respond to future emergencies.
Previous evaluations of the use of ICS have noted that its implementation is more effective when the response strategies and tactics are well known and commonly understood.Reference Buck, Trainor and Aguirre 14 Legionella prevention and control strategies are routine work for EHOs. However, the clear acknowledgment and use of environmental health expertize by the Incident Controller and the technical proficiency of staff in inspecting and sampling water systems were key to the field response.Reference Kunz and Cooley 17
Overall, response partners reported that the use of ICS was justified for this low-scale event. No further cases with similar exposures had been notified at the end of the investigation, indicating the effectiveness of the response strategies. However, the cost-effectiveness of such a resource-intensive activityReference Lock, Millet and Heathcock 18 should always be balanced against the risk for a larger outbreak occurring when considering the use of ICS for managing a response. Given the resource, cost, and logistical constraints of implementing an ICS, the decision to use this system should always be based on a risk assessment of the likelihood and potential impacts of the hazard at the time.
CONCLUSIONS
The strategic application of the ICS for this Legionnaires’ disease cluster enabled timely and effective coordination of the multiagency field response. Although all PHU staff had already participated in ICS training, it was the practical use of the system during this investigation that improved staff capacity and resilience to respond to similar incidents. Documenting the lessons learned may also help public health and local council staff refine their collaborative response to Legionnaires’ disease clusters or outbreaks in the future.