On April 15, 2013, two improvised explosive devices (IEDs) exploded at the Boston Marathon in a terrorist attack. Three bystanders were killed and 264 total patients were treated at 26 local hospitals in the aftermath of the event.Reference Malone 1 Despite the life-threatening injuries sustained by multiple victims, there was no subsequent mortality among those who survived transfer to a hospital.Reference Walls and Zinner 2 Many factors contributed to the high survival rate, including the location, timing, and characteristics of the IED, preparation for this annual mass gathering event, and the actions of bystanders and prehospital providers.Reference Walls and Zinner 2 - Reference Goralnick and Gates 5
Among the least understood factors in this and other major disaster responses were the leadership decisions and actions. 6 Most medical after-action reports (AARs) are anecdotal or descriptive.Reference Bradt and Aitken 7 Complex aspects of health care, including crisis leadership, teamwork, quality of care, and safety, are particularly amplified during a mass casualty incident (MCI) and may be best assessed by qualitative rather than quantitative analysis.Reference Giacomini and Cook 8
The objective of this investigation was to characterize organizational dynamics and leadership themes during and immediately after the Boston Marathon bombings utilizing a structured sequential qualitative approach consisting of a focus group followed by subsequent detailed interviews and expert analysis.
Methods
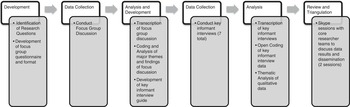
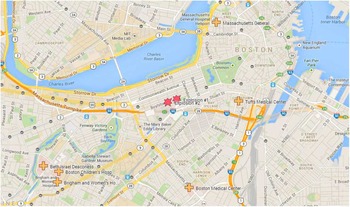
A flow chart of the research design and analysis is presented in Figure 1. Shortly after the bombings, we formed a consortium comprising emergency medicine (EM) and trauma surgery physicians who were designated as the institutional leaders of the 5 Level 1 adult trauma centers, 1 Level 1 pediatric trauma center, and 1 Level 2 trauma center at which patients received care in the wake of the Boston Marathon bombings (Figure 2). The participants each led debriefings within their own institutions prior to participating in this study.

FIGURE 1 Research Design and Analysis: Flow Chart.

FIGURE 2 Locations of Bombings and Hospitals.
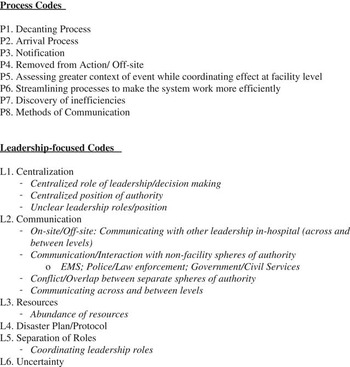
We then invited all 14 of these leaders to participate in a focus group discussion. The focus group discussion was facilitated by faculty members from the National Preparedness Leadership Initiative (NPLI)—a joint crisis leadership program of the Harvard School of Public Health and the Center for Public Leadership at Harvard’s Kennedy School of Government—and Tel Aviv University. The facilitators used Turning Point (Turning Technologies, Youngstown, OH), an audience response system that enables participants to respond anonymously to multiple choice queries, followed by open-ended discussion. Questions were derived from a structured AAR tool developed specifically for MCIs by 48 medical professionals from all 6 Level 1 trauma centers in Israel and a standard set that NPLI uses when evaluating major disasters.Reference Tami, Bruria and Fabiana 14 These questions sought to encourage participation and focus the group on leadership decisions and execution as opposed to strictly clinical decisions or a quantitative review. This focus group discussion was recorded and transcribed. Relevant words and quotations were identified and labeled with codes by a single researcher to create an audit trail (Figure 3).Reference Patton 15

FIGURE 3 Initial Open Coding Structure.
The coded focus group transcript was then distributed and reviewed by a core group of researchers (EG, SL, PH, EM, BD, LM, KP). This team reviewed both the codes and transcripts, focusing on designing a standard interview guide to further elaborate on the themes identified in the focus group.
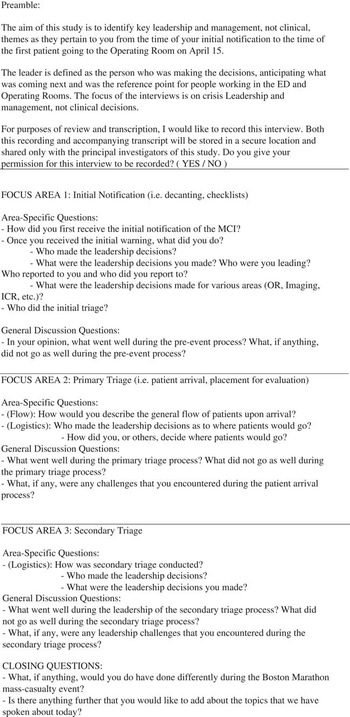
All focus group participants were invited to participate in subsequent key informant (KI) interviews based on a semistructured interview guide (Figure 4); 7 of 14 agreed to participate. Each of these interviews was conducted by a researcher in a private setting at the participant’s respective hospital. Interviews were recorded and transcribed. Following transcription, an analytical process of inductive and open coding was combined with thematic analysis of the data to allow general themes to emerge directly from the data.

FIGURE 4 Interview Guide.
The interview transcriptions and coded materials were shared with 7 faculty members from NPLI, the Harvard School of Public Health (HSPH), and Tel Aviv University (TAU). Additional qualitative data was collected from these faculty members during 2 interviews conducted by interactive video-messaging. During these sessions, NPLI, HSPH, and TAU faculty discussed and fine-tuned the open coding and thematic analysis results and compared and contrasted the Israeli MCI experience with the Boston Marathon bombings response.Reference Waage, Poole and Thorgersen 12 , Reference Adini and Peleg 16 - Reference Lynn, Gurr and Memon 20 During these sessions the team reviewed findings and added multiple perspectives, providing investigator triangulation, a strategy to enhance the rigor of qualitative analysis. Triangulation refers to examining the same data with multiple observers, methods, theories, or data with an aim to reduce systematic bias when drawing conclusions.Reference Patton 21 , Reference Curry, Nembhard and Bradley 22 The manuscript draft was shared with all participants (focus group members and core researchers) for review, clarification, and finalization.
The study was approved by the Institutional Review Board (IRB) of Beth Israel Deaconess Medical Center and funded by Brigham and Women’s Hospital’s Department of Emergency Medicine.
Results
In total, 14 people were invited from the 7 institutions that participated in the response to the bombing. Twelve accepted, representing all 7 institutions. The participants were senior- to mid-level leaders within their organizations, including 6 trauma surgery directors, and emergency medicine physicians including a chairman, vice chairman, and others designated as hospital emergency preparedness leaders.
Several leadership and management themes emerged from our analysis, including initial communications and volunteer surges, leadership and flexibility, information systems, and central command versus collaboration. Select participant quotations from the focus group and KI interviews are included in the supplementary table.
Initial Communications
Comments across respondents consistently revealed that the high volume of communication and confusion following the incident presented a serious management challenge. One participant noted “We used our group page and…we asked them to call back the emergency room, but then…80 people were trying to call back the emergency room at one time so we’re looking for a better way to communicate information out and have them communicate their availability through e-mail or social media.” The initial notification methods varied by institution (pagers, cell phones, e-mail, social media, etc). Another participant stated “people learned about the process going on from the media, from Twitter, from whatever social media they were using.” Many participants noted challenges with initial notification due to city-wide cell phone disruptions. Another said, “We’ve since discovered that our pager system sends out pages in a serial fashion, one after another, so it’s actually quite delayed.”
Volunteer Surge
Every participant noted a surge of volunteers who reported to their EDs. One participant stated “So many people came down [to the ED] that we…just had an overwhelming number of people. It was really crowd control.” Despite efforts to control this surge and potential ensuing chaos, most volunteers found opportunities to positively assist in the overall response. Another participant said “we had some drift of our command and general staff to the ED and the same issue with crowd control. We made crowd control announcements and directed individuals to form a labor pool.”
Information Systems Were the Universal Bottleneck
During the focus groups session, one of the audience response questions posed was “On April 15, what was the primary bottleneck in your system?” Participants chose from the following options: ED Patient Care Areas; Operating Room Availability; ICU Availability; Inpatient Bed Availability; Staffing; Radiology Tests; Laboratory Tests; Information Systems; None. One hundred percent of the participants responded that information systems was their greatest bottleneck. In response to: “Who was primarily responsible for resolving this bottleneck?” One hundred percent answered an administrative leader was responsible, rather than a physician or nursing leader.
One participant noted “If the patient is not in the computer, you cannot order, you cannot do many things. It is very hard to take care of patients that don’t exist.” Another participant stated “One of the things we learned is we don’t have a really easy, flexible, nonelectronic-based way of keeping track of people and we need to do that.”
Further discussion identified challenges with patient identification with unidentified naming conventions that were so similar that 1 hospital noted some “near misses” in differentiating patients’ lab results and studies, in patient tracking and in computerized order entry.
Communications Across and Between Levels
Because city-wide cellphone service was disrupted, communications were challenging not only within the hospitals but also across hospitals and other agencies, including law enforcement, emergency medical services, and public service leaders. One participant noted, “We paired up our law enforcement colleagues with our hospital police and security. Most of them are actually police officers themselves, and it was helpful to have them paired up with people that we knew.”Reference Xiao, Kim and Gardner 33 Solutions included face-to-face communications, runners, and radios.
Participants noted several advantages and challenges communicating through social media during this event. Social media was particularly helpful in providing actionable information.Reference Cassa, Chunara and Mandl 23 For example, 1 anesthesiologist and 1 emergency manager both reported activating their institutional disaster plans based on information from bystanders on Twitter. In the days that followed, during the pursuit and capture of the suspects, participants noted that “tweets” from law enforcement, including the Boston Police Department, became a critical resource for reliable information.Reference Davis, Alves and Sklansky 24 Social media also presented challenges, such as requiring providers to differentiate among “fact, fiction, and hysteria.”
Leadership and Flexibility: Central Command Versus Collaboration
All hospitals initiated their disaster plans; these were predicated on the incident command system (ICS), a tool developed in the 1970s by fire agencies and eventually adopted by hospitals in the 1990s to clarify an organizational chain of command, roles, and authority for personnel involved and identify lines of communication. Participants described “not following the disaster plans exactly as written” and encouraging autonomy in decision-making at various leadership levels. One trauma surgeon remarked, “I think what went well is the independent thinking of the people that we work with on a daily basis. So they were able to think outside the box in each of their fields of expertise. And collectively, we could come together with a good solution. So I like the fact that everybody had a framework to work in, as they do daily, but were allowed some freedom of decision making to make things work well.” This flexibility allowed hospital leaders to maintain organizational functioning across a broad range of hazardous and dynamic challenges.Reference Roberts, Stout and Halpern 25
As each institution activated its emergency operations plans, overlapping spheres of authority became a recurrent theme despite utilizing ICS. This overlap was quickly recognized such that the paradigm of “command-and-control” transitioned to “command-and-collaboration.” One EM physician noted “There was such an immediate response by the entire institution that it was just making sure people didn’t get in their own way—each other’s way. But there was no need to get people to do stuff. If anything, the challenge was to get people to not do stuff. There was such a committed effort and response, people came from all over…leadership had to control the need, desire and participation.” Participants described leaders’ flexible adaptation to the unique dynamics of this event after the initial checklist-driven initiation of a disaster plan as critical to their hospitals’ successful response.
Discussion
Through systematic qualitative interviews and focus group interviews of leadership of 7 hospitals responding to the Boston Marathon bombings, triangulated by international experts in crisis leadership and disaster response, we found that a highly flexible and cooperative leadership structure across institutions contributed to a successful response.
Although several institutions’ emergency operations plans included a predesignated meeting point for labor pool formation, volunteer surges to EDs were universal. Surges of volunteers are typical and understandable in these events (most people want to help) and management styles vary for labor pool formation and role clarification.Reference Roccaforte 26 - Reference Feliciano, Anderson and Rozycki 31 Leaders at 2 institutions improvised: one managed the surge with security personnel providing redirection to an alternate location; another, whose security personnel were already occupied with other tasks, employed 2 technicians, former military policemen, to redirect volunteers. Others have recommended that security personnel limit ED access to medically essential personnel and redirect additional volunteers to a predesignated staging area.Reference Hogan, Waeckerle and Dire 28 , Reference Halpern, Tsai and Arnold 32 Predefining staffing levels (eg, “two ENT physicians will be available in the ED to assess and record every patient’s tympanic membrane status”) is useful for the person assigned to direct staffing. This designee, ideally, is a senior leader, able to effectively yet politely redirect (sometimes very senior) volunteers.
Communication is frequently a challenge during disasters; despite vast preparation for the marathon, the April 15 response was no exception.Reference Hick, Chipman and Loppnow 27 Cell phones services were nonfunctional shortly after the explosions, just as they were after the September 11, 2001 World Trade Center attacks. In Israel, staff members are trained not to call the hospital while responding to an event so as to avoid overloading the telephone services and the attention span of staff already engaged in event management in the ED.
Social media platforms were also a valuable information resource during the response, but misinformation posed a potentially confounding problem for responders.Reference Cassa, Chunara and Mandl 23 Israel has begun to experiment with social media to relay protective measures for civilians during missile attacks and encourage vaccination during the current reemergence of poliomyelitis.Reference Adini and Peleg 16
Information systems were the universal bottleneck for 7 institutions with 7 different IS systems during the same events, which presents both a challenge and an opportunity. IS have been noted to be a key bottleneck during other crises and fixes have included transitioning to a paper-based system or employing an IS disaster mode to streamline order entry.Reference Halpern, Goldberg and Keng 34 , Reference Bookman and Zane 35 Until IS can fully support disaster workflows, preplanning and training of leaders and staff in using structured, paper-based tools and structured procedures for the necessary transition of data into IS will likely minimize variability in response management. For patient tracking, drills have demonstrated the efficacy of radio frequency identification (RFID), but there is no documented utilization of RFID during an actual event.Reference Fry and Lenert 36 - Reference Lenert, Kirsh and Griswold 39 The utility of electronic tagging is likely to be most helpful in the prehospital phase, where, by definition, the degree of chaos and the difficulty in controlling casualty flow is greater. Further investigation is needed to establish national standards for naming conventions for unidentified patients, patient tracking from the site of the incident to hospitals, and streamlining documentation.Reference Landman, Teich and Pruitt 40
Even in a hierarchical system of ICS, self-organization occurred. Order, as opposed to central control, emerged from multiple examples of spontaneous adaptation, such as internal medicine resident physicians who helped clear EDs by rapidly taking signouts and pushing patients to inpatient wards. Some of these actions were explicitly included in disaster plans and some were not. There were instances with direct leadership intervention and others where tasks were simply undertaken by personnel, often with great effectiveness. Staff knew their roles and the roles of others. Rigid hierarchies with dynamic flexibility and “teaming” have also been discussed in the context of trauma resuscitation teams and emergency medicine teams. Reference Klein, Ziegert and Knight 41 , Reference Edmonson 42 The ICS is designed to ensure efficiency and reliability in extreme conditions.Reference Bigley and Roberts 43 Leaders utilizing the ICS are able to structure and restructure frequently, allowing practitioners to balance preplanned organizational solutions to needed improvisation for unforeseen and novel complications that arise in complex, emergent situations.Reference Roberts, Stout and Halpern 44
Further study needs to be focused not only on optimal organization during these responses, but how we may further define and impart these requisite skills to front-line health care providers who will lead crisis response.
Limitations
There were several limitations to this study. First, we purposely restricted the scope of this study to trauma and emergency medicine physicians to allow for facilitation of the focus group and number of KI interviews. Each of the physicians had a varied experience either working primarily as a clinician or designated primary role in the ICS structure at their hospital. Trauma surgery (or surgery) and EM chairs were asked to provide their designated EM and trauma leaders for this discussion. This group, however, limits the experience to 5 Level 1 adult trauma centers, 2 Level 1 pediatric trauma centers and 1 community hospital. This was a community event and our community responded: from bystanders, EMS, Police, firefighters, physicians, and nurses, to environmental services technicians, public health officials, emergency managers, and local, city, state, and national governmental officials. There were many debriefs and lessons learned, but our focus for this study was physician leadership during the first few hours. We hope to further study each discipline’s leadership challenges during the marathon and other future events.
Second, due to their primary duties and responsibilities at their respective institutions, 12 of the original 14 representatives were able to participate in the focus group. Subsequently, only 7 of the original 12 focus group participants were available and completed the key informant interviews, which may have weighted the secondary analysis towards their comments and codes. We balanced this by designing the KI guides based on the results and coding of the initial focus group, but subsequent review sessions were based primarily on interview results. We then circulated drafts of the manuscript to all original representatives for review.
Third, the views of the review group used during the triangulation procedure may have been biased by prior MCIs rather than the Boston bombings, though these perspectives may also add to the richness of the data and support the validity of the findings.
Finally, because of the unique characteristics of the Boston Marathon bombings combined with the high density of emergency response and subspecialists in Boston, the findings may not generalize to other incidents in different settings.
Conclusions
Disasters provide a distinctive context in which to study the robustness and resilience of response systems. Strengths and obstacles that drills or exercises do not reveal become apparent. Yet those strengths and weaknesses are not always systematically captured and shared. Therefore, in the aftermath of a large-scale crisis, every effort should be invested in collecting critical lessons so they can be shared and incorporated into best practices and preparations. Novel communication strategies, flexible leadership structures, and improved information systems will be necessary to reduce morbidity and mortality during future events.
Acknowledgments
Brigham and Women’s Department of Emergency Medicine funded qualitative analysis (focus group and interview transcription, coding) and refreshments for focus group.
Ethics committee approval: Approved by the Beth Israel Deaconess Medical Center Institutional Review Board.
Supplementary Material
To view supplementary material for this article, please visit http://dx.doi.org/10.1017/dmp.2015.42