The term quarantine is derived from the Italian quaranta, which refers to the 40-day sequestration imposed on arriving merchant ships during plague outbreaks of the 14th century.Reference Shedev 1 The term is often used interchangeably with isolation, containment, and civil commitment (sometimes called internment). However, the strict public health definitions of these terms differ dramatically.Reference Barbisch and Gostin 2 Although all are public health procedures relating to physical separation and protecting public health, the significant difference is whether the potentially exposed individual is symptomatic or asymptomatic. Isolation is the “separation of symptomatic infected individuals from those who are not infected.” 3 In other words, “isolation” is for patients who are ill. Quarantine refers to the “separation of individuals who have been exposed to an infection but are not yet ill from others who have not been exposed to and are susceptible to an infection.” 3 Thus, quarantine is for those with no signs or symptoms who have possibly been exposed to a contagious disease and have the potential to transmit the disease to others. If an individual is potentially exposed but asymptomatic, this person may be subject to a quarantine order. Once the individual becomes symptomatic, quarantine would no longer apply and the person should be isolated. The 2001 Model State Emergency Health Powers Act identifies the associated terminology social distancing, which refers to creating a set space between individuals that will reduce the likelihood of transmission of contagion, e.g., 3 to 6 feet for droplets.
The authority to quarantine as a public health measure is a police power established under public health law, ostensibly to prevent the spread of communicable diseases. Independent jurisdictions have the legal authority to enact such laws for their respective areas; thus, one state or country may activate a quarantine order while another may not. The US Federal government quarantine authority is defined in Title 42 US Code §264. However, the US federal government rarely uses its quarantine authority. Ebola and other hemorrhagic fevers were added to the federal list of quarantinable diseases in 1983 by Executive Order 12452, which was signed into law by then President Ronald Reagan. 4 The restrictions associated when quarantine is enacted limit the personal freedom to travel and the proximity to others. These limitations infringe civil liberties. While the goal is protection of the public health by controlling the spread of communicable disease, quarantine is not and ought not to be used as a punitive measure. 5 - Reference Barbara 7 The underlying question remains: Does quarantine prevent the spread of communicable diseases?
The International Health Regulations (2005) (IHR) are the basis of international law and provide the binding legal framework for the management of emerging and reemerging international diseases and other health risks. 8 The IHR recognize that globalization makes national actions such as quarantine increasingly less effective.Reference Gostin 9 As recently as October 23, 2014, the World Health Organization reiterated its recommendation that there should be no general ban on international travel or trade. 10 They noted that general travel bans are considered relatively ineffective. Additionally, travel bans may add to the spread of disease because they run the risk of causing economic hardship that, in turn, may have an unintentional consequence of increasing the migration of potentially infected people from affected locales.
In late October 2014, two authoritative bodies within the United States, the Society for Healthcare Epidemiology in America (SHEA) and the Infectious Diseases Society of America (IDSA), issued similar statements against involuntary quarantine of asymptomatic health care workers (HCWs) with potential Ebola exposure. 11 , 12 Specifically, IDSA stated that it “does not support mandatory involuntary quarantine of asymptomatic healthcare workers returning from Ebola-affected areas” and, further, that “This approach carries unintended negative consequences without significant additional benefits.” 11
Nevertheless, specific guidance on quarantine is often ambiguous and varies from locality to locality. Public health and safety policies vary by jurisdiction, allowing countries and states to determine their respective protocols. The US Centers for Disease Control and Prevention Interim Guidance updated October 29, 2014, states that high-risk, symptomatic individuals should be isolated. 13 The interim guidance also notes that travel to a country with widespread Ebola transmission in and of itself does not require action if the individual had no personal contact with an infected person and is asymptomatic. On the same date, the state of California health officer issued a statewide quarantine order. 14 While this document appears to order a mandatory 21-day quarantine of returning asymptomatic HCWs who have cared for Ebola patients in West Africa, it also states that it applies to “individuals at risk of contracting and spreading Ebola” and further states that “specific requirements of an individual quarantine order shall be determined and communicated by the local health officer.” This has led to confusion and inconsistencies in application of actions to control the spread of disease. Asymptomatic persons do not spread Ebola; therefore, such actions are not scientifically supported.
The state of California order additionally states that “quarantine may include observation and monitoring of the Ebola contact and/or limitations on his or her freedom of movement.” It is unclear whether “observation and monitoring” without restriction of movement constitutes “quarantine” or rather some different type of public health order. Misapplication of quarantine guidelines to asymptomatic individuals resulted in fewer volunteers deploying to support the Ebola outbreak owing to concerns about restrictions upon their return.Reference Duffy 15
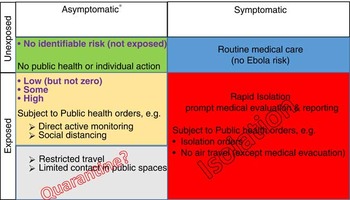
Within a health care facility, isolation is appropriate for symptomatic patients and HCWs with a communicable disease. If healthy individuals are exposed, they may be subject to quarantine for diseases that can be transmitted before symptom development. Even for diseases like Ebola that are not transmitted prior to symptom onset, some level of observation and monitoring is appropriate because of the potential for spread and the disease’s deadly nature. It may be voluntary or, in the case of a public health threat, it may be imposed by legal authorities and compulsory. As in all public health and medicine, a risk-benefit analysis is necessary. While we theoretically could achieve zero risk of transmission of infectious disease by completely separating everyone at all times, this is virtually unattainable and impractical. The challenge is to manage and balance the gray area of unknown exposure, the level of risk associated with the unknown exposure, and the science-based, appropriate level of quarantine to contain the spread of disease and protect the overall public health. Figure 1 reflects the US Centers for Disease Control and Prevention Interim Guidance updated October 29, 2014. 13 The figure further depicts how quarantine and isolation, as defined above, apply within this construct.

Figure 1 Ebola Patient Categories and Public Health Actions. *Type of exposure determines risk of the individual developing Ebola© 2014 Barbisch & Koenig. Reprinted with permission.
Taiwan 2002–2003: A Case Study on Hospital Quarantine
The severe acute respiratory syndrome (SARS) outbreak that affected many countries between November 2002 and July 2003 serves as a case study in quarantine. From an analysis of procedures used during SARS, several major findings emerge as guiding principles in the discussion of quarantine during the 2014 Ebola outbreak. The SARS outbreak resulted in more than 8000 cases and 774 deaths. 16 Both diseases are considered to be transmissible only after a person is symptomatic. However, the transmission of SARS—via droplet spread—differs significantly from that of Ebola, which spreads via blood and bodily fluids. Although those differences can significantly change transmission rates and decisions for appropriate personal protective equipment (PPE), similarities exist in the logic behind determining appropriate, evidence-based uses of quarantine. These include considerations of legal authorities and jurisdictional issues, justification and measured impact of detaining individuals for the protection of public health, the policy of cohorting quarantined individuals, the unintended consequences that may increase disease spread, and the potential negative outcomes associated with unjustified or indiscriminant restrictions of civil liberties.
Taiwan was seen as vulnerable to the spread of SARS owing to heavy travel from affected regions. The first case in Taiwan was identified on March 14, 2003, in a traveler from Guangdong Province, China. Within 5 weeks, 28 probable cases were reported: 24 were business travelers who were cared for primarily at large academic hospitals; 4 resulted from secondary transmission (1 HCW and 3 family contacts).Reference Twu 17
On April 22, 2003, authorities detected an outbreak of SARS among HCWs at a large municipal hospital in Taipei. Officials imposed an unprecedented mass-scale hospital-wide quarantine on all hospital staff, patients, and family members 2 days after the outbreak. HCW clusters at 8 additional hospitals in Taiwan were linked to the initial hospital outbreak. Sporadic community cases reported in Taipei and southern Taiwan were also linked to the initial outbreak. The use of hospital quarantine created an array of significant political, practical, and ethical issues. One unintended consequence of the action was that 4 of the hospitals were forced to discontinue both emergency and routine services for some period of time.
Taipei Municipal Hoping Hospital is a general governmental district hospital with a 500-patient capacity located in the western part of Taipei city. A middle-aged woman who traveled on the same train with a SARS patient from Hong Kong and subsequently visited the emergency department (ED) on April 9 was suspected to be the source of the outbreak. Another index case was a 42-year-old hospital laundry worker with diabetes mellitus and peripheral vascular disease. He had sleeping quarters in the hospital basement and spent off-duty time socializing in the ED. He was reportedly exposed to the woman in the ED and developed fever and diarrhea within 3 days. He was admitted to the hospital on April 16. Three hospital inpatients were first reported as probable SARS cases on April 21. On the next day, 7 staff members at this hospital, including a physician, 2 nurses, a nursing student, a laundry worker, an administrator, and a radiology technician, reported symptoms of SARS. On the basis of epidemiologic links among the cases, 61 HCWs were identified. Those symptomatic individuals were isolated.
Within 24 hours, authorities identified 10 additional cases; none were from the isolated cohort. The cases were identified in the ED and on 6 different floors of the hospital. These findings suggested widespread transmission. Specimens from the suspected SARS patients were sent to laboratories for genetic sequencing analysis to determine the sources of the virus. ED services were closed; the outpatient clinic was reduced. Overnight, an additional 16 cases were reported in connection to the hospital outbreak. The government implemented sweeping quarantine measures, closing down the hospital. By that time, there were 26 cases with symptoms related to SARS. Seven were reported as probable cases, 3 were suspected cases, and the remaining 16 were undetermined.
At noon on April 24, the cross-departmental SARS Emergency Response Task Force ordered the hospital to immediately stop operations. With the objective of preventing further disease spread, the hospital was contained, and all of its staff members, admitted patients, and their visitors and family members were quarantined and restricted from leaving the building. All 930 staff members were ordered to report to the hospital for a 2-week quarantine and were asked to perform duties as usual. All 240 patients staying at the hospital were prohibited from leaving. There were 129 visitors and outpatients at the hospital when an across-the-board freeze on its operations was imposed; they too had to remain in the hospital for at least 14 days. Home quarantine for 2 weeks was also mandated for discharged patients and the family members of the hospital staff. The police force was employed to ensure that no one entered or left illegally. Punishment of violators of the quarantine order (including refusal to come back to the hospital) consisted of both a fine and revocation of professional certification.
After the “sealed off” order, chaos ensued and continued for several days. The plan called for all recognized SARS patients to be immediately isolated and grouped into cohorts on 2 floors of the hospital. In assessing the risks and benefits, many management challenges were not considered. The forming of cohorts was not completed for 24 hours owing to limited and constrained resources. The overall implementation did not consider the 3S model that supports surge capacity to balance Stuff (supplies and equipment), Staff, and Structure.Reference Kaji, Koenig and Bey 18 - Reference Hick, Koenig, Barbisch and Bey 20 Even after isolation, medical staff who had contracted SARS broke protocol in order to care for non-SARS patients because personnel were inadequate for the increased patient care needs (staff in the 3S model). The space (structure in the 3S model) to accommodate the large numbers of people was inadequate. Staff were initially sleeping on the floor in the hallways; by the second day sleeping quarters were established outside the hospital. Six individuals with different exposure levels shared a room and the same transportation vehicle, leading to additional cross-contamination risk. PPE and disinfection materials were distributed, but supplies (stuff) were limited and inadequate for all care providers, especially for those caring for non-SARS patients. The challenge of maintaining strict protocols for isolation and quarantine continued. Frustration in the hospital boiled over when the staff began vociferously complaining about their treatment; SARS patients who should have been in isolation were being kept with them and everyone was at risk of eventually contracting the disease. HCWs were forced to witness some of their colleagues get sick and die. The staff felt strongly that they were being treated like prisoners; their dedication to work diminished. Some doctors and nurses tried to flee, others refused to provide care to the patients. Telephone lines and television cables were cut, and security reasons were cited, adding to the fear and mental stress of the persons in containment. By the third day, a videoconferencing system was erected to allow family members of those quarantined and isolated in the hospital to communicate with the detainees.
The risk of psychological impact was evident on the third day of confinement, when a depressed man who was suspected of having SARS hanged himself in the hospital despite psychiatric counseling. The following day, another suicide attempt was aborted by others who prevented an individual from jumping from one of the hospital windows.
Despite active surveillance within the hospital, SARS cases continued to increase. On the fourth day, the policy was changed. Authorities began moving SARS patients to other hospitals. By the seventh day, some, but not all, asymptomatic care providers were relocated to another lodging place for an additional 14 days of quarantine. Finally, on May 8, the 15th day after the confinement, all asymptomatic people were relocated for another quarantine course. During this period, a total of 81 SARS patients in isolation were transferred to 15 hospitals throughout Taipei. Within the first months after the hospital quarantine, a total of 137 probable SARS cases were associated with exposures at this hospital, including 45 cases (33%) among HCWs with 26 (19%) deaths, higher than the national average (15%).
Other public health measures were available that could have led to better outcomes. The day after the Hoping Hospital quarantine plan, reports indicated that there were a total of 250 SARS-related cases reported nationally. Department of Health documents indicated that there were 253 available isolation beds out of the national capacity of 778 patient care beds in isolation wards. They announced plans to summon 1300 volunteer medical staff, including 300 doctors and 1000 nurses. There was appropriate S3 to surge to meet care demands to manage the SARS outbreak. Excess Staff were available in the volunteer plan, adequate Stuff was available in the appropriate care environments, and the Structure existed in the isolation-ward patient capacity for symptomatic patients. Quarantine as it was implemented resulted in increased mortality while concurrently impeding the personal freedom of asymptomatic individuals.
Discussion
The use of quarantine introduces significant secondary and tertiary effects. Regardless of the disease, the decision to invoke quarantine should consider and assess projected best outcomes. Those outcomes should be weighed with the potential negative impacts of the intervention. In the case of SARS, the roughly 10% mortality rate and spread via the droplet route supports the decision to immediately isolate symptomatic individuals. The suspected SARS source case presented to the ED 15 days before the hospital quarantine was initiated. Additionally, another hospital staff member presented with SARS-like symptoms 10 days before. They were not isolated. During the interim, more than 10,000 outpatients and visitors and more than 5000 family members of hospital staff, as well as many discharged ward patients, had been potentially exposed. There was no process to identify or evaluate those potentially exposed individuals. At the decision point to consider quarantine, health administrators detected the outbreak too late for implementation to be a reasonable course of action; SARS had already spread to the entire community. A review of the SARS outbreak in Toronto found quarantine inefficient and ineffective and opined that it had likely played no role in the control of disease spread.Reference Schabas 21
In considering the decision to quarantine, leaders must recognize that if applied inappropriately, quarantine actions themselves may cause harm to both individuals and society. First, disease transmission may increase in the quarantined population if symptomatic persons are not isolated immediately or if the disease is one (unlike Ebola or SARS) that is contagious prior to symptomology onset. The logistical challenges of separating isolated individuals from those under quarantine can be overwhelming. If persons with clear evidence of infection are placed in cohorts together with persons with no evidence of infection, increased transmission may result. Furthermore, symptomatic patients may have diseases that mimic the disease of interest (e.g., malaria rather than Ebola) and thereby may be put at risk of contracting illness even when put in cohorts with people with evidence of infection.
In the SARS case study, all medical workers, patients, and visitors were immediately and forcibly quarantined inside the hospital where they were at serious risk of cross-infection as a result of a shortage of protective gear and a lack of internal segregation based on the level of their exposure. Although the hospital could obtain supplies from external sources, the space within the facility was limited, thus restricting effective surge capacity. Hospitals typically have no excess capacity to sustain staff, including sleeping, eating, and recreational activities. Staff, with variable exposures, worked together with the infected/symptomatic and the asymptomatic patients. Healthy individuals were continually exposed to possible sources during the quarantine period, making it difficult to identify their last exposure. While theoretically the “quarantine period” started when they were moved to the quarantine area, the time in detention may have discounted their initial exposures, causing them to be quarantined for a longer time period than necessary. In addition, quarantined patients were cared for by HCWs who may have been infected, thus increasing the likelihood of exposure and subjecting them to an environmental hazard.
Another risk associated with quarantine is the unintended impact on patients admitted to the hospital for other medical problems. Patients with acute coronary syndromes, strokes, cancer, and traumatic injuries were all subjected to confinement. In addition, the perceived benefit of confining medical personnel to the hospital did not guarantee that patients would be provided with timely and quality medical care.
In the case of SARS, patients with multiple diagnoses were cross-contaminated within the crowded hospital, adding to their health risks. In the case of Ebola, patients with malaria and dengue fever may be confined with Ebola patients. Given the risk, the benefit of this strategy may not outweigh the health risk to the large number of individuals affected.
The efficacy of a large-scale hospital quarantine is questionable. Many unknowns exist during the initial emergence of a new infectious disease. The projected incubation and contagious periods are likely to change. Furthermore, the modes of transmission may initially be unclear, e.g., droplet vs. airborne. In the case of SARS, the incubation period was long and the contagious period was still under investigation. There was no scientific basis or plausible criteria to determine who should be quarantined. Even if criteria had been established, more than 10,000 patients and visitors were exposed. The logistics of effectively implementing the quarantine for a population that large are virtually impossible. In review, the criteria used in this case of SARS were not evidence based; many exposed individuals were missed, and many were included with no significant risk of spreading the disease. Such measures are unethical; however, in urgent situations this principle is often disregarded or misunderstood.
Psychological stress is another risk for those confined because of a quarantine order. The psychological impact is derived from two sources: (1) the fear and ambiguity of the disease and (2) incarceration. Patients with SARS reported fear, loneliness, boredom, and anger, and they worried about the effects of quarantine and contagion on family members and friends.Reference Maunder 22
Staff were adversely affected by fear of contagion and of infecting family, friends, and colleagues. In the Prince of Wales Hospital in Hong Kong and the Ton Took Seng Hospital in Singapore, there were “dirty teams” who selflessly dedicated themselves to treating SARS patients. Hospital workers in Taipei Municipal Hoping Hospital, including those who were not directly involved in patient care, were forced to perform duties within a perceived unsafe environment. Communications with others outside the hospital were interrupted. Quarantine procedures were changed from one hour to the next. The perception of personal danger was exacerbated by uncertainty. Confinement to a small area for a prolonged period of time while facing the threat of a potentially lethal disease caused a sense of collective hysteria, driving the staff to desperate measures, including suicide.
Conclusion and Recommendations
Quarantine presents complex challenges. Determining effectiveness and equitable application of policies is difficult, especially with the associated issues of personal liberties. Controlled movement, exclusion from local or long-distance public transportation, and exclusion from (high-density) public or work places all represent graded public health strategies to control disease transmission. Any such restrictions of movement must be evaluated for efficacy: Is the action supported by evidence of improved outcomes? Can it be effectively implemented given the need for balanced S3 (stuff, staff, and structure) surge? Will it lead to unintended negative outcomes? Are other less restrictive public health measures such as monitoring and social distancing equally effective? Finally, given the impact on civil liberties, is it reasonable and is it enforceable? A decision tree to assist policy makers and public health officials in quarantine and isolation decisions is presented in Figure 2.

Figure 2 Quarantine and Isolation Decision Tree. © 2014 Barbisch & Koenig. Reprinted with permission.
In our increasingly global world, diseases transmissible via the airborne route will theoretically be spread throughout the population before they are contained, making quarantine ineffective and unmanageable.Reference Zeng 23 On the other hand, diseases that are transmissible through direct contact before symptoms occur may be contained through quarantine if and only if they are managed appropriately. The characteristics of the specific pathogen, especially whether it is transmissible from person to person prior to the onset of symptoms, should determine what strategies public health officials employ. More studies should be undertaken to review the legal tenets underpinning quarantine and to determine the characteristics of an emerging infectious disease that would warrant quarantine.
Those responsible for political decisions to quarantine must consider evidence-based data likely to lead to improved outcomes before they suspend civil liberties. Public health officials have the responsibility to demonstrate political leadership by publicly providing medically sound, honest and frank assessments of risk. Officials should avoid unrealistic reassurances or taking unnecessarily stringent measures in their efforts to appear decisive. In most infectious disease outbreak scenarios, other more effective and less restrictive public health strategies and alternatives to large-scale quarantine exist. Any intervention must be medically defensible in its effectiveness to contain the spread of disease and protect against threats to the public health. In addition, it must be implementable, that is to say, the governing authority must be willing and able to monitor and enforce the projected number of individuals subject to the law.
Questions remain. Can a government really monitor even a small percentage of the exposed population that might be subject to quarantine? What actions would be taken if people were noncompliant? Finally, the intervention should not exacerbate the outbreak and generate unintended adverse consequences. In the case of Ebola, this includes the unwillingness of HCWs to travel to West Africa to eradicate the disease at its source for fear of being quarantined upon their return to their home countries.
Should quarantine be an option, clarification of quarantine (the asymptomatic) as opposed to isolation (the symptomatic) is imperative. Once implemented, placing the symptomatic (who should be isolated) in cohorts with the exposed (who may be subject to quarantine in a disease that is transmissible prior to symptom onset) is an inappropriate albeit relatively common action. Persons with clinical or laboratory signs or symptoms of a contagious disease should be isolated, separate from those who do not have clinical or laboratory evidence of infection. Policies should be based on transmission route and effectiveness and should balance individual freedom with public health concerns. Population-based public health intervention strategies of quarantine, such as widespread use of masks as appropriate, with instructions understandable by laypersons; disease etiology-based reporting of travel plans and levels of home restrictions or social distancing; restrictions on assembly of groups; and even closure of some mass public transportation systems and mass gathering areas should be analyzed for effectiveness.
In the case of SARS as well as Ebola, potential exposure and level of risk are variable, adding to the challenge of determining who might be the target as well as what level of quarantine (if any) is appropriate. This is especially challenging in light of the need to balance personal freedom and enforcement issues. With the availability of real-time syndrome-based case data and analytic capacity and capability, public health leadership can identify potential cases to provide more appropriate disease containment decisions. Quarantine should be reserved for situations in which it is supported by scientific evidence.