

During any mass gathering, the potential exists for deadly human stampedes to occur due to complex yet incompletely understood interactions between natural instincts of self-preservation and impulse-driven crowd behavior. Improved collective understanding of human stampedes has crucial planning implications and is indispensable in mitigation of this unique form of crowd disaster. Human stampedes, referring to either trampling or asphyxiating crushes with mass casualties, have been reported in numerous settings. Although the majority of stampedes have occurred in connection with sporting events, music concerts, political demonstrations, major celebrations, or religious gatherings, other gatherings have resulted in human stampedes with numerous injuries and deaths.Reference Ngai, Burkle and Hsu1–Reference Ahmed, Arabi and Memish8 A classification scheme for grading the severity of human stampede disasters based upon reported deaths has been recently proposed.Reference Ngai, Burkle and Hsu1 Unlike with many other types of disasters, no comprehensive catalogue of these events has been available, leaving major gaps in the current general understanding of human stampede epidemiology. With relatively few reports in the peer-reviewed literature, the full spectrum of causative and mechanistic factors that may contribute to the toll of stampedes remains unclear. Other information sources, such as news reports and the Internet, are increasingly sought out to better understand this important recurring phenomenon. Without incorporating nontraditional sources, no other way to reasonably acquire sufficient data is available. In this article, we analyze an inclusive database of human stampede events from 1980 to 2007 to identify epidemiological characteristics associated with increased mortality.
METHODS
Primary Search Method
A LexisNexis search was performed using the search term “stampede” for headline, search terms “stampede” and “injur*” for body, source: News (all, English, full text), with the option “all available dates.” Only human stampede events with description or approximation of the number of injuries and/or deceased were included. Any events involving fire, bombing, or terrorism were excluded. The search resulted in 1422 articles between January 1, 1980 and December 31, 2007. All of the articles were read and reviewed using “full with indexing” and 136 human stampede events were identified.
Secondary Search Method
Multiple Internet-based English-language news agencies were sequentially searched in the following order: the British Broadcasting Corporation (BBC) News (archives available since 1998), the New York Times (archives available since 1981), Arab News (archives available since 2001), CNN, and Reuters. From the BBC News home page (http://newssearch.bbc.co.uk), a search using the word “stampede” yielded articles with the key word “stampede” in its title or body. Each article was reviewed; 49 events were identified. A similar search method was conducted on the New York Times homepage (http://www.nytimes.com/ref/membercenter/nytarchive.html) with 12 additional events identified, followed by Arab News (http://www.arabnews.com) with 2 additional events identified, CNN (http://www.cnn.com) with 13 additional events identified, and Reuters (http://www.reuters.com) with 1 additional event identified.
Supplemental Searches
Supplemental Internet searches were conducted on PubMed (http://www.ncbi.nlm.nih.gov/pubmed), Wikipedia (http://enwikipedia.org/wiki/Stampede), crowddynamics.com (http://www.crowddynamics.com/Main/Crowddisasters.html), and mapreport.com (http://mapreport.com/subtopics/d/3.html) with the search term “stampede” to identify additional unique events. Two additional events were identified by this method.
Data Abstracted
The following information from each human stampede was recorded: date of the event, country, geographical region, time of occurrence (day vs night), type of event (sports, religious, music/movie, political, and others, denoted as nonsports nonreligious nonmusic/movie nonpolitical [non-SRMP]), location (indoor vs outdoor), mechanism (unidirectional, turbulent, and unable to determine), number of participants (if known), number injured (if known), and number of deaths (if known). Each country was designated as “developed” or “developing” according to acknowledged sources.9 Human stampede events were mapped using GIS software (ArcView GIS v9.3, ESRI, Redlands, CA). Reports of total injuries and event participants were frequently available only as estimates. By the study convention, descriptive estimates were converted to corresponding numerical estimates: When the number of injuries/participants was reported as “few” or “several,” 5 was used as an approximation; for reports of “scores,” 20 was used as an approximation; and any other indeterminate numbers were recorded using the lowest range (eg, 200+ was recorded as 200, “thousands” was recorded as 1000).
Statistical Analysis
Descriptive analysis was first performed for deaths and injuries. Bivariate analyses of number of deaths or injuries according to stampede characteristics were conducted using a nonparametric Wilcoxon rank test. Multivariate regression under Poisson distribution on number of deaths was performed to determine the factors associated with increased number of fatalities during human stampede events. Adjusted relative death counts by event characteristics in the final multivariate regression model were estimated. The identical descriptive and bivariate analytical approaches were conducted to determine fatality rates in the subgroup of events with available estimates of participants. A negative binomial model was used to account for overdispersion in the fatality rate data and the multivariate model was adjusted for the size of population of participants in each event by incorporating the logarithm of the population size as an offset term.Reference Diekman, Ballesteros and Berger10 Adjusted relative fatality rates and their corresponding 95% confidence intervals (CIs) were estimated from the multivariate model. Data were analyzed using Statistical Analysis Software (SAS) version 9.1 using PROC GENMOD (SAS Institute, Cary, NC).
RESULTS
Overall, a total of 215 human stampede events were reported from 1980 to 2007, resulting in 7069 deaths and at least 14,078 injuries from 213 events with available fatality information and 179 events with injury information. The average (±standard deviation) and median number of fatal cases per event were 33.2 (±128.2) and 5, whereas those of injured cases were 78.6 (±257.0) and 32. At events that had estimated numbers of participants, the range was between 100 and 30 million with a median of 12,000 and an interquartile range (IQR) between 1000 and 50,000. The geographical distribution of these events was shown in Figure 1. Characteristics of these stampede events were summarized in Table 1. The majority of reported events have occurred since 2000, particularly in developing countries from south Asia (27.9%) and Africa (25.1%). Most stampedes have taken place during the daytime and indoors. The greatest number of stampedes occurred in the setting of sporting events (22.8%), followed by religious (19.1%) and political (17.7%) gatherings. The mechanism of stampedes was approximately evenly attributed between unidirectional and turbulent flow.

FIGURE 1 Geographic information systems chloropleth mapping of human stampedes around the world (1980–2007).
TABLE 1 Distribution of Reported Human Stampede Events by Characteristics of Events, 1981–2007

In bivariate analysis, stampedes that occurred from 1980 to 1989 had a higher number of deaths than those from other calendar periods. Stampede events occurring in the Middle East, in developing countries, outdoors, or associated with religious events had the highest median number of deaths (Table 2). In multivariate analysis, events that occurred from 1980 to 1989 and 1990 to 1999 (vs 2000–2007); developing countries (vs developed); geographical regions including south Asia, east Asia/Pacific, the Middle East, Africa, and Europe (vs America); and outdoors (vs indoors) were associated with increased number of fatalities. Stampedes that occurred in the context of SRMP events (vs non-SRMP), or had a unidirectional mechanism (vs turbulent) also increased the relative number of deaths (Table 3).
TABLE 2 Median of Fatalities and Number of Injured in Reported Human Stampede Events by Characteristics of Events, 1980–2007
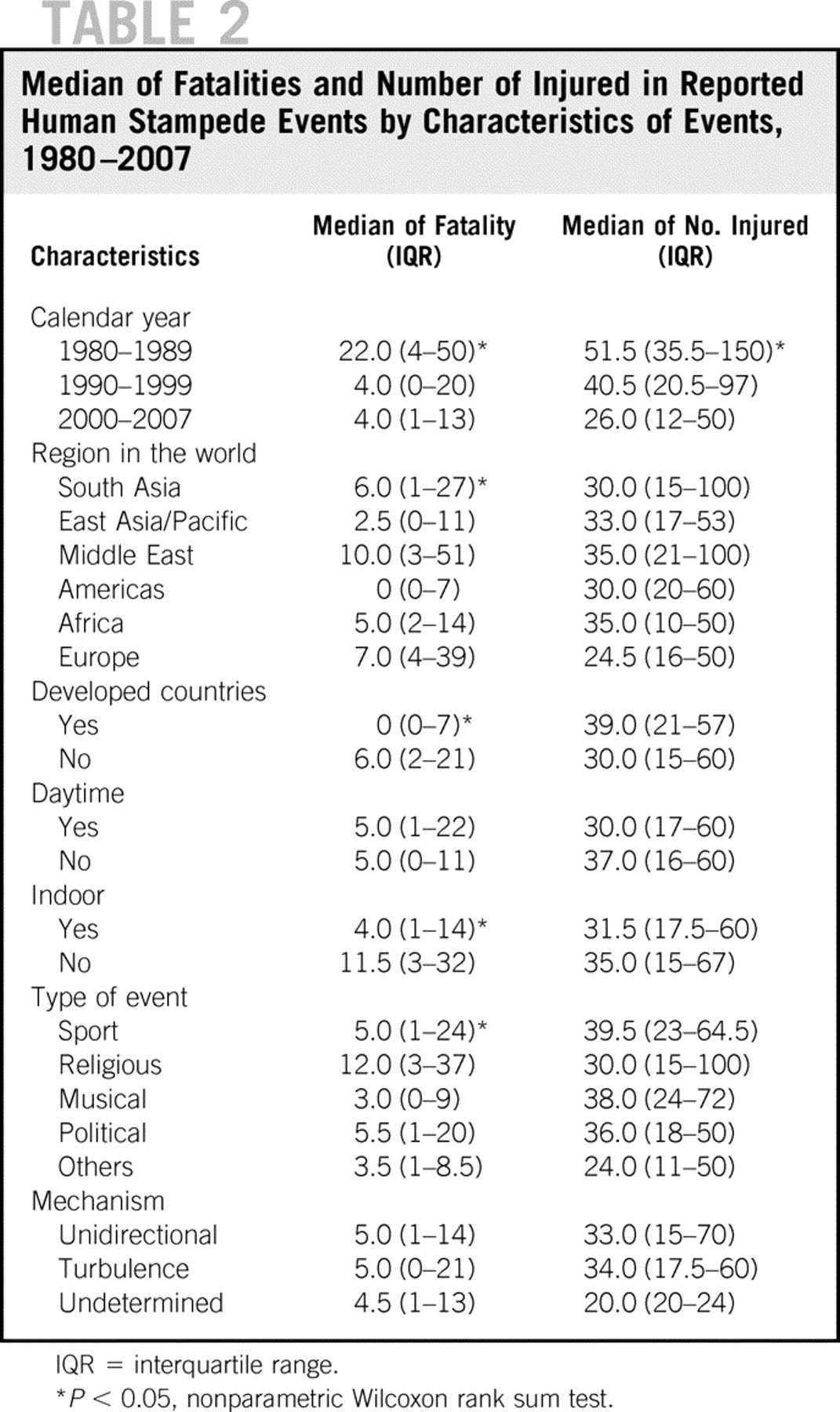
TABLE 3 Multivariate Analysis of Association of Factors and Number of Fatalities in Reported Human Stampede Events, 1980–2007

In the subgroup analysis of 133 events with estimated number of participants, median fatality rates were 32.5/100,000 with a range of 0 to 44,000/100,000 (IQR 6–315.0/100,000). Thirty-one (23.3%) events did not result in fatalities, 47 (35.3%) had a fatality rate of <100/100,000, and 55 (41.4%) had a fatality rate of ≥100/100,000. In bivariate analysis, geographical region, country developmental status, and type and mechanism of events were associated with fatality rate of events (Table 4). In the multivariate regression analysis, stampedes that occurred in the developing countries had a fatality rate 7.75 times higher than those occurring in the developed countries. Compared with sporting event–related stampedes, music, religious, political, and non-SRMP events had higher fatality rates between 4.4- and 40-fold. Unidirectional mechanism also increased fatality rates by 3.46 times compared with stampedes with turbulent flow (Table 5).
TABLE 4 Median of Fatality Rate and Number of Injured in Reported Human Stampede Events by Characteristics of Events, 1980–2007

TABLE 5 Multivariate Analysis of Association of Factors and Fatality Rate in 131* Reported Human Stampede Events, 1980–2007

DISCUSSION
Human stampedes are a relatively unique type of disaster that has not been systematically studied. Although occurrence of these events around the world has captured extensive media attention, limited scientific investigation has taken place. A recent literature review on the topic referenced just 8 human stampedes of the hundreds that have happened since the 1980s, mostly occurring in the United Kingdom or United States.Reference Ngai, Burkle and Hsu1–Reference Ahmed, Arabi and Memish8 Among these, only 1 detailed an event that ranked among the deadliest human stampedes in recent history.Reference Ahmed, Arabi and Memish8 The lack of high-quality epidemiological data represents a major barrier to better collective understanding of this recurrent phenomenon. In the absence of such information, all other existing primary sources deserve consideration. Although less precise, media sources can offer insight into patterns, characteristics, and major determinants of injury and fatalities that invariably result from these crowd disasters. During the early stages of epidemiological research on other disasters such as earthquakes, comparable approaches were taken to compile an initial record of events that could be studied.Reference Alexander11 Using this conceptualization, a comprehensive baseline of human stampede events was developed as a basis for further inquiry.
From 1980 to 2007, a total of 215 human stampede events were identified. The number of reported human stampede events has markedly increased during each decade since 1980—more than doubling between 2000 and 2007 from the prior decade—and this may be interpreted in several ways. Global demographic changes such as the expansive growth of densely populated geographic centers, some referred to as “megacities,” may lead to rising attendance at major mass gatherings and contribute to the striking increase of human stampedes over time. Alternatively, the increasing number of reported events may simply reflect increased sharing of available information via the ubiquitous nature of the Internet. Several major news sources have only recently begun to archive reports. More than likely, the rising number of human stampedes captured through the decades reflects a combination of these factors. Geographically, most reported stampedes have occurred in developing countries, notably in south Asia and Africa. It remains unclear whether societal, cultural, and behavioral norms in lesser developed countries may predispose crowd gatherings to greater likelihood of human stampede occurrence. Mass-gathering health care models have been proposed that incorporate psychosocial, biomedical, and environmental factors.Reference Arbon12 The extent to which limited organizational resources play a role deserves special attention. For instance, large scheduled events in developed countries are virtually always accompanied by strict crowd control measures enforced by security. In less developed settings, the absence of capacity regulations or sufficient crowd control measures combined with the sheer number and density of participants at an event in emotionally charged environments may set the stage for deadly human stampedes. The vast majority of stampedes have been associated with particular types of mass gathering events including sporting, religious, and political events that are geared to entertain, inspire, or thrill. Certain variables, such as event type, duration, crowd mood, and density have been linked to medical usage rates and general observed injury patterns.Reference Milstein, Maguire and Bissell13 Central attractions may further encourage the crowd to gather in higher densities, exceeding venue capacity. Resultant inadvertent physical contact, such as pushing and shoving, along with an absence of lines or orderly flow combine to create unsafe conditions. In contrast, an inciting event or even a rumor may prompt escape panic among the crowd with a frenzied, chaotic rush to exit. With either situation, escalating crowd density coupled with disruption of normal flow and movement speed may serve as early indicators of stampede potential.Reference Helbing, Farkas and Vicsek14, Reference Helbing, Johansson and Al-Abideen15
The highest median deaths occurred with stampedes during 1980 to 1989. This does not necessarily imply that human stampedes during that period were of increased severity or exacted a greater human toll. Rather, this may point to an earlier tendency for preferential reporting of only major events. Conversely, the increased reporting of virtually all human stampedes including less noteworthy events with few or no fatalities in more recent decades has a dilutional effect. As previously discussed, it is not surprising that the highest median fatality rates came from developing as opposed to developed countries. Human stampedes occurring outdoors or in the context of religious events and in Middle Eastern countries were observed to have among the highest number of fatalities. This reflects the recurrence of large-scale outdoor crowd disasters that have taken place during the Hajj through the years. Five of the top 10 deadliest human stampedes during the past 100 years have transpired in Mina Valley, Saudi Arabia, during the Hajj.Reference Ngai, Burkle and Hsu1 In addition, the third deadliest human stampede happened during a religious festival in Iraq in 2005.Reference Ngai, Burkle and Hsu1
It could be contended that the vast numbers of pilgrims present during these religious celebrations are orders of magnitude greater than those in attendance at other events and thus, numbers of deaths alone are not the most representative measure. Calculation of fatality rates offers a more evenly balanced comparison taking into account participants in attendance with widely varying event sizes. As would be anticipated, the number of participants at an event does markedly affect relative fatality rates when a human stampede occurs. Based upon subgroup analysis of 131 events for which the estimated number of participants was available, multivariate analysis revealed that although relative fatality rates at religious events were higher than for sports and musical events, they were not the highest. Of note, political events were associated with a markedly higher relative fatality rate. Non-SRMP settings had the highest relative fatality rate, more than 40 times greater than sports settings. A plausible explanation is that sporting events, religious celebrations, music events, and political gatherings are for the most part considered to be preplanned events. Thus, most are likely to have at least some rudimentary crowd control measures or security for prevention of large-scale crowd disasters and perhaps some predeployed basic medical resources. In some cases, for example, during the Hajj, preparations taken in response to previous crowd disasters are extensive and include measures such as construction of multilevel structures capable of handling tremendous capacity with plentiful entry and exit points supported by electronic surveillance.Reference Ahmed, Arabi and Memish8 This contrasts sharply with non-SRMP events that may be considered largely unplanned or impromptu mass gatherings. Without any preparation for crowd management, it becomes apparent that when a human stampede occurs, there is potential for the outcome to be far more deadly.
The developmental status of the country in which a stampede takes place is also an important factor associated with fatality rates. A nearly 8-fold higher fatality rate from stampedes in developing countries versus developed countries was demonstrated by the subanalysis. Once again, the lack of available resources to support large-scale event planning may lead to inadequate crowd control measures, which in turn result in human stampedes that are considerably more severe. Another contributing factor is the state of less sophisticated prehospital and hospital systems in developing countries. Restricted personnel and resources for treating stampede victims may account for the failure to prevent deaths that may be otherwise salvageable in settings with better health system infrastructure and advanced medical care.
Although the exact inciting factors are in some cases difficult to discern, the mechanism of human stampedes may generally be categorized as unidirectional or turbulent.Reference Ngai, Burkle and Hsu1 Whether a large crowd will flow unidirectionally or merge from different directions and become turbulent can be determined with reasonable certainty. The distribution of unidirectional (49.3%) and turbulent mechanisms (46.1%) was approximately equal along with median fatalities and injuries across all human stampedes; however, relative numbers of deaths and median fatality rates were both higher in unidirectional stampedes. Multivariate analysis of the subgroup with estimated event participants showed an even higher relative fatality rate for unidirectional versus turbulent mechanism stampedes. The authors suggest that an explanation for why a unidirectional mechanism is more lethal is that the forces generated by pushing in a single direction are greatly increased, whereas pushing in many directions simultaneously results in vector cancellation. The tremendous force created by 6 to 7 people pushing in a single direction has been reported to exceed the force required to bend steel railings.Reference Elliott and Smith3, Reference Smith and Dickie16 These crushing forces may translate into increased deaths during crowd disasters.
There are several important limitations to this study. Internet and media sources were used as primary sources because no other more accurate or accessible source for information pertaining to stampedes was available. Before the advent of the Internet, there may have been a reporting bias toward events with higher injuries and deaths and a tendency to neglect stampedes in which few or no casualties occurred. As previously discussed, this may partially explain the higher median deaths during 1980 to 1989. During this earlier period, there may also have been comparatively greater reporting from developed countries. Over time, technological improvements in communications have likely facilitated increased uniformity in reporting of events. Although the exact number of deaths following a human stampede are presumed to have been accurately reported, independent verification was beyond the scope of this study. Injury and event participant was incomplete: 99% of reported events contained fatality information, whereas 83.3% had injury information and 60.9% had event participant estimates. Reported numbers of injuries and participants at events were less reliable, but they served as a reasonable approximation. In certain cases, descriptive words such as “few” or “dozens” rather than numbers were used to quantify injuries. By study convention, these descriptions were translated to corresponding fixed estimates. By applying the most conservative values for descriptive terms, the impact of these estimation procedures was minimized.
CONCLUSIONS
Whereas there is considerable interest in exploring the concept of relative injuries and injury rates that occur during human stampedes, the imprecise quality of available injury data precludes further informative analysis. The need for adopting a more evidence-based approach to mass gathering planning is well recognized and may improve provision of health care.Reference Arbon17, Reference Arbon, Bridgewater and Smith18 At this time, however, there is no other way to reasonably acquire a sufficient body of data to study. Because no widely available database of human stampede events exists, further development of this type of resource is essential for future investigation. Accordingly, the systematic prospective collection of epidemiological data by appropriate multiagency investigative teams immediately following future human stampedes is strongly recommended. To our knowledge, this is the first attempt to examine epidemiological characteristics of human stampedes and identify specific factors associated with increased mortality. Considerable further study of human stampedes as a recurrent, distinctive type of disaster is warranted.
Acknowledgments
The authors gratefully acknowledge Timothy Shields, from the Johns Hopkins Bloomberg School of Public Health, for assistance in representative mapping of human stampede events.
Authors' Disclosures
The authors report no conflicts of interest.






