The current Ebola outbreak in West Africa is the largest in history. 1 The large number of infected health care workers (HCWs) 2 has brought additional attention to the need for effective personal protective equipment (PPE). PPE such as gloves, gowns and coveralls, surgical masks and respirators, aprons, face shields and goggles, and caps and hoods prevents the virus from entering the body through the mucous membranes (e.g., eyes, mouth, nose) and disruptions in the skin (e.g., cuts, scrapes, cracked skin). Respirators can reduce potential transmission of body fluids during aerosol-generating medical procedures, although the risk of transmission is not well understood.Reference Pshenichnaya and Nenadskaya 3 , Reference Macintyre, Seale and Yang 4 Anecdotal reports from HCWs in West Africa indicate that, owing to high ambient temperature and humidity, some personnel can wear PPE for only 40 minutes at one stretch.Reference Wolz 5 , Reference Chertow, Kleine and Edwards 6 Employees in many workplace settings (e.g., construction, agriculture, wild land firefighting, hazardous materials response, manufacturing) wear PPE for extended periods of time in hot, humid, and extremely challenging environments similar to those currently being experienced by HCWs in West Africa. PPE reduces the ability of the wearer to cool off by limiting heat transfer from the body via the normal physiological processes of sweat evaporation, convection, and radiation. Also, PPE adds to the burden of weight carried (PPE weighs from 3.8 to 4.2 kg depending on the combination of items used), thus further increasing the metabolic heat burden and physical exertion. However, the challenges faced in selecting PPE for the current Ebola outbreak in West Africa are unique in that consideration must be given to the selection of work and rest cycles to mitigate heat stress, 7 which is constrained by the availability of single-use PPE, high patient loads (i.e., more or longer rest breaks are not practical), the desire to reduce the frequency of doffing PPE because of the risk of exposure, and the high mortality rate and highly infectious nature of the virus.
Selection of PPE requires balancing issues such as heat stress and comfort with providing the appropriate level of protection. This tradeoff is not unique to the Ebola outbreak. To provide adequate protection, PPE designers often must make certain tradeoffs; sometimes, these include material choices (e.g., use of impermeable materials to block blood and body fluids containing infectious materials from coming in contact with the body) that make the PPE less breathable and thus less comfortable for the wearer because of the additional heat stress. During the care of patients with Ebola virus infection, reducing protection is not a viable option; thus, the focus is on the management of heat stress. The industrial hygiene community has decades of experience in developing strategies to manage heat stress, including work-rest cycles and “clothing adjustment factors” that take into account the role of clothing in reducing dry heat exchange (i.e., convection, radiation) and resistance to evaporative cooling to account for the extra PPE burden.Reference Bernard, Caravello, Schwartz and Ashley 8
Thermal manikins have been in use since 1940,Reference Holmér 9 and research has demonstrated that a sweating thermal manikin is useful for estimation of the dry and evaporative heat loss from a clothed body at user-defined temperature and humidity conditions.Reference Meinander and Hellsten 10 , Reference Holmér 11 In response to the pressing issue of Ebola-related PPE concerns, the National Institute for Occupational Safety and Health (NIOSH) has undertaken a sweating thermal manikin evaluation of PPE ensembles similar to those used in the past year in West Africa under prevailing ambient conditions. This is part of NIOSH’s work with national and international collaborators to develop solutions to improve PPE configurations for present and future use. The focus of the present study was to provide a baseline heat stress analysis of some of the PPE ensemble options used in West Africa in the fight against the spread of Ebola.
METHODS
A sweating thermal manikin (Newton sweating thermal manikin; Measurement Technology Northwest, Inc, Seattle, WA) with a standard 34 heat/sweat zone configuration (the manikin is divided into 34 “body” areas to evaluate specific body zones as well as the whole body as a human being) was used to test physiological and subjective perception responses to wearing PPE. The manikin is regulated by a software package adapted from the RadTherm finite difference thermal analysis program (ThermoAnalytics, Inc, Calumet Township, MI) that implements the Fiala thermoregulation model.Reference Fiala, Lomas and Stohrer 12 , Reference Fiala, Lomas and Stohrer 13 The manikin generates metabolic heating levels as programmed by the regulation model, depending on clothing and environmental conditions, and allows for computation of thermal comfort and thermal sensation perceptions from the temperature data that predict local and global thermal comfort as a function of local skin and core temperatures and their rates of change.Reference Rugh and Lustbader 14 - Reference Zhang, Arens, Huizenga and Han 17 The thermal manikin model has a maximum sweat rate of 30 g/min (1.8 L/h), which is an approximation of the maximum human body sweating capacity experienced by individuals wearing protective clothing while engaged in light-intensity exercise.Reference Sawka and Montain 18
Test Conditions
The studies were carried out in an environmental chamber programmed at the “near worst-case” conditions that HCWs would face in the warmest months of the year in West Africa (condition A, 32°C, 92% relative humidity [RH]). A second set of experiments was carried out at the highest conditions reported for September 26, 2014, in Monrovia, Liberia (condition B, 26°C, 80% RH). To replicate the HCWs’ activities, the metabolic work rate (work intensity) was set to the average for nursing (corresponding to patient care that includes standing and walking slowly [2.5 mph] and carrying light objects [<11.3 kg]) of 3 METs (metabolic equivalent, or the measure of the intensity of aerobic exercise) over 80 min of continuous activity.Reference Ainsworth, Haskell and Herrmann 19
Test PPE Ensembles
Five different PPE ensembles were tested during the months of September and October 2014. These were as follows:
-
(1) The control ensemble consisted of reusable medical scrubs (65%/35% polyester/cotton pullover shirt and pants with drawstring waist cincture [Fundamentals, White Swan, Ballwin, MO]) with cotton socks and mid-calf-length rubber boots (OnGuard, Havre de Grace, MD) (Figure 1).
-
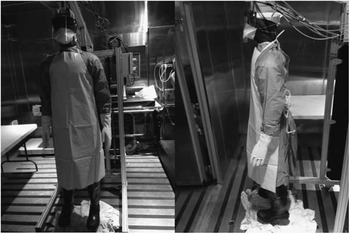
(2) Ensemble 1 (E1) consisted of medical scrubs, socks, and rubber boots with a mid-calf-length, disposable, fluid-resistant surgical gown (High Performance Surgical Gown 7696C; 3M, St. Paul, MN); a fluid-resistant 3-ply surgical mask (Technol Anti-Fog 49235; Kimberly Clark, Halyard Health, Roswell, GA); a disposable polyester lens face shield (FisherBrand Anti-Fog 19-460-10; Fisher Scientific, Pittsburgh, PA); and disposable nitrile examination gloves (Better Touch; CABVI, Utica, NY) (Figure 2).
-
(3) Ensemble 2 (E2) consisted of medical scrubs, socks, and rubber boots with a mid-calf-length, disposable, fluid-resistant surgical gown (High Performance Surgical Gown 7696C; 3M), a polyethylene surgical apron (A70; KleenGuard, Kimberly Clark), a face shield (FisherBrand Anti-Fog 19-460-10; Fisher Scientific); disposable nitrile examination inner gloves (Better Touch; CABVI); heavy-duty nitrile outer gloves (Assurance model 50-N-242064; Protective Industrial Products, Inc, Latham, NY); a duckbill N95 surgical filtering face piece respirator (Kimberly Clark model 46828); and a fluid-resistant surgical cap (Kimberly Clark KCH69240) (Figure 3).
-
(4) Ensemble 3 (E3) consisted of medical scrubs, socks, and rubber boots with a Tyvek coverall and separate custom-made Tyvek hood with an integrated splash-resistant surgical mask (Dupont, Wilmington, DE); a rubber surgical apron (Europrotex, La Bernadière, France); splash-resistant goggles (Bollè Duo, Oyonnax, France); surgical nitrile inner gloves; heavy-duty nitrile outer gloves; a duckbill N95 filtering face piece respirator (Kimberly Clark model 46828); and a fluid-resistant surgical cap (Kimberly Clark KCH69240) (Figure 4).
-
(5) Ensemble 4 (E4) consisted of medical scrubs, socks, and rubber boots with a Tychem QC highly impermeable coverall (Dupont); Médecins Sans Frontières (MSF) custom-made Tyvek hood with an integrated splash-resistant surgical mask; rubber surgical apron; splash-resistant goggles; surgical nitrile inner gloves; heavy-duty nitrile outer gloves; a duckbill N95 filtering face piece respirator (Kimberly Clark model 46828); and a fluid-resistant surgical cap (Kimberly Clark KCH69240) (Figure 5).

Figure 1 Control ensemble front and side views.

Figure 2 Ensemble 1 front and side views.

Figure 3 Ensemble 2 front and side views.

Figure 4 Ensemble 3 front and side views.

Figure 5 Ensemble 4 front and side views.
Test Measurements
The manikin was programmed to provide data on body core temperature (T co, °C), body surface skin temperature (T sk, °C), sweat rate (SR, g/min), thermal comfort (rated from −4 [very uncomfortable] to 4 [very comfortable]), and heat sensation (rated from −4 [very cold] to 4 [very hot]) (Table 1).
Table 1 Time to Reach Core Temperature (T co) of 39 °C in the 5 Ensembles and skin temperature (T sk), Heat Sensation, and Comfort at 80 min of TestingFootnote a

a Abbreviations: RH, relative humidity; PPE, personal protective equipment. T sk, body surface skin temperature. Condition A is 32 °C and 92% RH; condition B is 26 °C and 80% RH. n=3. Control PPE for condition B was not included in the statistical analysis because only 2 replicates were collected.
b-fSuperscript numerals indicate pairs of values that differ significantly (P<0.05), where b=control, c=ensemble 1, d=ensemble 2, e=ensemble 3, and f=ensemble 4.
Statistical Analysis
Each test was replicated 3 times and all variables measured were first calculated as mean and standard deviation for each PPE ensemble (independent variable). The dependent variables were time to reach 39°C T co (attaining T co of 39°C over 1 hour is associated with decrements in simple mental performanceReference Hancock and Vasmatzidis 20 ), T sk, and subjective measures (thermal comfort and heat sensation). A repeated-measures analysis of variance (ANOVA) was used to determine the main effects of each variable. The least significant difference (LSD) test was chosen for post hoc pairwise comparison. Statistical significance was accepted when P < 0.05.
RESULTS
Condition A
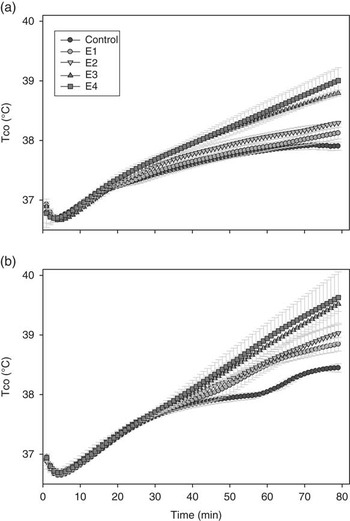
The increase in T co over time during 80 min of continuous PPE wear at ambient conditions of 32°C and 92% RH is shown in Figure 6B. The time to reach the critical T co of 39°C was significantly less for the E4 (62±6 min) and E3 (65±3 min) PPE ensembles than for the E2 (78±7 min) (P=0.04). The control and E1 ensembles never attained a T co of 39°C during the 80-min test period. T sk was significantly higher for the E4 and E3 ensembles than for the control and E1 ensemble (P=0.01 for both comparisons) and for the E2 compared with the control (P=0.04). The E3 and E4 ensembles had significantly higher ratings of heat perception (P=0.01 and 0.02, respectively) and discomfort (P=0.04 for both comparisons) than did the control (Table 1). All PPE ensembles, except the control, reached maximum sweat rate capacity (30 g/min) by the end of the 80-min test period.

Figure 6 Dynamic of Core Temperature (T co) for the 5 Ensembles Over the 80-Minute Test Duration at Ambient Conditions of (A) 26°C and 80% RH and (B) 32°C and 92% RH. Abbreviation: RH, relative humidity. Values are mean ±SD.
Condition B
The increase in T co over time during 80 min of continuous PPE wear at ambient conditions of 26°C and 80% RH is shown in Figure 6A. None of the PPE ensembles achieved a T co of 39°C, although the E4 and E3 ensembles approached that level. The E4 ensemble was associated with a significantly higher T co than the E1 and E2 ensembles (P=0.01 and 0.03, respectively), as was the E3 ensemble (P=0.01 for both comparisons). The T co of the E2 ensemble was significantly higher than that of the E1 ensemble (P=0.03). T sk was significantly higher for the E4 than for the E1 and E2 ensembles (P=0.01 and 0.0, respectively). The E4 ensemble was associated with a higher rating of heat sensation than the E1 (P=0.03) and approached statistical significance for higher heat sensation compared with the E3 and E2 ensembles (P=0.07 and 0.05, respectively). The E4 ensemble was associated with more discomfort than the E1 and E2 ensembles (P=0.02 for both comparisons), whereas the E3 ensemble approached statistical significance for discomfort compared with these 2 aforementioned ensembles (P=0.05, 0.07, respectively) (Table 1).
DISCUSSION
Ensemble configurations similar to the E4 PPE studied here are currently in use by MSF health care personnel in Ebola-affected countries of West Africa. The results of the present study indicate that use of this ensemble results in significant heat stress after 1 hour of use in a “near worst case” ambient environment scenario (32°C, 92% RH) at a typical HCW work rate (3 METs). This supports anecdotal reports of HCWs being able to work only for periods of 40 to 60 minutes before the need for a rest period and doffing of the PPE.Reference Wolz 5 , Reference Chertow, Kleine and Edwards 6 The E3 ensemble, which includes a Tyvek coverall, exhibited a heat stress performance profile very comparable with that of the E4 ensemble, which is not surprising given that the E4 coverall is composed of Tychem QC, a fabric that is similar to (but more impervious to liquid and viral penetration than 21 ) Tyvek. This is in variance with recent research on clothing adjustment factors (CAFs) reporting CAFs (in °C of Wet Bulb Globe Temperature) of 1.0°C for Tyvek and 7.5°C for Tychem at a low work rate and 50% RH.Reference Bernard, Caravello, Schwartz and Ashley 8 In the current study, however, the E3 PPE included a relatively impervious rubber apron that covered the anterior torso from neck to mid-calf and would have further reduced heat release mechanisms. Although both the E4 and E3 ensembles demonstrated higher values for study parameters in condition B, the impact of the E3 ensemble was less than noted for condition A, except for T co (Table 1). The E4 ensemble, by virtue of the use of goggles versus face shield and Tyvek cape/hood versus surgical cap, affords additional coverage to areas of the face and neck that would be exposed with the E2 ensemble (Figures 3 and 5), but in condition B resulted in markedly higher (P=0.05) heat sensations than the other PPE ensembles (Table 1). This suggests that the encapsulation of the head and neck by the cape/hood and goggles has a greater impact on subjective perceptions of heat, but this supposition would require human trials to verify. The near-attainment of the critical T co of 39°C at 80 min of wear with both the E4 and E3 ensembles in condition B further illustrates that time of wear is a critical factor in the development of heat stress (Figure 6) when wearing these PPE ensembles at temperatures attained in the Ebola-affected countries. This is an important issue in determining work/rest cycles for HCWs in West Africa.
The sweating thermal manikin provides an additional important piece of information on heat production, which could be useful for future studies and could assist in developing solutions to the heat stress problems generated by wearing these PPE ensembles in similar ambient conditions. At the work load and environmental conditions of the current study, the heat production of the manikin for the control and PPE ensembles ranged from 290 to 320 Watts. Possible solutions would include cooling devices (ice-cooling vests or liquid cooling garmentsReference Kim, Coca, Williams and Roberge 22 ) that could compensate for heat generation of ~300 Watts by effectively removing a portion of the generated heat. The study data are good baseline estimations of the thermal stress imposed by the control and 4 PPE ensembles on a healthy, fit individual.
Limitations
There were several limitations to this study. First, human variability is not completely considered when using thermal models or thermal manikin testing; for example, fitness level, heat acclimatization (sweating response differences as the result of sex, race, age), hydration level at the start of the test, medication use, and health status could impact the results. Second, the work rate used in the current study (3 METs) may not represent an actual work rate, which could result in over- or under estimation of the actual work rate; also, the use of a continuous work rate over an entire work cycle is not generally analogous to actual workplace scenarios. Next, the model does not take into account the human movement effects (e.g., air movement around the PPE with activity) on PPE and the associated changes in the thermoregulatory response.Reference Bernard, Caravello, Schwartz and Ashley 8 Finally, a representative set of PPE ensembles ranging from simple coverage of the body with lightweight PPE (ensemble 1) to full coverage of the body (ensembles 3 and 4) were chosen. In practice, many combinations of these ensembles are used in the field that vary in terms of the level of protection to viral penetration (even though both the surgical gown and the Tychem coverall models used in this study both pass the ASTM1671 standard 23 ), as well as number of items used (for example, single surgical gloves vs. double gloving with surgical and heavy duty gloves; surgical cap under hood or just the custom-made hood). This study was carried out by using PPE ensemble combinations selected from internal PPE recommendations from August 2014 used to procure PPE for the Ebola response (Chad Dowell, personal communication). These recommendations were based on information on what PPE was commonly in use in West Africa at that time. The PPE components were similar to, but not identical to, the WHO and MSF recommendations in place at the time. 24 , Reference Sterk 25 The WHO PPE recommendations were updated in November 2014. 26
CONCLUSIONS
Sweating thermal manikin data indicated that the E4 and E3 PPE ensembles increased T co to a critical level of 39°C more rapidly than the control, E1, and E2 ensembles. Because the PPE ensemble configurations studied here are similar to the ensembles worn in West Africa for the Ebola outbreak, implementation of an appropriate work-to-rest ratio is recommended, as well as investigation of possible cooling strategies and other precautions that would alleviate the heat stress faced by HCWs. These measures will help to achieve thermal relief during the recovery periods, possibly allowing longer, but safer, work periods. The subjective impact of head and neck encapsulation on heat perception requires further investigation and could be ameliorated by the use of alternative equipment (e.g., powered air-purifying respirators with shrouds or more breathable materials for body and head protection).
Acknowledgments
The authors are sincerely grateful for the technical and experimental support in conducting the present study from NIOSH’s Emergency Preparedness and Response Office (Chad Dowell and Lisa Delaney), the CDC foundation, Susan Lovasic (Dupont), Ivan Ivanov and Rosa Costanza Vallenas (WHO), and Catherine Villegas (MSF).
Disclaimer
The findings and conclusions in this article are those of the authors and do not necessarily represent the views of the CDC. Mention of product names does not imply endorsement. The authors identify no conflicts of interest in the conduct of this study.