


Theories regarding developmental pathways to substance use and disorder explain the emergence and escalation of use that occurs in adolescence by identifying risk and protective mechanisms through a life course perspective (Hussong, Reference Hussong2011; Masten, Faden, Zucker, & Spear, Reference Masten, Faden, Zucker and Spear2008; Zucker, Donovan, Masten, Mattson, & Moss, Reference Zucker, Donovan, Masten, Mattson and Moss2008). Although not capturing all forms of use (e.g., late onset), developmental pathways are powerful theories for prevention science as they can inform when intervention should occur, who should receive intervention, and what factors should be altered by intervention (Ialongo et al., Reference Ialongo, Rogosch, Cicchetti, Toth, Buckley, Petras, Neiderhiser and Cohen2006). In the current study, we focus on two established developmental pathways to substance use, often referred to as the internalizing (Hussong, Jones, Stein, Baucom, & Boeding, Reference Hussong, Jones, Stein, Baucom and Boeding2011; Hussong, Rothenberg, Smith, & Haroon, Reference Hussong, Rothenberg, Smith, Haroon, Fitzgerald and Puttlerin press) and externalizing (Chassin, Sher, Colder, & Hussong, Reference Chassin, Sher, Colder, Hussong and Cicchetti2016; Hussong, Rothenberg, et al., Reference Hussong, Rothenberg, Smith, Haroon, Fitzgerald and Puttlerin press; Zucker, Reference Zucker, Cicchetti and Cohen2006) pathways. Drawing upon theories and methods of peer network models (Berkman, Glass, Bissett, & Seeman, Reference Berkman, Glass, Brissette and Seeman2000; Brechwald & Prinstein, Reference Brechwald and Prinstein2013; Ennett & Bauman, Reference Ennett and Bauman1993; Ennett et al., Reference Ennett, Bauman, Hussong, Faris, Foshee, Cai and DuRant2006, Reference Ennett, Faris, Hipp, Foshee, Bauman, Hussong and Cai2008), we tested whether social standing in school-based peer networks differentially mediates the association between risky symptoms associated with these pathways (i.e., depressive symptoms and deviant behavior) and within-person, time-specific increases in substance use, particularly during the transition to high school.
The Internalizing and the Externalizing Pathways
The internalizing and externalizing pathways delineate early emerging risk processes that, if unchecked, lead to problematic substance use over the early life course (Chassin et al., Reference Chassin, Sher, Colder, Hussong and Cicchetti2016; Hussong et al., Reference Hussong, Jones, Stein, Baucom and Boeding2011; Hussong, Rothenberg, et al., Reference Hussong, Rothenberg, Smith, Haroon, Fitzgerald and Puttlerin press; Zucker, Reference Zucker, Cicchetti and Cohen2006). The more widely recognized and robustly supported of these is the externalizing pathway (also known as the early starter model, the deviance proneness model, and the behavioral disinhibition model; Sher, Walitzer, Wood, & Brent, Reference Sher, Walitzer, Wood and Brent1991; Zucker, Heitzeg, & Nigg, Reference Zucker, Heitzeg and Nigg2011). In this model, factors associated with behavioral disinhibition (i.e., an inability to inhibit socially undesirable or restricted actions; Iacono, Malone, & McGue, Reference Iacono, Malone and McGue2008) serve as an early emerging core deficit underlying risk for early, quickly escalating, and prolonged substance misuse. Previous studies show that indicators of behavioral disinhibition (i.e., aggression and conduct problems) assessed in early childhood predict substance use in adolescence (e.g., Caspi, Moffitt, Newman, & Silva, Reference Caspi, Moffitt, Newman and Silva1996; Zucker, Chermack, & Curran, Reference Zucker, Chermack, Curran, Sameroff, Lewis and Miller2000) and that indicators assessed in adolescence are strongly associated with substance use and related consequences during this developmental period (e.g., Dishion & Tipsord, Reference Dishion and Tipsord2011; Hussong, Curran, & Chassin, Reference Hussong, Curran and Chassin1998; also see Zucker et al., Reference Zucker, Heitzeg and Nigg2011).
The internalizing pathway focuses on the development of substance use as a form of emotion regulation (i.e., how individuals monitor, evaluate, and modify their emotional reactions in service of meeting their goals; Thompson, Reference Thompson1994). Internalizing symptoms and emotional distress, indicators of poor emotion regulation, are weak and inconsistent predictors of substance use in youth generally but may be pernicious risk factors for long-term substance use problems among vulnerable youth (e.g., those with poor coping skills or coping motives for use) or during vulnerable periods of development (Colder, Chassin, Lee, & Villalta, Reference Colder, Chassin, Lee, Villalta and Kassel2010; Kassel et al., Reference Kassel, Hussong, Wardle, Veilleux, Heinz, Greenstein, Evatt and Scheier2010). A recent review of previous studies showed that depressive symptoms are more consistently associated with future substance use outcomes than are either anxiety or overall internalizing symptoms when controlling for often comorbid externalizing symptoms (Hussong, Ennett, Cox, & Haroon, Reference Hussong, Ennett, Cox and Haroon2017). This review also showed that depressive symptoms more consistently predict composite scores of overall substance use than single substance use indicators (for alcohol, tobacco, marijuana, or illicit drugs).
Both developmental pathways posit a dynamic framework in which core deficits underlying risk for substance use emerge over time and contribute to broader risk mechanisms that promote substance involvement (Chassin et al., Reference Chassin, Sher, Colder, Hussong and Cicchetti2016; Hussong, Rothenberg, et al., Reference Hussong, Rothenberg, Smith, Haroon, Fitzgerald and Puttlerin press; Zucker, Reference Zucker, Cicchetti and Cohen2006). For both the internalizing and the externalizing pathways, a particularly relevant set of risk mechanisms involves the peer context. Risk for substance use is strongly linked to the peer context (Ennett & Bauman, Reference Ennett and Bauman1993; Ennett et al., Reference Ennett, Bauman, Hussong, Faris, Foshee, Cai and DuRant2006, Reference Ennett, Faris, Hipp, Foshee, Bauman, Hussong and Cai2008; Osgood, Feinberg, Wallace, & Moody, Reference Osgood, Feinberg, Wallace and Moody2014; Osgood et al., Reference Osgood, Ragan, Wallace, Gest, Feinberg and Moody2013), and we posit that both distress- and deviance-related substance use may be mediated by social processes as well. The social network model provides a way of capturing the complexity of adolescents' social relationships to articulate and test these hypotheses.
The Social Network Model
Social network models are particularly relevant for studying developmental pathways to adolescent substance use. This is not only because peer behavior and relationships play such a dominant role in adjustment and health outcomes (Haas, Schaefer, & Kornienko, Reference Haas, Schaefer and Kornienko2010; Walker, Wasserman, & Wellman, Reference Walker, Wasserman and Wellman1993) but also because social network analysis directly models adolescent friendship patterns within larger social networks and identifies relational patterns that signify individual experiences of that network. In the current study, we focus specifically on the roles of social integration and social status within the peer network. We posit that risk for substance use associated with the internalizing and externalizing pathways is at least partly due to risk mechanisms associated with low social integration and status, including such posited correlates as social withdrawal, marginalization, stress, and poor social support (Berkman et al., Reference Berkman, Glass, Brissette and Seeman2000; Borgatti, Mehra, Brass, & Labiance, Reference Borgatti, Mehra, Brass and Labianca2009).
Social integration and status are two distinct yet related attributes of peer networks. Social integration reflects the extent to which adolescents are embedded in peer relationships in the network. In social network models, measures of social integration are often composed of local indices of network position involving immediate and direct friendships of adolescents (e.g., Berkman et al., Reference Berkman, Glass, Brissette and Seeman2000). Low social integration thus reflects social fragmentation and few friendships relative to immediate social contacts. Low social integration may reflect experiences of social withdrawal or marginalization that are often experienced by youth as stressful and as resulting in poor social support (Berkman et al., Reference Berkman, Glass, Brissette and Seeman2000; Borgatti et al., Reference Borgatti, Mehra, Brass and Labianca2009, regarding the exclusion mechanism; Walker et al., Reference Walker, Wasserman and Wellman1993). Social status reflects the extent to which youth experience popularity, prestige, and recognition within the larger peer network (Berkman et al., Reference Berkman, Glass, Brissette and Seeman2000; Borgatti et al., Reference Borgatti, Mehra, Brass and Labianca2009, regarding the binding mechanism). Network measures of social status often comprise both local and global ties that reflect prominence in the larger network (Berkman et al., Reference Berkman, Glass, Brissette and Seeman2000). High social status may thus reflect social power, trend setting, and the ability to reinforce norms and direct flows of information through a network (Berkman et al., Reference Berkman, Glass, Brissette and Seeman2000; Borgatti et al., Reference Borgatti, Mehra, Brass and Labianca2009). Alternatively, low social status may reflect low social power, being out of touch with peers, and global or network isolation.
Although social status and integration may often be highly correlated (particularly at the lower extreme, as social isolates are low on both; Berkman et al., Reference Berkman, Glass, Brissette and Seeman2000), this is not necessarily the case. They are distinct dimensions of social position, and it is possible to be high on one and low on the other. For example, popular adolescents' friends may not be friends with each other, a key aspect of social integration, and low-status youth may maintain high-quality friendships (Berkman et al., Reference Berkman, Glass, Brissette and Seeman2000). Yet, as indicators of social standing, the two processes may resemble each other and reflect social withdrawal, rejection, or marginalization. These social experiences may translate into psychological risk for youth in the form of social stress, reduced social support, and the experience of learned helplessness or limited power within the larger peer network. Each of these social indicators has been associated with substance use, with some suggesting that socially isolated youth (with both low integration and status) are at heightened risk for substance use and abuse (Forster, Grigsby, Bunyan, Unger, & Valente, Reference Forster, Grigsby, Bunyan, Unger and Valente2015) and others showing that high-status youth have higher risk for some forms of substance use (alcohol) but not others (cigarettes; Osgood et al., 2013, Reference Osgood, Feinberg, Wallace and Moody2014).
Experiences associated with low social integration are relevant risk mechanisms for both the internalizing and the externalizing pathway. For example, some studies suggest that youth who are depressed may withdraw from their peers (reflecting low social integration and status) and resulting loneliness and limited social support may signal risk for engaging in self-harm behaviors like substance use (Schaefer, Kornienko, & Fox, Reference Schaefer, Kornienko and Fox2011; Van Zalk, Kerr, Branje, Stattin, & Meeus, Reference Van Zalk, Kerr, Branje, Stattin and Meeus2010). Van Zalk et al. (Reference Van Zalk, Kerr, Branje, Stattin and Meeus2010) used a community network approach to show that adolescents both select friends with similar levels of depression and that they may increase each other's depressive symptoms as relationships endure, but that friendships ended more frequently for depressed youth if their friends had fewer depressive symptoms.
While low social integration and status are clear risk factors for depressive symptoms, their relationship to deviant behavior is mixed. Although some studies show little association between consistent delinquent behavior and social integration in early to middle adolescence (Rulison, Kreager, & Osgood, Reference Rulison, Kreager and Osgood2014), others show that low social integration is associated with less deviant behavior (Demuth, Reference Demuth2004). In a more nuanced view, Niño, Ignatow, and Cai (Reference Niño, Ignatow and Cai2017) suggest that low social integration is a heterogeneous category, composed of socially avoidant, actively isolated, and socially disinterested youth and that only socially disinterested youth show a robust risk for engaging in violent delinquency. Moreover, research consistently finds positive linkages between aggressive behavior and social status: popularity escalates aggression, which may in turn boosts prestige (Faris, Reference Faris2012; Faris & Felmlee, Reference Faris and Felmlee2011; Stoltz, Cillessen, van den Berg, & Gommans, Reference Stoltz, Cillessen, van den Berg and Gommans2016). More generally, research suggests that externalizing behaviors, particularly at early ages, are associated with higher social status (Franken, Harakeh, Veenstra, Vollebergh, & Dijkstra, Reference Franken, Harakeh, Veenstra, Vollebergh and Dijkstra2017; Mayeux, Sandstrom, & Cillessen, Reference Mayeux, Sandstrom and Cillessen2008). For this reason, we anticipate that low social integration as an indicator of local fragmented friendships will mediate pathways from risky symptoms (both depressive symptoms and deviant behavior) to substance use. In contrast, social status may more consistently mediate internalizing–substance use associations than externalizing–substance use associations and high social status may mediate externalizing–substance use associations among older prestige-seeking youth.
However, both the internalizing and externalizing pathways consider reciprocal processes that may fuel risk for substance use over time. Low social standing, whether through withdrawal, rejection, or marginalization, may lead to increased social stress, a lower sense of belonging, and maladaptive coping responses associated with deviant behavior or depressive symptoms. For example, both low social integration and social status have been shown to contribute to depression (Cheadle & Goosby, Reference Cheadle and Goosby2012; La Greca & Harrison, Reference La Greca and Harrison2005; La Greca & Lopez, Reference La Greca and Lopez1998; Ueno, Reference Ueno2005; Van Zalk, Van Zalk, Kerr, & Stattin, Reference Van Zalk, Van Zalk, Kerr and Stattin2011). Similarly, rejection and low social support may be related to reactive aggression and maladaptive coping that includes deviant behavior (Coie, Terry, Lenox, Lochman, & Hyman, Reference Coie, Terry, Lenox, Lochman and Hyman1995; Sijtsema, Lindenberg, & Veenstra, Reference Sijtsema, Lindenberg and Veenstra2010). For this reason, we also tested whether depressive symptoms and deviant behavior mediate the association between social position and short-term elevations in substance use across adolescents.
Pathway Moderators
We tested whether the strength of these time-varying risk mechanisms differed as a function of gender and timing (around the high school transition). Gender differences in peer clustering (high rates of homophily in peer networks based on gender; Haas et al., Reference Haas, Schaefer and Kornienko2010) and forms of symptomatology that emerge in adolescents may lead boys and girls down different risk pathways to substance use. Of note, girls begin to show higher rates of depressive symptoms and boys higher rates of deviant behavior in early to middle adolescence (Keenan & Hipwell, Reference Keenan and Hipwell2005; Zahn-Waxler, Klimes-Dougan, & Slattery, Reference Zahn-Waxler, Klimes-Dougan and Slattery2000). Falci and McNeely (Reference Falci and McNeely2009) showed that low integration was associated with elevated depressive symptoms for both boys and girls. However, high levels of integration were also risky. Girls, but not boys, who were highly integrated but in fragmented social networks showed greater risk for depression than their peers.
Given posited factors that may change social integration and status over the course of adolescence, we anticipate that these mediating roles of social standing may be particularly relevant as youth move from middle to high school, a time of social reorganization and, for some, school-related stress (Gottfredson & Hussong, Reference Gottfredson and Hussong2011; Jackson & Schulenberg, Reference Jackson and Schulenberg2013). Our previous work shows that, particularly around times of stressful transition and social reorganization (such as the transition to high school), depression-related risk for substance use may be exacerbated in youth with lower social integration (Hussong, Ennett, et al., Reference Hussong, Ennett, McNeish, Rothenberg, Cole, Gottfredson and Farisin press) and reduced social support (Gottfredson & Hussong, Reference Gottfredson and Hussong2011). Youth in this transition may be motivated to use substances in response to social isolation either to self-medicate (in the case of those with depressive symptoms) or to act out as a result of a greater inclination away from socially accepted behavior (in the case of those engaged in deviant behavior).
The Current Study
In the current study, we integrated two developmental models to examine the role of peer relationships in the externalizing and internalizing pathways to adolescent substance use. We examined two indicators of social standing (social integration and social status) as mediators of the associations between risky symptoms (depressive symptoms and deviant behavior) and substance use over Grades 6–12. With the exception of Hussong, Ennett, et al. (Reference Hussong, Ennett, McNeish, Rothenberg, Cole, Gottfredson and Farisin press), prior tests of these mechanisms relied on self-report of peer relationships, failed to control for comorbid symptoms, and did not distinguish between-person (or time-invariant) and within-person (or time-varying) effects (e.g., Hussong & Hicks, Reference Hussong and Hicks2003; Pesola et al., Reference Pesola, Shelton, Heron, Munafo, Maughan, Hickman and van den Bree2015). The latter may be particularly informative for prevention programs as time-invariant effects within a developmental framework differentiate who is at risk for escalating patterns of substance use over time whereas within-person, time-varying effects differentiate when over development a mechanism is likely to occur. In prior analyses using the same sample as the current study, Hussong, Ennett et al. (Reference Hussong, Ennett, McNeish, Rothenberg, Cole, Gottfredson and Farisin press) showed that social network indicators differentially moderated both time-invariant and time-varying effects of depressive symptoms on substance use, after controlling for deviant behavior. As expected, time-invariant effects showed that youth with elevated depressive symptoms across adolescence had escalating trajectories of substance use in high school but only if they were also lower in social status or integration. Time-varying effects showed that depressive symptoms were more strongly associated with time-specific elevations in substance use for those with higher social status or lower social integration but only in the year just after the high school transition (i.e., Grade 9).
In the current study, we extend this work to better understand whether these moderation findings reflect an underlying mediational process involving risky symptoms and peer relationships. We also expand our focus here to consider both deviant behavior and depressive symptoms as separate indicators of risky symptom-based pathways whose effects on substance use may be mediated by peer relationships. Because we posit that risk for substance use associated with socially mediated effects of risky symptoms is (a) more likely to unfold over months than over years and (b) more likely to be evident in times when youth peak in their risky symptoms (relative to their own baseline), we tested time-varying, within-person mediating mechanisms while controlling for time-invariant effects. This approach allowed us to test whether the timing of this risk was more evident around the high school transition.
We tested four specific hypotheses. We posited that time-specific elevations in depressive symptoms and deviant behavior are associated with less social integration and extremes in social status (whether high or low) in the peer network and, in turn, predict time-specific elevations in substance use, thus forming meditational pathways predicting time-specific risk for substance use (Hypothesis 1a–1d). We anticipated that social integration would similarly mediate internalizing–substance use associations and externalizing–substance use associations, but that low social status would more consistently mediate internalizing–substance use associations and high social status would mediate externalizing–substance use associations. Given gender differences in symptom patterns across adolescence (i.e., greater depression in girls and deviance in boys) as well as gender clustering within peer networks, we tested whether these mediational pathways were stronger for girls (for depressive symptoms) and for boys (for deviant behavior; Hypothesis 2a–2d). Because these pathway effects are likely transactional (an effect we could not test directly in our data), we also posited that depressive symptoms and deviant behavior would mediate the association between poor social status and integration with time-specific risk for substance use (Hypothesis 3a–3d). Finally, we anticipated that these risk pathways would be more strongly associated with substance use during the often stressful and socially disruptive transition to high school (Hypothesis 4).
Method
The Context Study was designed to support investigation of individual and contextual factors (i.e., family, peer social network, school, and neighborhood contexts) that influence the development of substance use and other problem behavior from early to late adolescence. The study used a cohort-sequential design in which three cohorts of adolescents in the 6th, 7th, and 8th grades from three complete school districts in three primarily rural North Carolina counties were enrolled in the study and surveyed in school every 6 months for five data collection waves. Adolescents in two of the three school districts were surveyed in two additional waves, 6 and 12 months later (see Table 1). The school-based design allowed measurement of peer social networks bounded by school enrollment.
Table 1. Context study design

Note: One district was not in Waves 6 and 7. Networks were bounded by grade and school for middle schools and by school for high schools. Note that for some grades, the fall and spring assessments occurred within the same grade (7th–9th).
Participants
At Wave 1, adolescents were enrolled in all 10 schools with middle grades (Grades 6, 7, 8) in the three study school districts; three alternative schools also surveyed were not included in analyses because they were inclusive of middle and high school grades with no transition possibility (see Tables 1 and 2). Beginning with Wave 2, when the first adolescents transitioned to high schools at Grade 9, the school sample added all six high schools in the districts. The school sample size fluctuates across waves depending on the inclusion of middle and high schools and due to a single school system not participating at Waves 6 and 7 (because of a change in administration). At each wave, all enrolled students at the targeted grade levels, except for those in self-contained classrooms for exceptional children and those with limited English language reading skills, were eligible for the study. The sample includes a total of 6,776 adolescents who participated in at least one of the seven waves of data collection. At Wave 1, the mean age of adolescents was 13.09 years (SD = 1.00). About half were male (52%); 53% were White, 37% Black, 4% Hispanic, and 6% other race/ethnicity. A little over 10% of adolescents lived with a single parent, and for 33% of adolescents the highest education attained by either parent was high school education or less. Demographic distributions are similar across waves. Participation rates were relatively high, with 88%, 81%, 81%, 79%, 76%, 75%, and 73% of eligible students responding to the survey at Waves 1–7, respectively. Consistent with evidence from national studies that alcohol and cigarette use tend to be higher in nonmetropolitan than metropolitan areas, lifetime rates of these substances were higher in the sample than in the Monitoring the Future study for comparable years and grades (Johnston, O'Malley, Bachman, & Schulenberg, Reference Johnston, O'Malley, Bachman and Schulenberg2006; Johnston, O'Malley, Bachman, Schulenberg, & Miech, Reference Johnston, O'Malley, Bachman, Schulenberg and Miech2014). Prevalence of marijuana use, however, was comparable to national rates (Centers for Disease Control and Prevention, 2010; Ennett et al., Reference Ennett, Faris, Hipp, Foshee, Bauman, Hussong and Cai2008; Johnston et al., Reference Johnston, O'Malley, Bachman and Schulenberg2006).
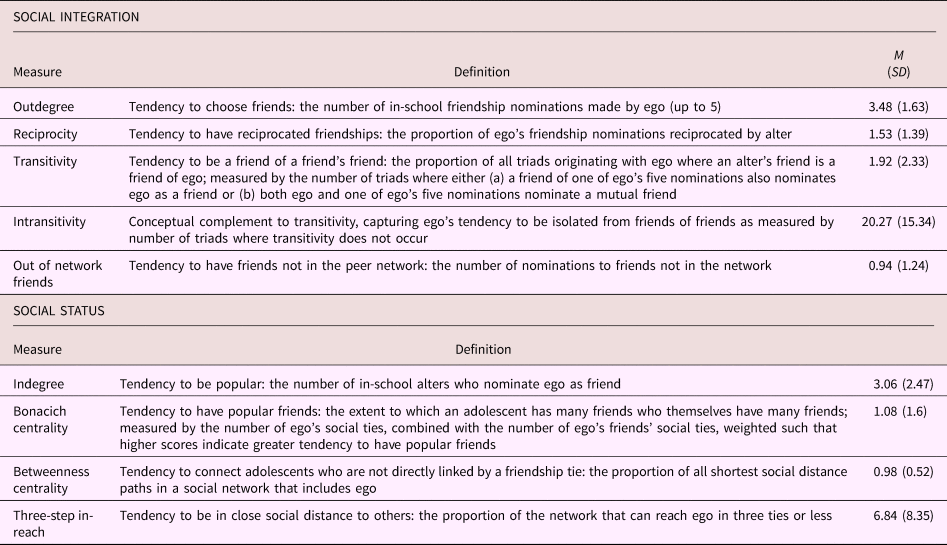
Table 2. Social network measures derived from social network analysis
Procedures
At each of the seven waves, adolescents completed in-school self-administered questionnaires taking approximately 1 hr. Trained data collectors provided instructions and monitored data collection. To minimize response bias, teachers were instructed not to answer questions about the study or walk around the classroom, but to stay in the classroom to maintain order. Adolescents were spread out from each other and instructed to use the questionnaire envelope to cover their answers. Adolescents' parents received letters that included telephone and mailed procedures for refusing study participation by their child. Written assent was obtained in school from adolescents. These procedures were approved by the University of North Carolina at Chapel Hill Institutional Review Board.
Social network analyses
Each adolescent was associated with a peer social network at each data collection wave. Schools form natural boundaries for adolescent friendships because they are the primary setting in which adolescents interact with each other (Blyth, Hill, & Thiel, Reference Blyth, Hill and Thiel1982; Brown, Reference Brown and Shirley Feldman1990; Ennett & Bauman, Reference Ennett and Bauman1996). Due to school mergers at the transition to high school, middle school networks ended and new high school networks started. Each social network was analyzed at each data collection wave to form the social network measures. (See Table 1 for a description of schools and networks.)
Social network analyses were based on friendship nominations made by adolescents within their social network (Ennett et al., Reference Ennett, Bauman, Hussong, Faris, Foshee, Cai and DuRant2006). To obtain adolescent friendship nominations, at each data collection wave, adolescents were given a student directory that included an alphabetical roster of all enrolled students and a unique four-digit peer identification number for each student. Adolescents wrote the first names of up to five of their closest friends, starting with their very best friend, in five provided spaces on the questionnaire. They then used the directory to identify any of their five friends in school and wrote in the peer identification number in the space for each friend. They were also instructed that friends not listed in the directory could be nominated; they were assigned identification number “0000.”
Measures
As in our previous work, we created scores for other measures using moderated nonlinear factor analysis (MNLFA; Bauer & Hussong, Reference Bauer and Hussong2009; Curran, Cole, Bauer, Hussong, & Gottfredson, Reference Curran, Cole, Bauer, Hussong and Gottfredson2016), a flexible extension of factor analysis that is described in further detail below. Five sets of factor scores were generated, including predictors (depressive symptoms and deviant behavior), outcomes (substance use), and mediators (social integration and status).
Depressive symptoms
Adolescents completed 3 items (i.e., hated self, was a bad person, and did everything wrong) using a 5-point response scale from a shortened version of the Short Mood and Feelings Questionnaire (Angold, Costello, Messer, & Pickles, Reference Angold, Costello, Messer and Pickles1995). Items were selected based on factor analyses conducted with a pilot sample drawn from a school district in the same region as those in the current study. Across grade Cronbach αs ranged from 0.84 to 0.93.
Deviant behavior
Adolescents completed 13 items from the Problem Behavior Frequency Scale (Farrell, Kung, White, & Valois, Reference Farrell, Kung, White and Valois2000) and 2 items assessing data violence (e.g., hitting or threatening to hit someone on a date) to assess deviant behavior. Items assessed the frequency of specific deviant behaviors (e.g., skipping school, being in a physical altercation, or cheating on a test) in the past 3 months, with five response options ranging from never to 10 times or more. Items were selected based on factor analyses conducted with a pilot sample drawn from one of the same school districts used in the larger sample analyzed in the current study. Across grade Cronbach αs ranged from 0.83 to 0.95.
Substance use
Items assessing alcohol, marijuana, and tobacco use comprised the substance use measures. Our measures of alcohol involvement included 7 items assessing consumption (i.e., quantity of use and frequency of use, having 3–4 drinks in a row, having 5 or more, getting drunk, getting drunk while alone, and being hungover in past 3 months) and 5 items assessing consequences (e.g., gotten into trouble with your parents because you had been drinking). Additional measures assessed marijuana use (1 item assessing frequency in past 3 months) and tobacco use (2 items assessing quantity and frequency of past 3 months use and 7 consequence items; e.g., found it difficult to keep from smoking in places where it is forbidden; Heatherton, Kozlowski, Frecker, & Fagerstrom, Reference Heatherton, Kozlowski, Frecker and Fagerstrom1991).
Social integration and social status
Using MNLFA, we estimated the social integration and social status factor scores from the social network variables defined in Table 2. For social integration, there were five variables: outdegree, reciprocity, intransitivity, transitivity, and out-of-network friends. For social status, there were four variables: indegree, betweenness centrality, Bonacich centrality, and three-step in-reach.
To obtain these measures, we conducted the social network analysis on present and absent friendship ties between adolescents using SAS IML modules developed by James Moody (Moody, Reference Moody2000, Reference Moody2001) and the network analysis software program UCINET (Version 6; Borgatti, Everett, & Freeman, Reference Borgatti, Everett and Freeman2002). For any pair of adolescents, a friendship tie indicates a friendship nomination of one to the other. Ties can be present or absent, and if present, they can be made only by ego (focal adolescent nominates alter as friend but not the reverse), made only by alter (alter nominates ego but not the reverse), or made by both (a reciprocated tie). If two adolescents are not directly connected by ties, they may be indirectly connected through their ties with others. Social distance is the number of ties in the shortest path between the adolescents, where a tie is counted as present if either ego nominated alter or alter nominated ego as a friend. Based on the entire set of present and absent friendship ties among the network members, social network analysis variables reflect patterns of relationships present in the network. We defined two fundamental properties that underlie our social network variables: social integration, or the degree to which individuals are embedded in school-based peer relationships, and social status, or the degree to which individuals are in prominent or advantageous social positions based on their ties to others.
Analytic approach
Our analyses followed a model-building approach. First, we used MNLFA (Curran et al., Reference Curran, Cole, Bauer, Hussong and Gottfredson2016) to create scores for key constructs. These scores served as variables in subsequent analyses that tested a series of hypotheses. We used MNLFA to generate factor score estimates for depressive symptoms, deviant behavior, substance use, social integration, and social status (Curran et al., Reference Curran, Cole, Bauer, Hussong and Gottfredson2016). MNLFA improves upon traditional confirmatory factor analysis models by integrating features of item response theory with the flexibility of factor analysis model. MNLFA scores account not only for how many items were endorsed but also for which pattern of items were endorsed and allows item loadings and item intercepts to vary as a function of student characteristics, included as covariates (referred to as differential item functioning). MNLFA also improves factor score precision by accounting for effects of student characteristics on latent variable means and variances, referred to as mean and variance impact (e.g., allowing scores to be more variable in youth from school 1 vs. 2).
As detailed in Cole et al. (Reference Cole, Hussong, Faris, Rothenberg, Gottfredson and Ennettin press), we estimated the MNLFA models using Mplus (for depressive symptoms and deviant behavior scores) or an automated R package (using an equivalent approach for substance use, social status, and social integration scores, aMNLFA; Cole, Gottfredson, Giordano, & Janssen, Reference Cole, Gottfredson, Giordano and Janssen2018), to implement the sequential model fitting approach of MNLFA (see Curran et al., Reference Curran, Cole, Bauer, Hussong and Gottfredson2016). First, a calibration sample was drawn whereby one observation was randomly selected for every participant in the sample. Descriptive statistics and item plots were evaluated and exploratory and confirmatory factor models were used to confirm unidimensionality of each construct. Second, we sequentially tested covariate effects on the latent variable means and variances and on item loadings and intercepts. Third, we estimated a simultaneous model in which nonsignificant covariate effects were trimmed using a 5% family-wise error-rate correction for multiple testing. The final scoring model was then applied to the full sample to generate factor scores.
For depressive symptoms, deviant behavior, and substance use, covariates included age, sex, race/ethnicity, parental education, school membership, study cohort, and two-way interactions among these characteristics. For social integration and social status, network size was added as a covariate. (For details regarding patterns of differential item functioning and impact results, see Cole et al., Reference Cole, Hussong, Faris, Rothenberg, Gottfredson and Ennettin press, for social integration and status and contact the first author for other constructs). As reported by Hussong, Ennett, et al. (Reference Hussong, Ennett, McNeish, Rothenberg, Cole, Gottfredson and Farisin press), final person-level deviance had a mean of 0.90 and SD of 1.0 whereas time-varying depressive symptom and substance use had means (and SD) ranging from –0.06 (0.63) to 0.05 (0.57) and –0.12 (0.71) to 2.4 (0.95), respectively. Social integration scores had a mean (and SD) ranging across schools from 0.02 (0.73) to 0.54 (0.80) and social status scores had a mean (and SD) ranging from –0.32 (0.86) to 0.26 (0.85).
Second, we estimated growth trajectories for the MNLFA-based substance use scores in the latent growth framework in Mplus 7.4 with full information maximum likelihood to address issues pertaining to missing data (Enders & Peugh, Reference Enders and Peugh2004). We fit five different plausible growth trajectories (guided by descriptive mean plots), including a linear model, a latent basis model, a quadratic function, a linear-linear piecewise model with a knot at Grade 8 Spring, and a linear-linear piecewise model with a knot at Grade 9 Fall (see Hussong, Ennett, et al., Reference Hussong, Ennett, McNeish, Rothenberg, Cole, Gottfredson and Farisin press, for more detail). Initial growth models of substance use MNLFA scores showed that a linear-linear piecewise model with a knot at Grade 8 Spring had the lowest Bayesian information criterion (65,003.98) and was well below the next best fitting model (latent basis; Bayesian information criterion = 65,040.51).
We also examined growth in each social network variable because ignoring growth in time-varying covariates can result in biased parameter estimates (Maxwell & Cole, Reference Maxwell and Cole2007). We found significant change in these variables over time (see Cole et al., Reference Cole, Hussong, Faris, Rothenberg, Gottfredson and Ennettin press; Hussong, Ennett, et al., Reference Hussong, Ennett, McNeish, Rothenberg, Cole, Gottfredson and Farisin press). There are multiple ways to account for systematic change in time-varying covariates over time but because our interest in the current analysis was to account for (rather than test hypotheses regarding) growth in time-varying covariates, we opted for a simplified approach. We first fit an unconditional latent basis growth model with each time-varying covariate as the outcome. Using a latent basis model allowed the growth process to be nonlinear. Then, in the target model used for the main analysis, we accounted for growth in the time-varying covariates by adding autoregressive paths constrained in magnitude to follow the estimated trajectory from the separate latent basis model. This allowed time-varying covariate growth to be accounted for with the most minimally invasive method while also estimating as few parameters as possible.
We then tested whether time-varying measures of social integration and status mediated associations between time-specific elevations in risky symptoms and time-specific elevations in substance use (Hypothesis 1) in four models that examined this mediating pathway for depressive symptoms and social status (Hypothesis 1a), depressive symptoms and social integration (Hypothesis 1b), deviant behavior and social status (Hypothesis 1c), and deviant behavior and social integration (Hypothesis 1d). In all models, race/ethnicity, gender, parental education, and school membership were included as time-invariant covariates. In addition, person-level means of deviant behavior, depressive symptoms, social status, and social integration were included, so that each time-varying effect may be interpreted as an individual's time-specific deviation from his or her overall mean (Curran, Howard, Bainter, Lane, & McGinley, Reference Curran, Howard, Bainter, Lane and McGinley2014; see Figure 1). All models were estimated in Mplus 7.4 with full information maximum likelihood. This method, which has shown superior performance to pairwise and listwise deletion (Enders & Bandalos, Reference Enders and Bandalos2001), assumes that data are missing at random (a reasonable assumption here) but allows all cases to be included, even if they are missing some data on outcomes. Data were clustered within six different schools. Because of the small sample of schools, the incidental nature of the clustering, and the fact that substantive questions pertained to person-level information rather than school-level information, we modeled the school-level data with fixed effects to avoid complications of random effect estimation with few clusters and to prevent possible endogeneity at the school level caused by potentially omitted variables at a level of minimal substantive interest (McNeish & Wentzel, Reference McNeish and Wentzel2017).

Figure 1. Summary of full structural equation models including time-varying mediation effects in Stage 3. PL-Dep, PL-Dev, and PL-SocInt stand for person-level means of depression, deviance, and social integration, respectively. LowEd, HighEd, SubUse, SocInt, and Dep stand for low parental education, high parental education, substance use, social integration, and depression, respectively. Finally, note that whereas time-varying social integration and depressive symptoms are used in our hypotheses, this general model was fit four times in total, with corresponding models for depressive symptoms and social integration (Hypotheses 1b–3b), deviance and social status (Hypotheses 1c–3c), and deviance and social integration (Hypotheses 1d–3d).
To test indirect effects, we employed a Monte Carlo resampling method with 100,000 replications (MacKinnon, Lockwood, & Williams, Reference MacKinnon, Lockwood and Williams2004; Williams & MacKinnon, Reference Williams and MacKinnon2008). This method has been shown to be more powerful than the traditional delta method (aka the Sobel test) in a study by Fritz and MacKinnon (Reference Fritz and MacKinnon2007). The resampling method is similar to bootstrapping except that the model-implied mean vector and covariance matrix from a single fit are resampled instead of the data. This is advantageous in the current analysis because the model only needs to be fit once rather than thousands of times as in bootstrapping (Preacher & Selig, Reference Preacher and Selig2012). With models of the complexity we fit in this study, computational times would be excessive with bootstrapping.
We next tested whether mediational pathways tested in Hypotheses 1a–1d varied by gender (Hypothesis 2) using a multiple-groups structural equation modeling approach. We used likelihood ratio tests to compare a fully unconstrained model (in which all parameters varied between males and females) and a constrained model in which the time-varying portion of the model (i.e., effects between symptoms, social network indicators, and substance use) were held equal across gender. If a likelihood ratio test showed a significant decrement in fit between the two models, we conducted Wald tests to determine which of the mediational pathways differed by gender in a series of models that constrained each pathway in time to be equal across gender one at a time.
Finally, we tested identical mediation models to those examined for Hypotheses 1a–1d but in which risky symptoms served as mediators of the association between time-varying social network indicators and substance use (Hypotheses 3a–3d). Because we estimated all mediational pathways across assessments from the spring of 6th grade through fall of 12th grade, we examined whether any of our mediational pathways was more evident around the high school transition (Hypothesis 4).
Results
Hypothesis 1: Social network indices mediate time-varying associations between risky symptoms and substance use
Depressive symptoms
The model including social status explained between 35.2% and 88.8% of the variance in substance use over time; the model including social integration explained between 35.4% and 88.4% of the variance in substance use over time. Variance explained increased across grade (in this and all models). Results of mediation analyses revealed significant indirect effects in which social status mediated the association between depressive symptoms and substance use at 2 of the 11 observed time points (Hypothesis 1a; see Figure 2). This mediation occurred just following the high school transition, in Grade 9 Fall (β = .001, 95% confidence interval; CI [.000, .003]) and Grade 9 Spring (β = .002, 95% CI [.000, .006]). Both indirect effects were positive with negative direct effects meaning that relatively higher individual depressive symptoms predicted lower social status, which in turn predicted higher substance use such that time-specific elevations in depressive symptoms increased substance use through lower social status.

Figure 2. Summary of all indirect effects for Hypotheses 1 and 3. Time-varying mediation pathways for all effects in models for Hypotheses 1a–d and 3a–d. Following standard notation, the path from the predictor to the mediator is labeled a; the path from the mediator to the outcome is denoted b; and the direct effect from the predictor to the outcome is denoted c’. For each of the hypotheses, an arrow indicates a significant indirect effect, given by a value of a*b that is significantly different from zero, at the corresponding time.
When social integration was treated as a mediator of the relationship between depressive symptoms and substance use, an indirect effect was found in 1 of the 11 time points (Hypothesis 1b). Social integration mediated the association between depressive symptoms and substance use in Grade 9 Spring (β = .002, 95% CI [.000, .003]). Similar to social status, the indirect effect was positive with negative direct effects (β = –.060, 95% CI [–.109, –.011] for the effect of depressive symptoms on integration and β = –.032, 95% CI [–.065, –.001] for the effect of integration on substance use), showing that time-specific increases in depressive symptoms increased substance use through lower social integration. (Note that zero is scarcely outside the 95% CI, so the hypothetical p value for these effects would be quite close to .05. The use of the resampling precludes computation of p values because the sampling distribution is empirical and does not follow a known distribution whose probabilities are easily calculable; DiCiccio & Efron, Reference DiCiccio and Efron1996.)
Deviant behavior
The model including social status explained between 39.6% and 90.2% of the variance in substance use over time; the model including social integration explained between 39.6% and 89.7% of the variance in substance use over time. When social status was used as a mediator of the relationship between deviant behavior and substance use (Hypothesis 1c), deviance exerted a positive indirect effect on substance use at Grade 7 Fall (β = .001, 95% CI [.000, .004]) and Grade 8 Spring (β = .001, 95% CI [.000, .002]). At both time points, deviant behavior was associated with increased social status, which in turn predicted increased substance use. In Grade 9 Fall, deviance exerted a negative indirect effect on substance use (β = –.002, 95% CI [–.005, –.001]), such that deviance was associated with increased social status but increased social status was associated with lower substance use.
Similar patterns emerged when social integration was used as a mediator of the relationship between deviant behavior and substance use (Hypothesis 1d). As with social status, deviance exerted a positive indirect effect through social integration at Grade 7 Fall (β = .001, 95% CI [.000, .003]) and Grade 8 Spring (β = .001, 95% CI [.000, .003]). At both time points, increased deviance predicted increased social integration, which predicted increased substance use. However, deviant behavior also showed a positive indirect effect at Grade 9 Spring (β = .001, 95% CI [.000, .004]); here, the direct effects were negative, with increases in deviance leading to lower social integration, which led to increased substance use.
Hypothesis 2: Gender differences in mediational pathways
Depressive symptoms
Providing an omnibus test of gender differences in the mediational pathway involving depressive symptoms, social status, and substance use (Hypothesis 2a), the unconstrained model provided a significant improvement in fit over the constrained model, χ2 (53) = 103.29, p < .001, indicating the presence of gender differences in these time-varying mediational pathways. However, tests of equality constraints across gender for individual indirect effects at each time point were null, suggesting no meaningful gender differences at any one time point. Similar results were found when investigating gender differences in the path from depressive symptoms through social integration to substance use (Hypothesis 2b). Here, too, there was a significant decrease in fit from the unconstrained model to the constrained model, χ2 (53) = 114.41, p < .001, but no differences in indirect effects across boys and girls.
Deviant behavior
As with depressive symptoms, we tested the hypotheses of gender differences in the time-varying relationships between deviance, social network variables, and substance use. When social status mediated the relationship between deviant behavior and substance use (Hypothesis 2c), there was a significant difference in fit between a model that constrained these parameters to equality across male and female subjects and one that did not, χ2 (53) = 90.80, p < .001. However, as with depressive symptoms, no specific indirect effects were found to differ across boys and girls. Parallel findings emerged in the model containing social integration as a mediator (Hypothesis 2d), with significant between-group differences, χ2 (53) = 108.52, p < .001, but no specific indirect effects differing between boys and girls.
Table 3. Effects of depressive symptoms and deviant behavior on substance use through social integration and status

Note: Bold estimates and standard errors are those that were significantly different from zero, p < .05. Note that, whereas the significance level of direct effects was determined using a Wald z test, the significance of indirect effects was determined using resampling as described by Preacher and Selig (Reference Preacher and Selig2012).
Table 4. Effects of social integration and status on substance use through depressive symptoms and deviant behavior

Note: Bold estimates and standard errors are those that were significantly different from zero, p < .05. Note that, whereas the significance level of direct effects was determined using a Wald z. test, the significance of indirect effects was determined using resampling as described by Preacher and Selig (Reference Preacher and Selig2012).
Hypothesis 3: Risky symptoms mediate time-varying associations between social network indices and substance use
Depressive symptoms
The model including social status explained between 35.4% and 88.9% of the variance in substance use over time; the model including social integration explained between 35.5% and 88.5% of the variance in substance use over time. We next tested whether depressive symptoms mediated the relationship between social status and substance use (Hypothesis 3a). Social status exerted a negative indirect effect on substance use by decreasing depressive symptoms, which in turn predicted increased substance use, at Grade 7 Spring (β = –.005, 95% CI [–.010, .000]), Grade 9 Fall (β = –.002, 95% CI [–.005, .000]), and Grade 9 Spring (β = –.004, 95% CI [–.010, .000]). At Grade 10 Spring, social status exerted a positive indirect effect on substance use (β = .004, 95% CI [.000, .011]) by increasing depressive symptoms, which in turn increased substance use.
Social integration exerted a negative indirect effect on substance use as mediated through depressive symptoms at Grade 7 Spring (β = –.004, 95% CI [–.008, .000]) and Grade 9 Spring (β = –.005, 95% CI [–.010, .000]). Specifically, greater social integration was associated with lower depressive symptoms, but the effect of depressive symptoms on substance use was positive.
Deviant behavior
The model including social status explained between 39.6% and 90.0% of the variance in substance use over time; the model including social integration explained between 39.6% and 89.8% of the variance in substance use over time. Deviance was shown to mediate the relationship between social status and substance use at four time points (Hypothesis 3c). Specifically, social status was associated with decreased deviant behavior, which in turn predicted increased substance use at Grade 7 Fall (β = .027, 95% CI [.006, .051]), Grade 8 Fall (β = .019, 95% CI [.003, .037]), and Grade 9 Fall (β = .020, 95% CI [.007, .035]). However, in Grade 12 Fall, this effect changed directions (β = –.050, 95% CI [–.093, –.014]), with a negative direct effect from social status to deviance and a positive direct effect from deviance to substance use.
Finally, deviant behavior mediated the relationship between social integration and substance use at three time points (Hypothesis 3d). This indirect effect was positive, with positive direct effects, at Grade 7 Fall (β = .031, 95% CI [.008, .058]), Grade 8 Spring (β = .007, 95% CI [.001, .016]), and Grade 9 Fall (β = .016, 95% CI [.000, .033]).
Discussion
In the current study, we tested hypotheses based on the integration of models regarding internalizing and externalizing pathways (Chassin et al., Reference Chassin, Sher, Colder, Hussong and Cicchetti2016; Hussong et al., Reference Hussong, Jones, Stein, Baucom and Boeding2011; Hussong, Rothenberg, et al., Reference Hussong, Rothenberg, Smith, Haroon, Fitzgerald and Puttlerin press; Zucker, Reference Zucker, Cicchetti and Cohen2006) for youth substance use with models regarding social standing of youth drawn from social network theory (Berkman et al., Reference Berkman, Glass, Brissette and Seeman2000). We tested potential reciprocal effects in these pathways, including whether time-specific elevations in social network indicators (i.e., social standing and integration) mediated associations between risky symptoms (i.e., depressive symptoms and deviant behavior) and substance use and whether risky symptoms mediated the association between social network indicators and substance use. Results indicate that the pattern of effects underlying these pathways differs prior to and just following the transition to high school and that models accounted for moderate to large proportions of variance in substance use outcomes. These effects were found after controlling for the time-invariant effects of deviant behavior and depressive symptoms on substance use outcomes and did not differ by gender. Two primary risk mechanisms linking risky symptoms, social network indicators, and substance use emerged from these findings with unique patterns associated with pathways involving deviant behavior and depressive symptoms.
In middle school, deviant behavior predicted high social status and high social integration, markers of high visibility and embeddedness in the school network consistent with some definitions of popularity (Berkman et al., Reference Berkman, Glass, Brissette and Seeman2000). This association was reciprocal in our mediational models (for fall of seventh grade) such that deviant behavior beget popularity and vice versa, with both pathways increasing risk for substance use. After the high school transition, popularity (high social status and integration) still predicted higher deviant behavior and greater risk for substance use, but the role of social network indicators as mediating the association between deviant behavior and substance use changed. During ninth grade, deviance behavior predicted greater social status but lower social integration; in turn, lower social status and social integration (consistent with the experience of social isolation) predicted greater risk for substance use. In other words, deviant behavior had dual effects in the year after the high school transition: it predicted higher social status, which was associated with lower risk for substance use, but it also predicted lower social integration, which was associated with amplified risk for substance use. Based on our findings, it is not clear whether these dual effects are taking place for different youth or are competing mechanisms that jointly influence risk for substance use within any given youth. It is clear, however, that the potential mechanisms that may account for the interplay of deviant behavior and social interactions in relation to substance use begin to shift after the high school transition.
In middle school, deviant behavior–substance use relations were associated with peaks in social status and integration. The use of substances early in adolescence, when use is less prevalent, may reflect a social mimicry behavior (Moffitt, Reference Moffitt1993) and convey a sense of pseudomaturity (Newcomb, Reference Newcomb1996) signaling that an adolescent has achieved adult status and is able to engage in adult behaviors, involving both deviant behaviors and substance use. These youth may be leaders among young adolescents seeking maturity. Even in high school, having high status and integration in the high school peer network continued to increase risk for substance use via engagement in deviant behavior. However, this was only part of the picture as the main effects of low social status and integration were also associated with greater risk for substance use, consistent with a social isolation mechanism.
This high school transition was also critical in findings pertaining to the internalizing pathway to substance use. In middle school, there was no support for a depression pathway to substance use as mediated by social network indicators. However, low social status and social integration indicative of social isolation each increased risk for depressive symptoms and in turn substance use (in the spring of seventh grade). In ninth grade, this pattern continued, but a reciprocal effect was also evident in which depressive symptoms predicted greater social isolation (i.e., lower social integration and status) and in turn greater substance use. The potentially greater stress that youth anticipate (Stein & Hussong, Reference Stein and Hussong2007) and experience after this transition (Gottfredson & Hussong, Reference Gottfredson and Hussong2011; Jackson & Schulenberg, Reference Jackson and Schulenberg2013) may motivate them to seek new ways of coping. This may include the use of substances, but it may also include finding new social relationships that fit with an emerging sense of self during a time of social transition. In addition, youth may have more access to substances as a way of coping after they transition to high school. For most youth in this study, the transition to high school meant integrating into a social network that included students from other feeder schools, resulting in larger classes and potential shifts in social hierarchies. As youth settle into these hierarchies outside of the high school transition, depressive symptoms may operate less through moving youth around within the social network (by lowering social status and integration) and once again more directly predict substance use by means of self-medication. Thus, the mechanisms by which depressive symptoms and substance use are associated may shift over development.
In general, findings regarding social status and integration were largely consistent with one another as would be anticipated by mechanisms such as befriended popularity (i.e., involving high status and high integration) and isolation (i.e., involving low status and low integration), although this pattern was disrupted for mediational pathways associated with deviance–substance use associations in the year after the high school transition. In addition, isolated effects evident later in high school showed that (a) greater social status predicted greater depression and, in turn, greater substance use in 10th grade and (b) greater social status predicted lower deviant behavior and, in turn, lower substance use in 12th grade. These findings may suggest that the role of social status in these risk pathways for substance use continues to change across high school and, perhaps, to change in ways that do not parallel effects for social integration. Similar findings regarding the importance of popularity in guiding adolescent behaviors (Lansu & Cillessen, Reference Lansu and Cillessen2015; Logis, Rodkin, Gest, & Ahn, Reference Logis, Rodkin, Gest and Ahn2013) and in the importance of timing of peer experiences on social and mental health outcomes (Dijkstra, Cillessen, & Borch, Reference Dijkstra, Cillessen and Borch2013; Prinstein & Giletta, Reference Prinstein, Giletta and Cicchetti2016) have been reported in the sociometric literature. Given that school-based peer networks become a smaller part of an adolescent's social network in high school (with school dropout or increased out of school activities associated with sports and work), the meaning of social status within this network may change with development as well as with local school-based norms regarding what is valued as a sign of status.
Both risky symptoms and social network indicators were independently associated with time-specific increases in substance use at time points outside of the high school transition. Deviant behavior and depressive symptoms were consistently positively associated with risk for substance use; social integration and status showed more varied effects. However, mediational pathways were largely clustered around the high school transition. These findings suggest that at the point of the high school transition, these risk processes for substance use may intersect, creating unique risk processes at a time of both increased stress and greater social reorganization in the lives of youth.
The study has several strengths that include the prospective design, focus on social network constructs rather than individual measures, and integration of two theoretical models to better understand adolescent substance use. However, limitations are also present. These include shortened measures for depressive symptoms (that may have focused more on low self-esteem and self-image than on the broader construct of depression), a small school-level sample size (that did not permit us to examine school differences), use of a school-based peer network (that omits potential relationships outside of school), and reliance on self-report measures for depressive symptoms, deviant behavior, and substance use. We were also unable to examine the joint effects of social integration and status, which would more directly map onto the construct of social isolation. Nonetheless, the largely consistent findings of the study are compelling. Future directions for research include consideration of additional factors within the individual (e.g., motivations for use) and family context that might further identify persons and mechanisms related to risk for depression-motivated substance use, particularly around the high school transition. In addition, future work is needed to consider the impact of larger peer networks, beyond that within the school, on these dynamic relationships among peers, depressive symptoms, and substance involvement. In sum, the high school transition appears to be a particularly risky time for substance use as related to the interplay of increases in depressive symptoms and deviant behavior on the one hand and decreases in social status and integration on the other. These findings suggest important targets (the interplay of social factors related to risky depressive symptoms and deviant behavior) and timing (around the high school transition) for refining prevention programs targeting elevations in substance use for adolescents.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S095457941900049X.
Funding Statement
Research reported in this publication was supported by National Institute on Drug Abuse of the National Institutes of Health Grants R01 DA037215 (to A.M.H.) and R01 DA13459 (to S.T.E.), National Research Service Award F31 DA040334 (to V.T.C.), Mentored Research Scientist Award K01 DA035135 (to N.C.G.), and Predoctoral Fellowship T32-HD07376 through the Center of Developmental Science, University of North Carolina at Chapel Hill (to W.A.R.). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.








