



For centuries, philosophers, theorists, and researchers have proposed a strong link between language and thought (Corballis, Reference Corballis2016; Piaget, Reference Piaget, Gabain and Gabain1959; Plato & McDowell, Reference Plato and McDowell1973; Vygotsky, Reference Vygotsky1934/1962). As beings capable of engaging in a thinking process, whether reflecting, remembering, or problem solving, we benefit from an ability to hold representations in mind in the form of words. The private representation and use of language in its overt (i.e., out-loud), covert (i.e., muttering and whispering), and internalized (i.e., silent “inner speech”) forms has attracted many labels such as private speech, inner speech, self-directed speech (SDS), self-regulatory speech, and self-talk. Private speech is extensively used to describe overt and covert forms, whereas inner speech typically refers to internalized verbal thought. For the purpose of this review, self-directed speech provides an inclusive term to capture both private and inner speech forms (Copeland, Reference Copeland1979; Kuvalja, Verma, & Whitebread, Reference Kuvalja, Verma and Whitebread2014; Lidstone, Meins, & Fernyhough, Reference Lidstone, Meins and Fernyhough2010; Reference Lidstone, Meins and Fernyhough2012).
As a metacognitive tool to monitor and control thinking and behavior, SDS holds an important self-regulatory function from early childhood. Following a curvilinear developmental trajectory, overt private speech emerges in the toddler years, increases in promininence during early primary school, and gradually becomes more covert as children progress toward internalized verbal thought (Manfra & Winsler, Reference Manfra and Winsler2006; Winsler, Diaz, Atencio, McCarthy, & Chabay, Reference Winsler, Diaz, Atencio, McCarthy and Chabay2000; Winsler & Naglieri, Reference Winsler and Naglieri2003). Typically developing preschoolers use increasingly goal-directed private speech (Winsler, Carlton, & Barry, Reference Winsler, Carlton and Barry2000) and display performance benefits when instructed to use overt private speech within tasks (Winsler, Manfra, & Diaz, Reference Winsler, Manfra and Diaz2007). Although overt private speech use positively influences performance (Müller, Zelazo, Hood, Leone, & Rohrer, Reference Müller, Zelazo, Hood, Leone and Rohrer2004; Winsler & Naglieri, Reference Winsler and Naglieri2003) and self-control (Manfra, Davis, Ducenne, & Winsler, Reference Manfra, Davis, Ducenne and Winsler2014) in early childhood, an earlier developmental progression toward internalized verbal thought has been associated with increased task success (Winsler et al., Reference Winsler, Manfra and Diaz2007). Furthermore, a conscious awareness of private speech, although not a precondition for verbal strategy use, was positively related to both its use and self-regulatory effectiveness (Winsler & Naglieri, Reference Winsler and Naglieri2003). Thus, an awareness of private speech and its progression toward inner speech present critical developmental markers.
Notwithstanding clear developmental trends relating to SDS form, content and self-awareness, the dynamic interaction between SDS and self-regulatory efficacy is complex and likely influenced by task demand, social context, and individual differences (Diaz & Berk, Reference Diaz and Berk1995). The progression from private to inner speech may synonymously signal a progression in deployed cognitive effort to task-based automaticity, a phenomenon persisting into adulthood (Diaz & Berk, Reference Diaz and Berk1995; Duncan & Cheyne, Reference Duncan and Cheyne2002; Kray, Eber, & Karbach, Reference Kray, Eber and Karbach2008). Fernyhough and Fradley (Reference Fernyhough and Fradley2005) observed a dynamic interaction between SDS use and task difficulty in typically developing 5-year-old children completing the Tower of London problem-solving task. Overt private speech was most obvious within trials of medium difficulty and less obvious during trials that were either too easy or too difficult. Additionally, the efficacy of overt private speech was most obvious during medium difficulty trials. In contrast, success on simple trials was associated with silence, and failure on difficult trials was associated with overt private speech. Equally, Diaz and Berk (Reference Diaz and Berk1995) proposed individual differences in the efficacy of SDS and alluded to qualitative differences in the self-regulatory content of SDS in children with learning or behavior difficulties.
Paralleling the research on other metacognitive behaviors, recent findings suggest that SDS may emerge as a component of developmentally significant interfunctional relations (Fernyhough, Reference Fernyhough, Sokol, Müller, Carpendale, Young and Iarocci2010) between language (Manfra & Winsler, Reference Manfra and Winsler2006), executive functioning (Müller, Jacques, Brocki, & Zelazo, Reference Müller, Jacques, Brocki, Zelazo, Winsler, Fernyhough and Montero2009), and social understanding (Fernyhough & Meins, Reference Fernyhough, Meins, Winsler, Fernyhough and Montero2009; Manfra & Winsler, Reference Manfra and Winsler2006). Not surprisingly, there is growing evidence to suggest atypical SDS development in children with DLD, ASD, and ADHD; neurodevelopmental disorders underpinned by varying degrees of deficit in executive function, language, and social understanding (Barkley, Reference Barkley2011; Farrant, Fletcher, & Maybery, Reference Farrant, Fletcher and Maybery2006; Finneran, Francis, & Leonard, Reference Finneran, Francis and Leonard2009; Geurts & Embrechts, Reference Geurts and Embrechts2008; Hill, Reference Hill2004; Wehmeier, Schacht, & Barkley, Reference Wehmeier, Schacht and Barkley2010). Atypical SDS represents a common metacognitive control deficit underpinning self-regulatory challenges characteristic of these diagnostic groups. However, despite the identified role of SDS in self-regulation, there remains a lack of clarity concerning the nature, extent, and implications of SDS interruption in neurodevelopmental disorders.
To date, literature reviews on private speech (Winsler, Reference Winsler, Winsler, Fernyhough and Montero2009) and inner speech (Alderson-Day & Fernyhough, Reference Alderson-Day and Fernyhough2015) broadly discuss this topic across many branches of the psychological sciences, yet there has been limited focus on the self-regulatory implications of SDS interruption in neurodevelopmental disorders. Furthermore, a surge in research on SDS in neurodevelopmental disorders over the past decade provides opportunity to better understand mechanisms underpinning self-regulatory impairments in this group of children. This systematic review will narrow the lens and spotlight atypical development of SDS in neurodevelopmental disorders, identify the impact on self-regulation of thinking and behavior, and emphasize important future directions to explicate the mechanistic relationship between SDS and self-regulation. It is proposed that findings from this review will provide a valid precursor to future research in this field.
Theoretical background
Conceptually, the developmental research on SDS is underpinned by two major theoretical traditions: sociocultural and information processing theories. From a sociocultural tradition, Vygotsky (Reference Vygotsky1934/1962) and his colleague Luria (Reference Luria1959) posit SDS as a mediator of higher order cognitive functions, the emergence of which signifies a critical point in the shift from externally regulated, to self-regulated behavior. From this perspective, SDS exists as a product of socially mediated ontogenesis. The regulatory language of significant others used to guide young children's actions and behavior becomes represented by the self as overt private speech and then gradually internalized as verbally mediated thought used to self-regulate aspects of cognition and behavior (Fernyhough, Reference Fernyhough, Sokol, Müller, Carpendale, Young and Iarocci2010; Winsler, Reference Winsler, Winsler, Fernyhough and Montero2009). This process reflects the development of what Vygotsky and his colleague Luria coin a “functional system” in which functional relations develop between language and other higher order cognitive functions such as executive functioning and social understanding (Fernyhough, Reference Fernyhough, Sokol, Müller, Carpendale, Young and Iarocci2010).
In accordance with this sociocultural position, interference in the ontogenesis and self-regulatory effectiveness of SDS is implicated by cognitive and socio-affective deficits inherent in the outlined neurodevelopmental disorders. Disturbance in language development poses a cognitive barrier to the emergence and use of linguistically mediated SDS. Developmental language deficits represent a fundamental feature of DLD, whereas children with ASD and ADHD exhibit an increased likelihood of difficulty across the domains of receptive language, expressive language, and pragmatic communication (Geurts & Embrechts, Reference Geurts and Embrechts2008; Walsh, Scullion, Burns, Macevilly, & Brosnan, Reference Walsh, Scullion, Burns, MacEvilly and Brosnan2014). Lidstone et al. (Reference Lidstone, Meins and Fernyhough2012) underscore a twofold barrier to SDS development in children with language difficulties: expressive language weakness may impact on the “utility of speech in cognition” while receptive language weakness may limit comprehension of linguistically mediated caregiver scaffolding believed to support the shift from other- to self-regulation.
Furthermore, the Vygotskian perspective on SDS as a socially mediated phenomenon implies a relational barrier to its emergence and use in children with ASD and ADHD, stemming from impoverished social interactions characteristic of these disorders (Lidstone, Fernyhough, Meins, & Whitehouse, Reference Lidstone, Fernyhough, Meins and Whitehouse2009; Wehmeier, Schacht, & Barkley, Reference Wehmeier, Schacht and Barkley2010). Indeed, the quality of parent-child interactions for individuals with ASD and ADHD has been shown to suffer (Beurkens, Hobson, & Hobson, Reference Beurkens, Hobson and Hobson2013; Danforth, Connor, & Doerfler, Reference Danforth, Connor and Doerfler2016; La Rocque & Winsler, Reference La Rocque, Winsler, Finestone and Lidstone2011). The importance of quality parent-child interactions in supporting regulatory private speech use is evidenced in research with typically developing preschoolers. Effective adult scaffolding increases child use of task-directed private speech and subsequent task performance (Winsler, Diaz, & Montero, Reference Winsler, Diaz and Montero1997). Hence, a breakdown in responsive parent-child interactions in children with ASD and ADHD could potentially interfere with the development and self-regulatory effectiveness of SDS (Barkley, Reference Barkley1997; Winsler, Reference Winsler1998).
In the advent of information processing theory, researchers have also come to consider SDS in the context of verbally mediated strategy use that supports performance in memory and problem-solving tasks. The influential working memory model as conceptualized by Baddeley and Hitch (Reference Baddeley, Hitch and Bower1974) positions SDS as functional within its component phonological loop. This multicomponent model consists of a central executive whose proposed role is to concurrently store, manipulate, and coordinate information directed from two slave systems: the visuospatial sketchpad and the phonological loop (Baddeley, Reference Baddeley1992; Baddeley & Hitch, Reference Baddeley, Hitch and Bower1974). The phonological loop comprises two components, a passive phonological store, which holds information for up to one to two seconds, and an active articulatory control process. Baddeley (Reference Baddeley1992) describes the articulatory control process as akin to inner speech. The role of this control process is the subvocal rehearsal of verbal material to prevent decay, and the translation of visual information into verbal representations that, too, can be rehearsed. While offering useful methodological paradigms for the investigation of inner speech, the working memory model alone provides a narrow explanation of SDS as verbal strategy use, largely independent of wider self-regulatory functions (Williams, Happé, & Jarrold, Reference Williams, Happé and Jarrold2008).
Developmental private speech markers
The array of research questions and methodological paradigms within the literature under review has largely been driven by the theoretical standpoint of the researchers. Albeit using different methods, researchers tend to profile variables such as SDS form and content. These measures of SDS provide markers against which to compare typical and atypical developmental trajectories. In addition, the interaction between SDS use and task performance provides insight into its self-regulatory function.
The form of SDS is often characterized on a maturational continuum from overt speech (i.e., out-loud) through covert speech (i.e., lip movement, mumbling, whispering) to internalized speech (i.e., inner speech). While overt and covert forms of private speech are identified and profiled from observational paradigms, internalized speech poses a challenge for measurement. Rather the presence and extent to which inner speech is used, is typically explored via experimental protocols based on a working memory conceptualization of inner speech. One classic design requires participants to engage in arithmetic task switching (i.e., alternating between addition and subtraction) with and without articulatory suppression, an experimental condition that requires consistent verbalization of material unrelated to the primary task (e.g., days of the week repeated over and over). This manipulation is believed to exhaust the capacity of the phonological loop and, consequently, impairs a participant's ability to use inner speech for subvocal verbal rehearsal. Indeed, for those using inner speech, articulatory suppression leads to latency or performance costs on the primary task (Baddeley, Reference Baddeley1992).
The content of SDS typically refers to the meaning of the utterance. Coded content categories may be defined by the content elicited during a task or predefined semantic (e.g., task relevant, task irrelevant), syntactic (e.g., questions, exclamations), or functional codes (e.g., self-regulatory, imaginary). In typical development, the content of SDS becomes increasingly strategic in the later preschool years (Winsler et al., Reference Winsler, Diaz, Atencio, McCarthy and Chabay2000) and markers associated with developmental maturity include task relevant and regulatory content. SDS content has typically been considered in the broader context of whether it is task relevant or irrelevant following Berk's (Reference Berk1986) three-level categories that co-classify SDS form and content. Within this coding scheme, SDS is categorized as overt task irrelevant private speech, overt task relevant private speech, and inaudible muttering (i.e., covert speech). However, SDS has also been coded according to semantic or syntactic content (Copeland, Reference Copeland1979; Winsler, Reference Winsler1998) or the pre-supposed function it is believed to represent within a specific task (Furrow, Reference Furrow1984).
Method
The systematic review approach provides a robust review methodology that aims to synthesize key findings, uncover patterns, and identify gaps that exist in research on this area. In our synthesis of the research, we highlight differential ontogenesis of private speech form and content in neurodevelopmental disorders, and interpret the self-regulatory implications of atypical SDS development for children with DLD, ASD, and ADHD. Emerging from this analysis, important directions for future research are highlighted.
Selection criteria
The review sought to include peer-reviewed research investigating SDS in children with DLD, ASD, and ADHD diagnoses associated with developmental vulnerability in areas of language, social-emotional functioning, and executive functioning. Research written in English and published from 1962 to August 2017 was considered. Childhood was defined by ages 2 to 12 years—2 years marking the developmental period that a young child's expressive language output typically shifts from single-word to phrase-level utterances (Luinge, Post, Wit, & Goorhuis-Brouwer, Reference Luinge, Post, Wit and Goorhuis-Brouwer2006), and 12 years marking a point typically accepted as pre-teen (McDevitt, Reference McDevitt2013). Accordingly, research with a participant mean age between 2 and 12 years met the criteria for consideration. Only research investigating children with DLD, ASD, and ADHD, as determined in accordance with criteria from the Diagnostic Statistical Manual (DSM) at the time of investigation, was included. Adherence to diagnostic standards ensures reliability in the definition of developmental vulnerability. The English translation of Lev Vygotsky's book titled, Thought and Language, positions 1962 as a historically significant starting point in that his conceptualization of SDS as a self-regulatory tool sparked an emergence of research into this phenomenon.
Literature search
We performed an extensive literature search of multiple electronic databases and communicated with key experts on the topics of private- and inner-speech. An electronic search strategy was designed consisting of predefined search terms and use of search techniques such as Boolean operators, truncation, and parentheses to support database search sensitivity (see Supplementary Material). Relevant databases identified by researchers included PsychInfo, PubMed, ERIC, CINAHL, SpeechBITE, and OT Seeker. The electronic literature search retrieved a total of 643 records and one further record was obtained via communication with experts. The titles and abstracts of all identified records were collated using EndNote™ reference management software. Following the omission of duplicate records, the titles and abstracts of 481 prospective records were screened for relevance and acceptability using the predefined selection criteria. A total of 444 records were excluded following this screening process. Finally, the full-texts of 37 remaining records were retrieved and assessed for inclusion in the review. Primary reasons for exclusion of records at this point included a lack of clarity regarding adherence to relevant DSM criteria at the time of publication, failure to meet criteria as a peer-reviewed record, and discussion of SDS as an intervention component rather than the primary focus of investigation. Consequently, a total of 19 records were considered in the qualitative synthesis of data (see Figure 1).
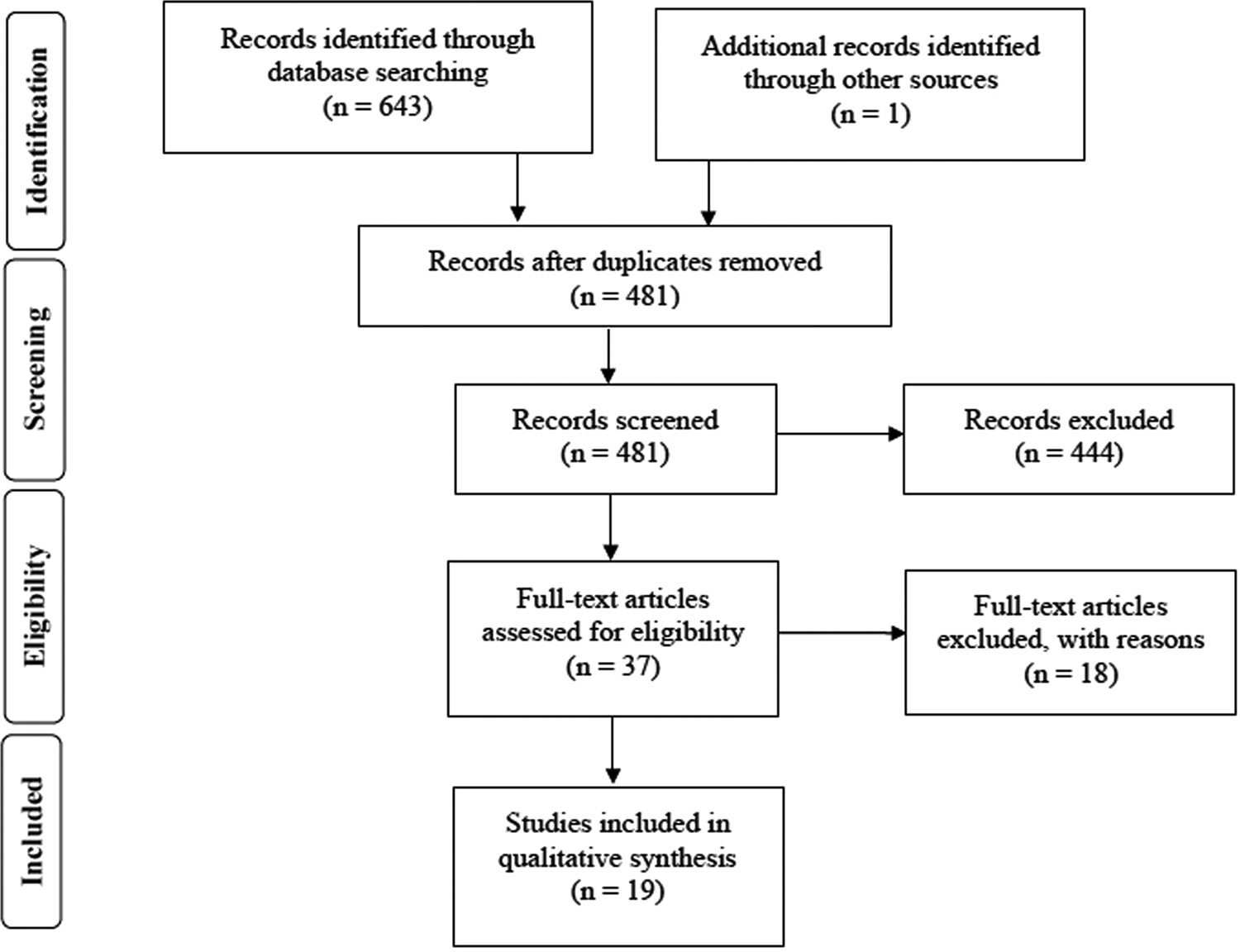
Figure 1. PRISMA flow diagram. The diagram depicts the selection of studies according to the guidelines of Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).
Coding
Included studies were categorized by diagnostic group, and relevant data were extracted according to the following codes: (a) author, title, and year of publication; (b) operational definition of SDS; (c) participant characteristics (ages, IQ, diagnosis, and grouping); (d) study design, methods, and measures; (e) primary outcomes; and (f) research quality. A brief tabulated overview of each study is included in the Supplementary Material. Although research quality was not an eligibility criterion, it was appraised to highlight the impact of reported outcomes (see Supplementary Material). The mixed-methods appraisal tool (Pace et al., Reference Pace, Pluye, Bartlett, Macaulay, Salsberg, Jagosh and Seller2011) allowed for concomitant appraisal of methodological quality in qualitative, quantitative, and mixed-methods designs. Extracted data were synthesized to provide a comprehensive narrative commentary.
Results
This section synthesizes findings on SDS relevant to each diagnostic group and the impact on regulation of thinking and behavior. Following this, the discussion highlights important issues across the reviewed research and emphasizes relevant directions for future research in the field.
Developmental language disorder
DLD, previously labeled specific language impairment, represents significant limitation in the acquisition of language not attributable to other developmental, neurological, or physical disorders. Language learning deficits in DLD relate to the understanding and use of phonology, morphology, syntax, semantics, or pragmatics (Tomblin et al., Reference Tomblin, Records, Buckwalter, Zhang, Smith and O'Brien1997). Interference in the ontogenesis of SDS is suggested by the very nature of DLD itself. Deficits in understanding or using language may impact the use and effectiveness of language as a thinking tool. Despite preserved nonverbal ability, several authors attribute poorer performance in self-regulation (Fujiki, Brinton, & Clarke, Reference Fujiki, Brinton and Clarke2002), executive functions (Finneran et al., Reference Finneran, Francis and Leonard2009), theory of mind (Farrant et al., Reference Farrant, Fletcher and Maybery2006), and visuospatial tasks (Windsor, Kohnert, Loxtercamp, & Kan, Reference Windsor, Kohnert, Loxtercamp and Kan2008), as exhibited in children with DLD, to the possible impact of language impairment on verbal mediation of thought.
Review of findings
The systematic search strategy uncovered four relevant research articles that investigate SDS in children with DLD. Current findings acknowledge the presence of SDS in children with DLD, yet suggest a level of interference in its development and consequential impact on the utility of SDS in regulating thinking and behavior.
Age level comparison across the reviewed studies suggests a maturational delay in the emergence and gradual internalization of SDS in children with DLD. Four-year-old children with DLD used less problem-solving language overall relative to typically developing peers during a play-based problem-solving task, most of which consisted of overt private speech (Sturn & Johnston, Reference Sturn and Johnston1999). Contrastingly, while completing the Tower of London task, 4- to 7-year-old children with DLD used a comparable amount of overt private speech to their peers but significantly less “inaudible muttering,” a feature of SDS internalization (Aziz, Fletcher, & Bayliss, Reference Aziz, Fletcher and Bayliss2017). During a play-based planning task, 6-year-old children with DLD used more private speech utterances overall than peers, but the difference in frequency per minute was not statistically significant (Kuvalja et al., Reference Kuvalja, Verma and Whitebread2014). Finally, in the eldest 7- to 11-year-old group, children with DLD used more overt and less internalized SDS than typically developing peers while completing the Tower of London and a digit span task (Lidstone et al., Reference Lidstone, Meins and Fernyhough2012). The combined findings of SDS frequency and form across age levels reflect a delayed maturational trajectory in both the emergence and internalization of SDS in children with DLD.
Broadly, the content of SDS in children with DLD appears similarly strategic to that of typically developing peers in that it is largely task relevant. While their study captured both private and social utterances in preschoolers, Sturn and Johnston (Reference Sturn and Johnston1999) determined the majority of utterances to be cognitively oriented in both groups. Although participants with DLD used less language overall, task-relevant utterances were proportionally similar between groups. Using Berk's (Reference Berk1986) coding scheme, Lidstone et al. (Reference Lidstone, Meins and Fernyhough2012) reported only two instances of task-irrelevant content within their entire data set, suggesting both children with DLD and their typically developing peers used a predominance of task-relevant content. Similarly, Aziz et al. (Reference Aziz, Fletcher and Bayliss2017) found that only 2.5% of total utterances were task irrelevant. Task relevance, however, is a broad marker, and future research may seek to delve more deeply into the metacognitive content of SDS.
Findings from Lidstone et al. (Reference Lidstone, Meins and Fernyhough2012) highlight that typically developing children and those with DLD equally rely on SDS as a regulator of thought, at least within a planning task. When the use of overt and internalized SDS was inhibited by articulatory suppression (i.e., repetition of verbal material unrelated to the task), both groups experienced significantly reduced accuracy in the completion of Tower of London problems. This finding implies that both groups use SDS, whether overt or internalized, as a verbal mediator of visuospatial planning. Coinciding with findings of delayed SDS internalization, authors interpreted delay rather than deviance in the development of SDS in children with DLD.
While children with DLD appear to rely on SDS for self-regulation, it may not function as effectively for this purpose. Four-year-old children with DLD who used more problem-solving speech during a play-based bridge building task measured as less cognitively efficient on the Kansas Reflective-Impulsivity Scale for Preschoolers (KRISP) (Wright, Gaughan, & McClanahan, Reference Wright, Gaughan and McClanahan1978). The opposite was true for children who were typically developing (Sturn & Johnston, Reference Sturn and Johnston1999). Indeed, there has been speculation that cognitive costs associated with verbalization may impact negatively on the efficacy of SDS in children with DLD at this age (Sturn & Johnston, Reference Sturn and Johnston1999). Kuvalja et al. (Reference Kuvalja, Verma and Whitebread2014) highlight SDS inefficiency in 6-year-old children with DLD during a Lego® play task that required the shortest route for postal delivery of six items. Using a new analytical approach, researchers subsequently identified significantly reoccurring temporal patterns of SDS and nonverbal behavior using a t-pattern detection algorithm (Magnusson, Reference Magnusson2000). During task completion, 580 events were coded for children with DLD and only 389 for children who were typically developing. Analysis also revealed a greater complexity of patterns in children with DLD, many of which contained SDS. Such findings suggest a regulatory inefficiency in private speech use for children with DLD. More recently, Aziz et al. (Reference Aziz, Fletcher and Bayliss2017) found that 4- to 7-year-old children with DLD used a similar amount of overt private speech as their typically developing peers, yet performed significantly worse on the Tower of London task. Furthermore, children with DLD and comorbid markers of hyperactivity used more overt private speech and performed worst on the task. While this finding corroborates earlier research to suggest reduced utility of SDS, Aziz and colleagues’ item-based probability analysis revealed that children with DLD were more accurate on trials when using overt private speech, and typically developing children performed comparably regardless of overt private speech use. Clearly, broad level comparisons do not provide a sensitive measure to support interpretation of regulatory efficacy. Future research may seek to reveal the mechanistic interaction between SDS and self-regulation in children with DLD. Is the regulatory function of private speech simply delayed in line with delayed internalization, or do specific features of SDS use or content impact negatively on its regulatory effectiveness?
General issues
It is important to remain mindful that the previously outlined comparisons are made in the context of methodological and sampling differences. One study included both social and private speech in their analysis (Sturn & Johnston, Reference Sturn and Johnston1999), whereas another concurrently investigated the validity of two new analytical measures of SDS (Kuvalja et al., Reference Kuvalja, Verma and Whitebread2014). The variability in identified studies highlights the emergent nature of this research and the need for further investigations to both corroborate and extend upon findings. All studies used variable forms of planning tasks to elicit SDS: two play tasks (Kuvalja et al., Reference Kuvalja, Verma and Whitebread2014; Sturn & Johnston, Reference Sturn and Johnston1999) and a structured visuospatial task (Aziz et al., Reference Aziz, Fletcher and Bayliss2017; Lidstone et al., Reference Lidstone, Meins and Fernyhough2012). It is difficult to determine whether these tasks placed differential demand on cognitive control, which could potentially influence SDS use.
The included studies used different instruments and cutoff scores in the identification of DLD. In the effort to achieve a defined clinical group and support justified comparison, researchers must begin to use similar measures and scores to identify participants with DLD. This is particularly the case because children with DLD can present with heterogeneity in their specific profile of language strengths and weaknesses. Lidstone and colleagues (Reference Lidstone, Meins and Fernyhough2012) encourage more comprehensive profiling of language abilities in future research to investigate the potential influence of different language profiles on aspects of SDS.
Autism spectrum disorder
ASD is a pervasive neurodevelopmental condition identified by impairment in social interaction, accompanied by restricted and repetitive behaviors and interests, in the presence or absence of language and intellectual impairment (APA, 2013). Although a broad level of heterogeneity exists in this population, cognitive domains typically implicated include theory of mind (Steele, Joseph, & Tager-Flusberg, Reference Steele, Joseph and Tager-Flusberg2003), executive function (Hill, Reference Hill2004), and communication (Geurts & Embrechts, Reference Geurts and Embrechts2008). With identified challenges across multiple areas of socially mediated higher order cognitive domains, it is not surprising that investigators hypothesize interference in SDS. Deficits in theory of mind have been hypothesized to negatively impact the ability to meta-represent one's own SDS and engage in a dialogic mode of thinking (Fernyhough, Reference Fernyhough2008; Williams et al., Reference Williams, Happé and Jarrold2008). Furthering this notion, research shows that typically developing preschool children who performed better in a mentalizing task were more aware of their own private speech (Manfra & Winsler, Reference Manfra and Winsler2006), a feature positively related to both its use and self-regulatory effectiveness (Winsler & Naglieri, Reference Winsler and Naglieri2003). Challenges in executive function tasks are well-profiled in children with ASD (Hill, Reference Hill2004), which some researchers argue are underpinned by paucity or failure of SDS in the verbal representation of novel and arbitrary rules required for such tasks (Russell, Jarrold, & Hood, Reference Russell, Jarrold and Hood1999).
Review of findings
In the time period encompassed by this systematic review, eight papers investigating SDS in children with ASD were identified, two of which provide a reanalysis of data from earlier studies (Lidstone et al., Reference Lidstone, Fernyhough, Meins and Whitehouse2009; Williams & Jarrold, Reference Williams and Jarrold2010). Six of the eight research papers engage experimental paradigms to investigate whether children with ASD use inner speech similarly to children who are typically developing. Both the design and interpretation of this research have been influenced by Baddeley's (Reference Baddeley1992) description of inner speech from his working memory model. Emergent findings from this research suggest that children with ASD do not use inner speech to the same extent as typically developing peers. However, conjecture remains regarding the cognitive features underpinning such differences, how findings should be interpreted in the broader sense of SDS deviance or delay, and whether SDS serves a self-regulatory function in this diagnostic group.
Limited recruitment of inner speech is evinced in findings from three original data sets (Holland & Low, Reference Holland and Low2010; Russell-Smith, Comerford, Maybery, & Whitehouse, Reference Russell-Smith, Comerford, Maybery and Whitehouse2014; Whitehouse, Maybery, & Durkin, Reference Whitehouse, Maybery and Durkin2006). Across three experiments, Whitehouse and colleagues (Reference Whitehouse, Maybery and Durkin2006) compared late primary-school-aged children with ASD with ability-matched controls on measures of inner speech use. Superior recall of pictures over words alone is proposed when using inner speech due to the susceptibility of pictures to dual verbal and visual encoding. Similarly, those recruiting inner speech are expected to display a word length effect, recalling more short than long words from visual stimuli due to capacity limitations of the phonological loop. Last, performance costs are expected under articulatory suppression, a condition that interrupts the use of SDS. In comparison with the typically developing control group, children with ASD demonstrated a lesser picture superiority effect, a lesser word length effect, and no significant performance cost in task switching under articulatory suppression—all findings indicative of limited inner speech recruitment. Likewise, Holland and Low (Reference Holland and Low2010) displayed limitation in the recruitment of inner speech in late primary-school-aged children with ASD and a tendency to rely more heavily on visuospatial resources. Children engaged in arithmetic task switching and the Tower of Hanoi under silent, articulatory suppression, and visuospatial suppression (i.e., repetitive tapping of four blocks in a specified pattern to interrupt visual encoding) conditions. While typically developing children took longer to complete tasks under both articulatory and visuospatial suppression, children with ASD experienced significant delays under visuospatial suppression only. Children with ASD relied more heavily on visual encoding, whereas typically developing peers tended to use both verbal and visual routes to regulate thinking. Corroborating these findings, the most recent investigation of private speech use in late primary-school-aged children with ASD points to disruption in the recruitment of both internalized and overt forms of SDS (Russell-Smith et al., Reference Russell-Smith, Comerford, Maybery and Whitehouse2014) as a regulatory tool. Russell-Smith et al. (Reference Russell-Smith, Comerford, Maybery and Whitehouse2014) had children with ASD and their typically developing peers complete the Wisconsin Card Sorting Task under four conditions: silent, articulatory suppression, concurrent mouthing, and talk-aloud. The talk-aloud condition actively encourages the use of overt private speech, articulatory suppression inhibits any form of SDS, and mouthing provides a control for any motor costs associated with articulatory suppression. While children with ASD did not display significant performance differences across conditions that manipulate SDS use, typically developing children performed significantly worse when SDS was inhibited and better when it was encouraged via the talk-aloud condition. Together, these findings suggest that children with ASD did not use SDS to the same extent as typically developing children in regulating task performance.
In contrast, Williams and colleagues’ (Reference Williams, Happé and Jarrold2008; Reference Williams and Jarrold2010) two papers using the same data set report intact use of inner speech in children with ASD but in the context of comparable verbal rather than chronological age. Participants included children with ASD with a mean age of 12 years, 3 months and comparison children matched on age and verbal ability who were either typically developing or possessed moderate learning difficulty. Participants completed a serial recall task using visual stimuli that were phonologically similar, visuospatially similar, or held neither form of similarity. The effect of similarity is proposed to diminish recall in the route used to encode stimuli, thus revealing a propensity for visual or verbal encoding. Analogous to Hitch, Woodin, and Baker's (Reference Hitch, Woodin and Baker1989) findings of a phonological similarity effect in children beyond 7 years; Williams and colleagues (Reference Williams, Happé and Jarrold2008; Reference Williams and Jarrold2010) discovered that, despite differing chronological ages, all participants possessing a verbal mental age of 7 or above showed a phonological similarity effect indicative of verbal recoding of visual information. A verbal mental age of 7 years or older, rather than diagnosis, appeared to be critical for the use of inner speech as a mediator of thought.
Further investigating the association between cognitive profile and inner speech use, Whitehouse and colleagues (Reference Whitehouse, Maybery and Durkin2006) reanalyzed their third experiment and found that both verbal and nonverbal IQ differences were required to account for discrepancies in inner speech recruitment in children with ASD (Lidstone et al., Reference Lidstone, Fernyhough, Meins and Whitehouse2009). In the arithmetic task-switching paradigm, those children with ASD and a predominately nonverbal cognitive profile did not recruit inner speech to the same extent as children with ASD and a more even profile of verbal and nonverbal ability. In response, Williams and Jarrold (Reference Williams and Jarrold2010) conceded to this finding in a reanalysis of their 2008 data but found that verbal mental age persisted as a stronger predictor of inner speech use. While ambiguity persists as to the cognitive features that may predict inner speech use in children with ASD, this approach emphasized the need to delve deeper than the diagnosis, somewhat heterogeneous in its grouping, into the specific nature of cognitive profiles to further understand mechanisms underpinning SDS use.
The majority of existing research on SDS in children with ASD has concentrated on inner speech with limited empirical consideration of overt private speech or its content. Winsler, Abar, Feder, Schunn, and Rubio (Reference Winsler, Abar, Feder, Schunn and Rubio2007) provide the only empirical observation of spontaneous private speech (i.e., overt to partially internalized) in children with ASD. The private speech of 7- to 18-year-old children with ASD was elicited during two computer administered executive function tasks (i.e., Wisconsin Card Sort Task and Building Sticks Task) and compared with that of age-matched children with ADHD and children who are typically developing. While a similar amount of task-relevant overt and covert private speech was present for all groups, researchers identify important associations with task difficulty and developmental trajectory. Thirty-nine percent of the children with ASD quit the Building Sticks Task prior to completion and displayed a trend toward greater frequency of private speech overall and more task-relevant content per item. On the Wisconsin Card Sorting Task, children with ASD were also more likely to get items correct when talking compared with their typically developing peers who were more likely to get items correct when silent. Perhaps these persisting markers of SDS immaturity highlight a greater degree of cognitive challenge in these tasks for children with ASD. As with previous research, overt private speech use was negatively correlated with increasing age for typically developing children (Winsler & Naglieri, Reference Winsler and Naglieri2003), but not so for children with ASD, whose overt private speech did not decrease with age.
Although speculative, it is questionable whether the previously outlined findings of inner speech interruption in children with ASD reflect a delay in SDS internalization rather than deviance in inner speech per se. Of the three original studies using articulatory suppression to investigate inner speech, one discouraged participant verbalization in the silent condition (Holland & Low, Reference Holland and Low2010), whereas the other two studies did not instruct participants to either use or inhibit private speech (Russell-Smith et al., Reference Russell-Smith, Comerford, Maybery and Whitehouse2014; Whitehouse et al., Reference Whitehouse, Maybery and Durkin2006). Although not reported, it is possible that spontaneous overt private speech was recruited in silent baseline conditions reflecting delayed internalization in those not recruiting inner speech to the same extent. Interestingly, however, in Russell et al.’s (Reference Russell-Smith, Comerford, Maybery and Whitehouse2014) talk-aloud condition, children with ASD used fewer words per minute and, in contrast with Winsler et al.’s (Reference Winsler, Manfra and Diaz2007) research, did not experience performance benefits to the same extent as typically developing children when using overt private speech. This finding could synonymously reflect a delay in the developmental trajectory of increasingly prominent overt private speech followed by later internalization, or equally limitation in the self-regulatory capacity of SDS used in this group. While a supposition of delay correlates with the findings of William and colleagues (Reference Williams, Happé and Jarrold2008; Reference Williams and Jarrold2010) who demonstrated intact inner speech when verbal mental age is considered, other explanations of qualitative difference or a combination of factors are plausible. In the context of Baddeley's (Reference Baddeley1992) working memory model, some researchers propose that findings of inner speech interruption in ASD reflect a dual coding deficit or challenge in flexibly shifting between verbal and visual strategies to service the regulation of cognitive processes in the central executive (Holland & Low, Reference Holland and Low2010; Russell-Smith et al., Reference Russell-Smith, Comerford, Maybery and Whitehouse2014). Other researchers have postulated that findings of increased propensity for visual over verbal encoding may reflect a compensatory response to reduced verbal ability and SDS regulatory effectiveness (Lidstone et al., Reference Lidstone, Fernyhough, Meins and Whitehouse2009; Russell-Smith et al., Reference Russell-Smith, Comerford, Maybery and Whitehouse2014). In particular, Lidstone and colleagues (Reference Lidstone, Fernyhough, Meins and Whitehouse2009) postulate that children with ASD and predominately nonverbal cognitive profiles select nonverbal skills as the most efficient strategy available to them. Indeed, Williams, Bowler, and Jarrold's (Reference Williams, Bowler and Jarrold2012) later investigation, albeit with adults, offers further insight into cognitive mechanisms that underpin the propensity for inner speech recruitment in this diagnostic group. Although adults with ASD recruited inner speech for a recall task, they did not appear to recruit inner speech for the purposes of planning and instead used visuospatial resources. Interestingly, the tendency to rely on visuospatial skills for planning correlated significantly with the severity of communication difficulty identified on the Autism Diagnostic Observation Schedule (ADOS) and the Autism Quotient (AQ). Researchers suggest that recruitment of inner speech is influenced by task-based requirements for monologic or dialogic inner speech, and that the development of dialogic inner speech required for planning tasks is likely affected by social communication challenges. A downward extension of such research with a childhood population is required to explore the developmental nature of such differences.
Findings regarding SDS content in children with ASD are limited. Winsler et al. (Reference Winsler, Manfra and Diaz2007) identified no significant difference in the amount of task-relevant private speech content in children with ASD and their TD peers. Although not empirically tested or compared with a normed group, Schaerlaekens and Swillen's (Reference Schaerlaekens and Swillen1997) case study observations of pre-sleep private speech content depict a preference for monologue in three young children with ASD as compared with the predominately dialogic content of two other children described as “psychotic.” Interestingly, Fernyhough (Reference Fernyhough2008) credits dialogic SDS as reflective of the ability to accommodate and represent multiple perspectives considered important for creative ability and social understanding.
General issues
In contrast to SDS research in children with DLD and ADHD, researchers primarily investigated the use of inner speech in children with ASD, with research paradigms driven by a working memory rather than a self-regulatory model of SDS. Extending on Winsler and colleagues’ (Reference Winsler, Manfra and Diaz2007) findings, further Vygotskian driven research that explores the spontaneous use of SDS will be advantageous in providing a more holistic picture of its use and self-regulatory effectiveness. Furthermore, there has been limited consideration of the spontaneous content of SDS in children with ASD engaged in social or learning-based tasks. In view of social understanding as a core deficit of ASD, there is a need for future research to move beyond the primary use of executive function tasks in an effort to explore the relationship between SDS and social emotional functioning also inherent in self-regulation. Finally, there is a dearth of SDS research in preschool or early primary school children with ASD, whose patterns may shed light on the developmental trajectory of SDS in ASD and further the understanding of delay or deviance.
Attention deficit hyperactivity disorder
ADHD is a developmental condition characterized by symptoms of hyperactivity, impulsivity, and inattention in excess of what is typical for developmental age (APA, 2013). The onset of symptoms occurs in childhood and can affect individuals across the life span. ADHD may be associated with academic underachievement or failure, social difficulties, mental health problems, and delinquency (Sibley et al., Reference Sibley, Pelham, Molina, Gnagy, Waschbusch, Biswas and Karch2011; Wehmeier et al., Reference Wehmeier, Schacht and Barkley2010). With identified challenges across social, emotional, and learning activities, a dysfunction of self-regulatory capacity has frequently been suggested in ADHD (Barkley, Reference Barkley2011).
A proposition of variation in developmental markers and self-regulatory efficacy of SDS in children with ADHD is not surprising given the Vygotskian position of SDS as critical to planning, monitoring, and guiding one's own goal-directed actions. Furthermore, Barkley's (Reference Barkley1997) widely accepted unifying theory of ADHD links a core deficit in inhibition to secondary deficits in four executive neuropsychological functions, including working memory, self-regulation of affect, reconstitution (i.e., creative use of past experience), and internalization of speech. Barkley (Reference Barkley1997) suggests that a delay of SDS internalization in ADHD negatively impacts upon the guiding function of SDS that he describes as fundamental to self-control, problem solving, moral reasoning, and metacognition.
Review of findings
ADHD holds the position as the earliest investigated developmental disorder in SDS research, and there are eight peer-reviewed research articles that meet the inclusion criteria for the present review. Among the developmental disorders considered in this review, this research provides the most robust picture of SDS in atypical development. The literature outlines a general consensus of delay along the curvilinear progression from overt to internalized SDS, and preponderance for task-irrelevant content. Interestingly, markers of SDS immaturity are noted to increase during periods of high cognitive demand and attenuate in response to psycho-stimulant medication. Conjecture remains as to the efficacy of SDS in this diagnostic group.
Delayed self-directed speech internalization
Corroborating Barkley's (Reference Barkley1997) hypothesis, investigations into SDS in children with ADHD provide a general consensus for delayed internalization. This delayed pattern of SDS maturation is evidenced by variation in SDS frequency and form when compared with that of typically developing children. Specifically, children with ADHD displayed a greater frequency of SDS use overall (Copeland, Reference Copeland1979; Reck, Hund, & Landau, Reference Reck, Hund and Landau2010), and a tendency to use more overt than partially internalized forms (Berk & Potts, Reference Berk and Potts1991; Lawrence et al., Reference Lawrence, Houghton, Tannock, Douglas, Durkin and Whiting2002; Winsler, Reference Winsler1998; Winsler et al., Reference Winsler, Manfra and Diaz2007), both features reflective of an immature patterning. In their exploration of ADHD, Lawrence et al. (Reference Lawrence, Houghton, Tannock, Douglas, Durkin and Whiting2002) asked boys ages 6 to 12 years old to play video games. Researchers coded occasions of overt task-relevant private speech, along with other event related actions to profile deficits according to Barkley's (Reference Barkley1997) unified theory of ADHD. In this everyday context, the boys with ADHD used more overt task-relevant private speech than typically developing peers. Similarly, Berk and Potts’ (Reference Berk and Potts1991) classroom-based exploration of private speech during an independent math activity identified an age-related shift from overt to internalized SDS in 6- to 12-year-old children with ADHD, which, although delayed by approximately 2 years, was parallel to that exhibited by typically developing children. Thus, although children with ADHD appear to use overt private speech for a prolonged period, it may eventually progress to its mature internalized form, at least within some tasks or situations. Future research that longitudinally investigates the SDS of children with ADHD across task types and situations would be beneficial to confirm the typical ontogenesis of SDS in this diagnostic group.
Task irrelevant self-directed speech content
With off-task behavior encapsulated by many of the ADHD diagnostic symptoms (APA, 2013), it is not surprising that five of eight studies report more task-irrelevant (Corkum, Humphries, Mullane, & Theriault, Reference Corkum, Humphries, Mullane and Theriault2008; Reck et al., Reference Reck, Hund and Landau2010; Winsler, Reference Winsler1998; Winsler et al., Reference Winsler, Manfra and Diaz2007) and immature (Copeland, Reference Copeland1979) SDS content in children with ADHD than that exhibited by typically developing peers. Copeland (Reference Copeland1979) provides the first empirical observation of SDS in children with an identified diagnosis of “hyperkinetic disorder,” now known as ADHD. Coding beyond the task relevant and irrelevant dichotomy, she found that 6- to 10-year-old “hyperactive” boys used more exclamations and descriptions of self rather than meta-cognitively rich planning statements while playing alone in a novel playroom for 3 minutes. In an object location memory task that investigated the use of SDS as a mnemonic tool, Reck et al. (Reference Reck, Hund and Landau2010) noted that boys with ADHD could remember locations as well as typically developing peers, but engaged a learning phase characterized by more task-irrelevant private speech, increased learning errors, and less attention to task. Although Berk and Potts’ (Reference Berk and Potts1991) research revealed no significant group differences in the amount of task-irrelevant private speech, the methodological parameters of this research only allowed for SDS coding when a child's attention to task was either moderate or focused, presentations likely to show a greater association with regulatory speech content and actions.
Task influence on self-directed speech
It is important to note that variation in the previously discussed markers of SDS immaturity may in fact reflect a more complex interaction between age, areas of cognitive weakness, and task demand or difficulty. Corkum et al. (Reference Corkum, Humphries, Mullane and Theriault2008) noted that two different task types, a problem-solving task and a behavioral inhibition task, elicited two representations positioned at different points on the curvilinear progression from overt to internalized SDS, in the same 6- to 11-year-old ADHD cohort. The problem-solving task elicited more overt and task-irrelevant private speech, whereas the behavioral inhibition task elicited more task-relevant and partially internalized SDS. Less mature SDS markers during the problem-solving task may suggest that this required a greater degree of cognitive control for those children with ADHD. Similarly, Winsler (Reference Winsler1998) found that two task types, a Lego® construction task and a sustained attention task, appeared to present different levels of cognitive challenge and differentially influenced SDS markers across both ADHD and typically developing groups. Although the results were more pronounced for the ADHD group, all children displayed reduced performance, poorer attention, more private speech, longer and more overt private speech utterances, and a greater incidence of task-irrelevant content during completion of the more challenging Lego® construction task. Findings of SDS interaction with task difficulty in ADHD imply the need for future research interpretation and design to account for variation in task challenges experienced by participants.
Self-directed speech efficacy
Although some of the research examining SDS in ADHD contemplates its regulatory efficacy, there remains conjecture as to whether SDS functions to enhance performance or behavioral engagement in children with ADHD. On broader measures of task performance, it would appear that the relationship between SDS use and performance is negligible (Corkum et al., Reference Corkum, Humphries, Mullane and Theriault2008; Reck et al., Reference Reck, Hund and Landau2010; Winsler, Reference Winsler1998; Winsler et al., Reference Winsler, Manfra and Diaz2007); however, micro-level analyses have uncovered some instances of interaction (Berk & Potts, Reference Berk and Potts1991; Kopecky, Chang, Klorman, Thatcher, & Borgstedt, Reference Kopecky, Chang, Klorman, Thatcher and Borgstedt2005; Reck et al., Reference Reck, Hund and Landau2010; Winsler et al., Reference Winsler, Manfra and Diaz2007).
Winsler's (Reference Winsler1998) investigation of bidirectional interactions between children's private speech use and parental scaffolding during a problem-solving task revealed that private speech was less related to ongoing activity and performance outcomes for children with ADHD in comparison with typically developing children. In this instance, Winsler (Reference Winsler1998) suggested that poorer scaffolding by parents of children with ADHD may constrain opportunity to use private speech for self-regulatory purposes. In a later study, Winsler et al. (Reference Winsler, Manfra and Diaz2007) found no significant correlation between private speech and overall task performance in children with ADHD and their typically developing peers while engaged in two computer administrated executive function tasks. However, when using a trial-level analysis, all children were more likely to use overt and covert private speech on failed trials in the problem-solving Building Sticks Task (Winsler et al., Reference Winsler, Manfra and Diaz2007). Likewise, Kopecky et al. (Reference Kopecky, Chang, Klorman, Thatcher and Borgstedt2005) noted an increase in overt private speech use during failed trials on the Tower of Hanoi. This effect was more pronounced for children with ADHD than their typically developing peers. Although these combined findings suggest that overt private speech use relates to failure or high cognitive demand, it is unclear what function it plays in this context. Does overt private speech function to support task engagement under increased cognitive load, or does it in fact prevent effective engagement leading to instances of failure? Kopecky et al. note that, overall, children with ADHD and typically developing children use more regulatory than non-regulatory utterances. Regulatory utterances are those that define, plan, monitor, or evaluate, the nature of which would suggest a facilitative function. Interestingly, these researchers also noted an increase in non-regulatory utterances during failed Tower of Hanoi trials. One could speculate as to whether such utterances reflect a reaction to failure or may in fact contain dysfunctional content that serves to impede performance. An investigation into the temporal patterns of private speech content and task-related behavior in ADHD could potentially shed light in this regard.
Beyond the measure of performance, Berk and Potts (Reference Berk and Potts1991) identified a relationship between SDS form and child engagement level during an independently completed math task. Focused attention was positively correlated with markers of internalized speech and negatively correlated with overt private speech for both typically developing and ADHD children. Simply, regardless of diagnostic status, children using more mature forms of SDS were more attentive to task.
Interpretations regarding the self-regulatory efficacy of SDS in ADHD to date are somewhat speculative. A movement from broad-level correlation between overall task performance and SDS to trial-level analysis presents a potentially more informative approach for future research.
Influence of medication on self-directed speech
The use of medication in children with ADHD raises questions with regards to the directionality of influence between SDS and self-regulation of cognition. Two of the reviewed studies explore shifts in SDS use in children with ADHD when the attentional system is augmented by methylphenidate (Berk & Potts, Reference Berk and Potts1991; Kopecky et al., Reference Kopecky, Chang, Klorman, Thatcher and Borgstedt2005). Methylphenidate is the drug most often prescribed to treat children with ADHD and is associated with improvements in teacher ratings of general behavior and ADHD symptoms (Storebø et al., Reference Storebø, Krogh, Ramstad, Moreira-Maia, Holmskov, Skoog and Gluud2015). From a sample of 19 boys with ADHD, Berk and Potts (Reference Berk and Potts1991) tracked eight boys both on and off psycho-stimulant medication. The use of medication was associated with movement toward increasingly mature markers of SDS use, demonstrated by a substantial reduction of overt private speech and a concomitant rise in partially internalized speech. Interestingly, medicated children using more covert forms of private speech also displayed corresponding improvement in motor quiescence and focused attention. Berk and Potts (Reference Berk and Potts1991), however, highlight methodological constraints, including a small sample size and absence of a placebo condition. Kopecky et al. (Reference Kopecky, Chang, Klorman, Thatcher and Borgstedt2005) also investigated the effects of psycho-stimulant medication on overt private speech content in 22 children with ADHD combined subtype and 19 children with ADHD predominantly inattentive subtype. Participants with ADHD took part in a randomly ordered double-blind clinical drug trial whereby a defined dosage of methylphenidate or placebo was administered over a period of 21 days. Overt private speech content was profiled over three sessions during the completion of Tower of Hanoi problems. Children with ADHD inattentive subtype displayed a reduction in overt private speech use during failed trials irrespective of pharmacological condition, whereas those with the combined ADHD subtype required medication to display such effects. Researchers suggest that children with ADHD predominantly inattentive subtype displayed a greater practice effect over the three sessions. Interestingly, all medicated children with ADHD displayed a reduction in non-regulatory content during failed trials, again suggestive of more refined and purposeful use. Findings of pharmacologically influenced attenuation of immature SDS markers highlight the importance of a washout procedure in research that investigates SDS in this diagnostic group.
A pharmacologically induced shift toward more sophisticated SDS use in children with ADHD poses important theoretical questions. Could it be that pharmacological intervention bolstered the attentional system and caused children to use more sophisticated and internalized speech (Berk & Potts, Reference Berk and Potts1991)? Interestingly, Barkley's (Reference Barkley1997) theory of ADHD identifies internalization of speech as one of four executive functions permitting self-control but posits that these functions are secondary to effective behavioral inhibition for their execution. This contradicts a commonly held Vygotskian understanding of SDS as a tool that exerts increasing control over cognitive processes as it progresses to inner speech. From a Vygotskian standpoint, immature SDS would underpin observed self-control weakness in children with ADHD. Acknowledging both positions, Berk and Potts (Reference Berk and Potts1991) propose theoretical expansion beyond a unidirectional explanation and advocate a bidirectional model of influence in the SDS and behavior relationship. In better understanding the mechanism by which SDS operates in ADHD, research may seek to further investigate the directionality of influence between SDS and a host of cognitive variables implicated in this developmental disorder, including behavioral inhibition, attention, language, and social understanding.
General issues
The research on SDS in ADHD has raised important avenues for continued investigation, specifically longitudinal investigation that both captures earlier SDS representations and confirms a delayed trajectory; the need to account for variation in task difficulty; trial-level analysis of SDS efficacy; and in-depth investigation of the directionality of influence between SDS and other cognitive variables in this diagnostic group. On a more general level, while all subjects were selected in accordance with relevant DSM criteria for the time-period, the identification of subjects with ADHD was achieved using a variety of different measurement approaches and tools. Although variation in diagnostic tools may be a consequence of the broad timespan within which this research has been completed, it would be beneficial for future researchers to align with a standardized procedure in so far as possible.
Discussion
Self-regulatory challenges inherent in children with neurodevelopmental disorders have far-reaching behavioral, social, and economic consequences across a lifetime (Blair & Diamond, Reference Blair and Diamond2008; Casey et al., Reference Casey, Somerville, Gotlib, Ayduk, Franklin, Askren and Shoda2011). Indeed, atypical SDS development holds significance as a common metacognitive control deficit in children with DLD, ASD, and ADHD, interfering with the ability to verbally regulate thought and action in service of goals. Not surprisingly, investigations of SDS in neurodevelopmental disorders have grown considerably in recent years. This emergent research provides snapshots of SDS use across age levels and diagnoses, often presenting conflicting results. In an effort to impose clarity in the current body of evidence, we undertook a systematic review that synthesizes and interprets the research to date.
The findings of this systematic review highlight differential development and use of SDS, an important self-regulatory tool, among children with the neurodevelopmental disorders DLD, ASD, and ADHD. Children with DLD and ADHD present with maturational delay regarding the emergence and use of SDS, and while SDS is harnessed as a self-regulatory tool for both groups it appears to be less effective for this purpose. In contrast, there is some evidence to suggest that children with ASD do not use inner speech to regulate thinking; however, this may be task-specific and influenced by cognitive profile features.
In an effort to further explicate the mechanism by which atypical SDS development interferes with self-regulatory capacity, a number of directions for future research are identified. As discussed in this section, researchers are encouraged to consider methodological limitations, the importance of cognitive profiling, the possibility of an impaired theory of speech, and the need to extend research beyond the child level and concomitantly explore the influence of social context across diagnostic groups.
Methodological issues
Variable methodology
Across the presently reviewed literature, variable theoretical perspectives have inspired a plethora of research questions and, consequently, research methods. Theoretical approaches range from a sociocultural Vygostkian approach to the information processing working memory model of Baddeley and Hitch (Reference Baddeley, Hitch and Bower1974), and diagnostic-specific theories such as Barkley's (Reference Barkley1997) theoretical account of ADHD. Thus, caution should be exercised when interpreting data derived from different research approaches, because such data may not represent the same functional or developmental significance. As achieved effectively across the reviewed literature, future research in this area should continue to specify the researchers’ theoretical stance, clearly specify research questions, and comprehensively outline methods. In recognition of the emergent nature of research in this area, it is likely that methods will continue to evolve. Researchers are encouraged to refer and contribute to Winsler, Fernyhough, McClaren, and Way's (Reference Winsler, Fernyhough, McClaren and Way2005) Private Speech Coding Manual. This working document aims to provide researchers with up-to-date methods for SDS coding and measurement.
Sampling challenges
The research under review included a large number of studies with small sample sizes. Additionally, many of the studies either did not include female participants or presented a larger male representation. Although recruitment challenges and a higher prevalence of males in the outlined disorders (Eric, Reference Eric2009; Tomblin et al., Reference Tomblin, Records, Buckwalter, Zhang, Smith and O'Brien1997; Willcutt, Reference Willcutt2012) present as sampling barriers, many researchers acknowledge these limitations and call for future research to avail of larger sample sizes and achieve a more balanced gender representation. Furthermore, researchers highlight the need for inclusion of younger samples with neurodevelopmental disorders in an effort to expand insights into the ontogenesis of SDS in such populations. The emergence of increasingly specific diagnostic tools for use with younger populations (e.g., ADOS-2), and the trend toward earlier diagnosis and intervention (Ozonoff, Reference Ozonoff2015) may allow future researchers to identify and recruit younger samples in these target populations.
Measurement of self-directed speech efficacy
The predominantly held Vygostkian understanding that posits SDS as a mediator of higher order cognitive functions suggests that it functions to support both engagement and performance across tasks. However, the self-regulatory efficacy of SDS in the profiled diagnostic groups remains somewhat equivocal. Despite identified variation in SDS frequency, form, and content in response to task difficulty, failure, and ongoing performance, interpretations remain speculative and fail to adequately answer whether aspects of SDS are facilitative, inhibitory, or incidental. Task difficulty level is a confounding factor in the measurement of SDS efficacy. Disparities in task types and individual ability within and across research studies may differentially influence SDS use and performance. In acknowledgment, Winsler (Reference Winsler1998) suggests movement beyond a single point in time concurrent correlations between speech and performance to the investigation of speech-performance relations either longitudinally or micro-genetically (i.e., examining moment to moment speech-action correspondences).
Moreover, chosen measures of SDS content across the reviewed research may not effectively profile the functional content of SDS across diagnostic groups. Six of the studies reviewed do not consider overt private speech content, whereas eight further studies avail of broad level categories that specify the presence or absence of task-relevant or regulatory content. Berk's (Reference Berk1986) commonly used three-category coding scheme may effectively profile the maturational trajectory of SDS form but lacks content-based specificity. Such broad level approaches may fail to explicate mechanistic aspects of SDS as a regulatory tool. A movement toward more sensitive metacognitive content measurement has the potential to reveal meaningful interactions between SDS content and self-regulatory effectiveness.
Self-directed speech and cognition
Fernyhough (Reference Fernyhough, Sokol, Müller, Carpendale, Young and Iarocci2010) suggests that SDS may relate to functional interaction across cognitive domains of language, executive functioning, and social understanding, and may be subject to shifting patterns of cognitive interaction across the course of development. The specific nature of the developmental relation between SDS and higher order cognition is far from established in the discussed diagnostic groups. The outlined research on SDS use in children with ASD highlights the need to move beyond diagnosis alone and consider specific differences in cognitive profiles that may influence the development of SDS, its selection as a metacognitive strategy, and its self-regulatory effectiveness across task types. This is further signified by identified heterogeneity within these neurodevelopmental disorders (Lidstone et al, Reference Lidstone, Meins and Fernyhough2012; Lord & Jones, Reference Lord and Jones2012), as well as the high incidence of comorbid challenges across cognitive domains (Dyck, Piek, & Patrick, Reference Dyck, Piek and Patrick2011). Future research may seek to reveal the complex ways in which SDS and aspects of higher order cognition interact, both in atypical and typical development. Researchers may use more comprehensive cognitive profiling of inter- and intra-individual differences in cognitive domains of language, executive functioning, and social understanding across development to better understand the mechanism of interaction between SDS and higher order thinking. In the reviewed research, SDS is typically elicited and examined during verbal recall or planning tasks. In better understanding the functional relations between SDS and wider aspects of self-regulation in children with neurodevelopmental disorders, researchers could also examine SDS during social understanding and emotional regulation task types. A deeper understanding of the neurocognitive mechanisms associated with SDS is key to facilitating improved intervention efforts.
Theory of speech
SDS is one of many forms of metacognitive behavior that serve to monitor, control, and regulate thinking. Recent research suggests that the emergence of metacognition is marked by implicit use prior to conscious awareness of metacognitive behaviors such as SDS (Manfra & Winsler, Reference Manfra and Winsler2006; Whitebread et al., Reference Whitebread, Almeqdad, Bryce, Demetriiou, Grau, Sangster, Efklides and Misailidi2010). Interestingly, this shift from implicit use to conscious awareness of SDS may hold regulatory significance. In typical development, a “theory of speech” or developing metacognitive knowledge of how private speech can be used may present a stimulus for children to use private speech in more purposeful ways (Manfra, Reference Manfra, Winsler, Fernyhough and Montero2009). Manfra and Winsler (Reference Manfra and Winsler2006) found that a conscious awareness of private speech was evident from 45 months in typically developing children. Those children with increased awareness of private speech held more positive views about its usefulness and availed of more task-relevant content. Furthermore, a theory of speech was positively correlated with task performance (Manfra, Reference Manfra2006; Winsler & Naglieri, Reference Winsler and Naglieri2003). Despite the emerging link between a theory of speech and its utility as a regulatory tool, research to date has not yet explored this concept in the neurodevelopmental disorders considered in this review. Future researchers may seek to investigate the stage at which children with DLD, ASD, or ADHD develop a theory of speech and its influence on markers of SDS maturity or regulatory efficacy. Of interest also in terms of intervention-based supports, one might question whether explicit instruction regarding a theory of speech could serve to influence the development and effectiveness of this metacognitive behavior.
Self-directed speech in collaborative interactions
Within the sociocultural approach, in particular, SDS is considered a product of social experience. Whether due to behavioral, social, or cognitive barriers, children with the outlined neurodevelopmental disorders may experience reduced quality of interaction with primary caregivers, likely to interfere with the development of SDS. Despite this widely held position, the literature captured by this review included only one study that considered the influence of social context on the use of SDS in children with ADHD (Winsler, Reference Winsler1998). This research identified that the bidirectional breakdown in parent-child interactions negatively influenced the gradual shift from other to self-regulatory speech behavior, particularly during difficult tasks. La Rocque and Winsler (Reference La Rocque, Winsler, Finestone and Lidstone2011) have extended such investigations to children with ASD and their parents; however, our criterion for publication form prevented the inclusion of this symposium presentation in the review. Similarly, this research identified poorer quality scaffolding in parents of children with ASD and reduced likelihood of private speech use following a collaborative session with parents. An extension of such research to investigate the quality of parent-child scaffolding and SDS use in children with DLD would be beneficial. Interestingly, La Rocque and Winsler's research (Reference La Rocque, Winsler, Finestone and Lidstone2011) also identified that reduced parental verbal control in a parent-child session was positively associated with children's private speech use and task performance in a follow-up individual session for children with ASD, ADHD, and typically developing children. Future research may seek to extend upon such findings and isolate the aspects of scaffolding that positively influence SDS use and task performance. Parent and teacher training in the use of such techniques may hold the potential to enhance the self-regulatory efficacy of SDS in children with neurodevelopmental disorders across both learning and social contexts.
Conclusion
In its synthesis and comparison of key findings, this review has sought to assert clarity on the current body of research that investigates SDS in children with DLD, ASD, and ADHD. Although well executed, the research provides snapshots of SDS use across time points and task types. While it is clear that differences exist in the development, use, and self-regulatory impact of SDS in these neurodevelopmental conditions, ambiguity pervades with regard to the precise nature and mechanisms of such differences. Additionally, many questions or areas for future consideration have emerged from this systematic review. What SDS patterns are evident longitudinally for each diagnostic group? Do specific cognitive profile differences underpin interruption in the development of SDS? Is the SDS of children with DLD, ASD, and ADHD less effective than their typically developing peers’, and how do we reliably measure this? Do children with neurodevelopmental disorders present with an impaired theory of speech? Would interventions that train parent- or teacher-led scaffolding support normalization in the development of SDS, and would this translate to improved task performance? It is hoped that these questions may provide a stimulus for future research.
Supplementary material
To view the supplementary material for this article, please visit https://doi.org/10.1017/S0954579418001670
Author ORCIDs
Aisling Mulvihill, 0000-0001-5157-5304; Paul E. Dux, 0000-0002-4270-2583
Financial support
Aisling Mulvihill is a recipient of the Australian Government Research Training Program Scholarship. Paul E. Dux was supported by an ARC Future Fellowship (FT120100033), and Paul E. Dux and Annemaree Carroll were supported by the ARC-SRI Science of Learning Research Centre (SR120300015).


