


Adolescence presents an array of opportunities for risk taking in the domains of substance use, sexuality, and aggressive or otherwise endangering behavior. Vulnerability to risk taking intensifies in adolescence partly due to the increased social influence of peers (Gardener & Steinberg, Reference Gardner and Steinberg2005) and the psychobiological changes of puberty (Steinberg, Reference Steinberg2008). Brain systems that regulate the processing of social information, emotions, and rewards are more easily aroused, while prefrontal networks that support self-regulation mature at a slower pace (Steinberg, Reference Steinberg2007). Some degree of risk taking by adolescents is therefore normative. However, in the present paper, we examine risky behavior from a developmental psychopathology perspective (Cicchetti & Toth, Reference Cicchetti and Toth2009; Sroufe, Reference Sroufe1997) and argue that adolescents with histories of early adversity will be particularly vulnerable to risk taking. Early adverse experiences, which involve stress and deprivation, as in the case of family poverty and child maltreatment, have been found to predict disturbance in a range of child and adolescent cognitive (e.g., executive function) and affective (e.g., reward processing and emotion regulation) capacities with relevance to risky behavior (Fisher et al., Reference Fisher, Lester, DeGarmo, Lagasse, Lin, Shankaran and Higgins2011; Pechtel & Pizzagalli, Reference Pechtel and Pizzagalli2011). In the present paper, we focus on low family income (relative to need) across infancy and early childhood as a dimension of early adversity with specific and enduring relevance to adolescent risk taking.
Moreover, identifying factors that either buffer or exacerbate the long-term effects of early adversity on risk taking is a crucial step in preventing risky behavior and its attendant morbidity and mortality. Relationships, and particularly the infant–caregiver attachment relationship, are a major route by which the environment impacts children's development, with the potential for these formative relationships to either ameliorate or heighten the effects of early adversity (Fisher et al., Reference Fisher, Beauchamp, Roos, Noll, Flannery and Delker2016; Luthar & Brown, Reference Luthar and Brown2007; National Scientific Council on the Developing Child, 2004). As such, informed by diathesis–stress models of development (Bowlby, Reference Bowlby1973, Reference Bowlby1979; Roisman et al., Reference Roisman, Newman, Fraley, Haltigan, Groh and Haydon2012), we examined whether history of infant–caregiver attachment security protects adolescents from the risk taking associated with childhood poverty, while infant–caregiver insecure–disorganized attachment exacerbates the association.
Risky Behavior and Its Potential Consequences
Risk taking involves a gamble, a willingness (that can border on heedlessness) to accept an immediate payoff at the potential cost of long-term harm or loss. Mishra and Lalumière (Reference Mishra and Lalumière2009) capture the instant gratification implied in risk taking with their definition of risky behavior as “impulsive, reckless behavior that maximizes short-term gains (e.g., sexual gratification, emotional arousal, relief of negative feelings) with potential for immediate or future costs (e.g., car accident, unwanted pregnancy)” (p. 40). Unfortunately, these costs can be substantial. For example, we know that injury is the leading cause of death among adolescents, with those aged 15 to 19 more likely to die from injuries sustained in motor vehicle traffic accidents and firearms than are younger children (Federal Interagency Forum on Child and Family Statistics, 2015). In the domain of sexual activity, risk for teenage pregnancy increases substantially for teens who do not use contraception. By age 17, adolescent females are more than five times as likely to be teen mothers if they did not use a method of contraception at their first experience of sexual intercourse (11%), compared to females who used contraception (2%; Martinez & Abma, Reference Martinez and Abma2015). Teen motherhood in turn is associated with lower educational attainment and a cycle of family poverty (Basch, Reference Basch2011). In the domain of substance use, we know that onset of substance use in early adolescence predicts a more rapid progression to substance use disorder for cigarettes and alcohol (Behrendt, Wittchen, Höfler, Lieb, & Beesdo, Reference Behrendt, Wittchen, Höfler, Lieb and Beesdo2009). Adolescent use of alcohol and other drugs is also associated with intentional (e.g., gunshot and stab wounds) and unintentional (e.g., falls and vehicular trauma) injuries, particularly for males (Spirito, Jelalian, Rasile, Rohrbeck, & Vinnick, Reference Spirito, Jelalian, Rasile, Rohrbeck and Vinnick2000). In addition, although the relation between adolescent substance use and academic performance is complex (King, Meehan, Trim, & Chassin, Reference King, Meehan, Trim and Chassin2006), research generally suggests deleterious effects (e.g., Meier et al., Reference Meier, Caspi, Ambler, Harrington, Houts, Keefe and Moffitt2012). These findings across multiple behavioral domains underscore the urgency of understanding and preventing risky behavior in this age group.
The Effects of Early-Life Socioeconomic Adversity on Risk Taking in Adolescence
Compared to children from middle- and high-income families, children from low-income families are more likely to be exposed to family and neighborhood violence, substandard housing and other material inequities, inadequate nutrition, low family social support, and parental stress and preoccupation related to the difficulties of meeting daily needs (Evans, Reference Evans2004; Wadsworth et al., Reference Wadsworth, Raviv, Reinhard, Wolff, Santiago and Einhorn2008). In social environments marked by harshness and uncertainty or scarcity of resources, the development of risk taking and its emphasis on short-term gain may be adaptive (Belsky, Schlomer, & Ellis, Reference Belsky, Schlomer and Ellis2012; Ellis, Reference Ellis and Hewlett2013) in certain circumstances, though as noted above, the long-term consequences of risky behavior may outweigh its advantages. Empirically, the specific association between economic hardship exposure in early childhood and risk taking has been examined with less frequency than related but distinct constructs such as externalizing behavior (Evans & Cassells, Reference Evans and Cassells2014; Wadsworth, Evans, Grant, Carter, & Duffy, Reference Wadsworth, Evans, Grant, Cartere, Duffy and Cicchetti2016) and stress-related disruptions to neuroendocrine development (Evans & Kim, Reference Evans and Kim2013; Lupien, McEwen, Gunnar, & Heim, Reference Lupien, McEwen, Gunnar and Heim2009).
Given the degree of conceptual overlap between externalizing behavior and risk taking, it is worth noting that some risk-taking behaviors may involve the “aggression, delinquency, and hyperactivity” that are characteristic of externalizing behavior (Liu, Reference Liu2004, p. 2), but many do not. For instance, smoking cigarettes, binge-drinking alcohol, and sexual intercourse without contraception are risk behaviors that do not necessarily involve aggression or delinquency, nor the operant or instrumental quality that the latter constructs imply. As such, risk behaviors may have more specific relevance to public health issues and outcomes than the construct of externalizing behavior. However, the literature on externalizing behavior is a useful touch point for the present inquiry, providing convergent evidence that, by mechanisms not yet fully understood, childhood socioeconomic adversity may predict risk taking later in development.
Several research teams have analyzed data from the National Longitudinal Study of Youth and found that low (relative to high) family household income in early childhood predicts higher rates of antisocial behavior and trajectories of increased antisocial behavior across early adolescence (Jarjoura, Triplett, & Brinker, Reference Jarjoura, Triplett and Brinker2002; Strohschein, Reference Strohschein2005). In another longitudinal study, male adolescents exposed to chronic poverty in early childhood were significantly more likely to exhibit chronic externalizing behavior problems than adolescents who did not experience childhood poverty or who experienced temporary poverty (Schonberg & Shaw, Reference Schonberg and Shaw2007). Family socioeconomic disadvantage in early childhood also has been linked to growth in impulsivity across early adolescence (Olson et al., Reference Olson, Sameroff, Lansford, Sexton, Davis-Kean, Bates and Dodge2013). In addition, in the specific domain of substance use, Daniel et al. (Reference Daniel, Hickman, Macleod, Wiles, Lingford-Hughes, Farrell and Lewis2009) conducted a systematic review of the literature on the association between early-life socioeconomic status (SES) and illicit drug use in adolescence and found a consistent association between childhood disadvantage and marijuana use, but not other illicit drug use.
A prevention study by Hawkins, Catalano, Kosterman, Abbott, and Hill (Reference Hawkins, Catalano, Kosterman, Abbott and Hill1999) illustrates how risk taking in adolescence can be averted by providing preemptive psychosocial support for elementary school-age children exposed to socioeconomic adversity. The authors conducted a psychosocial prevention program from first to sixth grades with children from a low-income, “high-crime” community and found that fewer children who received the intervention (compared to those in the control group) reported heavy drinking, sexual intercourse, multiple sexual partners, “violent delinquent acts,” or pregnancy by age 18 (Hawkins et al., Reference Hawkins, Catalano, Kosterman, Abbott and Hill1999). Of course, inherent within these findings on early poverty and adolescent risk taking is the reality that while many youths raised in economic disadvantage go on to engage in risky behaviors, many do not. A number of studies have examined individual and contextual protective factors, and among those, some have highlighted the importance of the early family context.
Early Caregiving Relationships as Mediators and Moderators of the Effect of Childhood Socioeconomic Adversity on Risk Taking in Adolescence
In infancy and early childhood, when children are most dependent on the caregiving adults in their lives, repeated interactions with caregivers are how children experience the world around them. Relationships have been called the “‘active ingredients’ of the environment's influence on healthy human development” (National Scientific Council on the Developing Child, 2004, p. 1), and as such, the caregiver–child relationship has been examined as a potential mediator and moderator of the effects of SES on development. For instance, Garwood, Gerassi, Jonson-Reid, Plax, and Drake (Reference Garwood, Gerassi, Jonson-Reid, Plax and Drake2015) found that childhood poverty (age range not reported) was a significant predictor of teen pregnancy by age 17, but this risk nearly doubled for those girls raised in poverty who also reported childhood interpersonal traumatization (i.e., abuse and neglect). Using statistical mediation, Belsky et al. (Reference Belsky, Schlomer and Ellis2012) applied an evolutionary framework to examine maternal depression and sensitivity in early and middle childhood as mediators of the effect of environmental harshness (low family income to needs across child age 1–60 months) on adolescents’ number of oral and sexual intercourse partners at age 15. The authors found that childhood income to needs ratio did not predict sexual behavior directly, but only indirectly, via lower levels of maternal sensitivity when the child was in the first and third grades (Belsky et al., Reference Belsky, Schlomer and Ellis2012). In addition, early childhood contextual risk, a construct that includes economic hardship, has been found to interact significantly with infant–caregiver attachment, such that infants with insecure attachment histories are more vulnerable to the adverse effects of contextual risk in early and middle childhood than infants with secure attachment histories (Belsky & Fearon, Reference Belsky and Fearon2002; Fearon & Belsky, Reference Fearon and Belsky2011). Building on this work, the present analysis investigates whether vulnerability related to the interaction between contextual adversity and infant–caregiver attachment extends into adolescence.
Secure Versus Disorganized Infant–Caregiver Attachment as a Buffer Against Risk Taking Associated With Low SES
Attachment theory provides a particularly relevant conceptual framework for considering the qualities of primary caregiving relationships that prospectively protect against risky behavior. Adolescents who experiment with sexual activity, drug use, and other risky behaviors in the context of new peer groups and social settings are, in a sense, exploring novel environments. Attachment theory proposes that one of the functions of the infant–caregiver attachment system is to provide a “secure base” for the child's exploration of novel environments (Carlson, Reference Carlson1998). Repeated early interactions with a caregiver who provides this secure base for child exploration will presumably help these children develop a set of stress-regulatory strategies and expectations of self and other in relationships that generalize beyond the attachment relationship to influence positive adaptation to novel social environments in childhood and adolescence (Kobak, Cassidy, Lyons-Ruth, & Ziv, Reference Kobak, Cassidy, Lyons-Ruth, Ziv, Cicchetti and Cohen2006).
The responsiveness and predictability of caregivers in secure dyads can be contrasted with the behavior of attachment figures in disorganized dyads. In the disorganized dyad, the primary caregiver's behavior in relationship to the child may be anomalous in ways described as frightened and/or frightening (Madigan et al., Reference Madigan, Bakermans-Kranenburg, van Ijzendoorn, Moran, Pederson and Benoit2006; Main & Hesse, Reference Main, Hesse, Greenberg, Cicchetti and Cummings1990). In what has been described as an “insoluble dilemma” (Madigan et al., Reference Madigan, Bakermans-Kranenburg, van Ijzendoorn, Moran, Pederson and Benoit2006, p. 90), the caregiver, who should be the source of comfort and safety, is a source of fear, confusion, and potential danger (Main & Hesse, Reference Main, Hesse, Greenberg, Cicchetti and Cummings1990). As the caregiver of the disorganized infant has not served as a consistent secure base from which the child has learned to explore novel environments safely, disorganized infants do not have reliable strategies for exploring the social environment in the presence of the caregiver. In consequence, when presented with a proliferation of novel environments across the transition to adolescence, a child with a history of disorganization may not be as sensitive to cues of potential threat in the environment. In support of this assertion, disorganized attachment in infancy predicts dissociation, a marker of decoupling between information about an event and the processing of that event as threatening (DePrince & Freyd, Reference DePrince, Freyd, Friedman, Keane and Resick2014; Kennedy et al., Reference Kennedy, Clarke, Stopa, Bell, Rouse, Ainsworth and Waller2004), at age 19 (Carlson, Reference Carlson1998). Moreover, evidence suggests that insecure–disorganized (vs. secure) attachment in early childhood is associated with middle-childhood impulsivity and deficits in inhibitory control (Bohlin, Eninger, Brocki, & Thorell, Reference Bohlin, Eninger, Brocki and Thorell2012; Jacobsen, Huss, Fendrich, Kruesi, & Ziegenhain, Reference Jacobsen, Huss, Fendrich, Kruesi and Ziegenhain1997; Kissgen & Franke, Reference Kissgen and Franke2016; Thorell, Rydell, & Bohlin, Reference Thorell, Rydell and Bohlin2012), constructs with strong links to externalizing behavior problems (Murray & Kochanska, Reference Murray and Kochanska2002; Schoemaker, Mulder, Deković, & Matthys, Reference Schoemaker, Mulder, Deković and Matthys2013; Sulik et al., Reference Sulik, Blair, Mills-Koonce, Berry and Greenberg2015) and complex links to risk taking (King, Patock-Peckham, Dager, Thimm, & Gates, Reference King, Patock-Peckham, Dager, Thimm and Gates2014). However, the long-term association between insecure–disorganized (vs. secure) attachment and later risk-taking behaviors in adolescence, along with the role of secure attachment as a protective factor in relation to early family economic hardship, is not yet well understood.
The Current Study
In this investigation, we examined infant–caregiver attachment security as a potential buffer against the increased adolescent risk taking associated with socioeconomic adversity in early childhood. We employed data from the NICHD Study of Early Child Care and Youth Development (SECCYD), a large prospective longitudinal study that involved multiple methods of data collection (NICHD Early Child Care Research Network, 2005). Extending prior work on predictors of adolescent risk taking focused on socioeconomic adversity in school-age children, we focused on poverty exposure specifically in infancy and early childhood, as evidence suggests that developmental processes with relevance to risk taking (e.g., inhibitory control) are already adversely impacted by poverty at this early stage (Hackman, Farah, & Meaney, Reference Hackman, Farah and Meaney2010; Moilanen, Shaw, Dishion, Gardner, & Wilson, Reference Moilanen, Shaw, Dishion, Gardner and Wilson2009). We indexed socioeconomic adversity with a cumulative measure of family income to needs assessed concurrently across child age 1–54 months. As an index of poverty status, the income to needs ratio has the advantage of being a parsimonious measure used widely across health and human services research on child development, with precise cutoffs indicative of poverty (<1.0) and near poverty (1.0–1.99; Newacheck, Hughes, Hung, Wong, & Stoddard, Reference Newacheck, Hughes, Hung, Wong and Stoddard2000).
We hypothesized that there would be a main effect of early socioeconomic adversity on adolescent risk taking, with children raised in poverty exhibiting greater risk taking at age 15 than their peers raised in relative affluence. Informed by work on the importance of early attachment relationships for later psychosocial development (Sroufe, Carlson, Levy, & Egeland, Reference Sroufe, Carlson, Levy and Egeland1999), we expected to find a main effect of infant–caregiver attachment at age 15 months on adolescent risk taking, with disorganized attachment history predicting greater risk taking than secure attachment history, regardless of early socioeconomic disadvantage. In the main test of our hypothesis, we anticipated an Attachment History × Early Poverty interaction, such that poverty during the first 4.5 years of life would predict risky behavior at age 15 for those teens who, as infants, had disorganized attachment relationships with their caregivers. We anticipated that this relationship would not emerge for those adolescents who had a secure attachment with their caregivers in infancy.
Tests of this moderation hypothesis controlled for individual and social-contextual factors known to be associated with increased (male sex of the child and ethnic minority status) and decreased (parental monitoring) risk-taking behaviors in adolescence (Delker, Noll, Kim, & Fisher, Reference Delker, Noll, Kim and Fisher2014; Dishion & McMahon, Reference Dishion and McMahon1998; Hawkins et al., Reference Hawkins, Catalano, Kosterman, Abbott and Hill1999; Kaplow, Curran, Dodge, & Conduct Problems Prevention Research Group, Reference Kaplow, Curran and Dodge2002; Patterson & Stouthamer-Loeber, Reference Patterson and Stouthamer-Loeber1984). In addition, to ensure that a long-term association between early childhood socioeconomic adversity and risk taking would not be confounded by concurrent family socioeconomic adversity in adolescence, the latter variable was included in the model as a covariate.
Method
Participants and procedure
NICHD SECCYD is a multisite, prospective longitudinal study of 1,364 children and their families designed to investigate the role of early childcare histories in the psychosocial development of children. Mothers giving birth at hospitals in 10 cities throughout the United States were screened for study eligibility during selected 24-hr sampling periods between January and November 1991. Exclusion criteria were (a) mother under 18, (b) family planned to move, (c) the child had obvious disabilities at birth or remained in the hospital more than 7 days postpartum, and (d) the mother was not conversant in English. After initial sampling, 5,265 met eligibility criteria and a subset was selected with a conditionally random sampling plan. A detailed description of study recruitment procedures and sample characteristics can be found in NICHD Early Child Care Research Network (2001).
Study assessments with children and their families occurred at 1 month (enrollment) and 6, 15, 24, 36, and 54 months. Later phases of the study followed these participants into childhood and adolescence, with a final assessment at child age 15. Regarding demographic characteristics at the sample level (N = 1,364), 48.3% (n = 659) of children were female and 51.7% (n = 705) were male. Mothers’ mean age in years was 28.11 (SD = 5.63), 76.5% were married and living together with a partner (n = 1,044), and 21% (n = 287) had no more than a high school education at child age 1 month. The ethnic identity distribution of the children was 80.4% White; 12.9% Black or African American; 1.6% Asian or Pacific Islander; 0.4% American Indian, Eskimo, or Aleutian; and 4.7% other. In addition, 6.1% of children were Hispanic. The mean family income to needs ratio averaged across child ages 1–54 months was 3.39 (SD = 2.69, range = 0.13–23.79).
The demographic characteristics of the subsample of children classified as having secure or insecure–disorganized attachment relationships with a primary caregiver at age 15 months (n = 887) differed in several respects from the rest of the sample. In general, this subsample appeared to be more socioeconomically advantaged. The mean family income to needs ratio across child age 1–54 months was significantly higher for this subsample (M = 3.57, SD = 2.72) than the rest of the sample (M = 3.06, SD = 2.62), t (1,353) = 3.30, p = .001, 95% confidence interval (CI) [0.21, 0.81]. Mothers in this subsample (M = 28.51, SD = 5.56) were significantly older, in years, than mothers in the rest of the sample (M = 27.36, SD = 5.70), t (1,362) = 3.60, p < .001. A significantly higher proportion of fathers lived with the child's mother in this subsample (n = 87.9%) than in the rest of the sample (79.5%), χ2 (1) = 17.48, p < .001. A significantly higher proportion of mothers was married in this subsample (80.4%), compared to the rest of the sample (69.4%), χ2 (1) = 20.87, p < .001. In addition, a significantly higher proportion of female children (51.5% female) were included in this subsample, compared to the rest of the sample (42.3% female), χ2 (1) = 10.45, p = .001. However, there were no significant differences between dyads with secure/insecure–disorganized histories and the rest of the sample in maternal education past high school (79.75% vs. 77.6%) and child ethnic minority status (18.3% vs. 22%). Among children with histories of secure and insecure–disorganized attachment, child ethnic identity distribution was 81.7% White; 11.2% Black or African American; 1.9% Asian or Pacific Islander; 0.5% American Indian, Eskimo, or Aleutian; and 4.7% other. In addition, 4.8% of children were Hispanic.
As is typical in longitudinal research, not all families remained in the study over time. By the wave of data collection at child age 15 years, 979 participants remained (71.77% of the original sample of 1,364). Children who participated in the final wave of study data collection at age 15 did not differ significantly from those who dropped out on the basis of child ethnic minority status, χ2 (1) = 1.72, ns, male sex of the child, χ2 (1) = 3.26, ns, or attachment at age 15 months, χ2 (1) = 0.34, ns. However, children who participated in the final wave of study data collection at age 15 were raised in families with significantly higher income to needs ratio levels (M = 3.56, SD = 2.63) across child age 15 months than families who dropped out (M = 2.91, SD = 2.79) of the study, t (1,353) = 3.96, p < .001.
These findings suggest that some data points in the current investigation are missing at random, meaning data are missing for a knowable reason. In longitudinal research such as the SECCYD study, some attrition will be truly random (missing completely at random) and some, in this case, attributable to a known reason: the higher attrition of low-income families. As such, findings should be interpreted with caution, given potential bias to model estimates associated with these missing data processes. This issue is addressed further in the Analysis Plan and Discussion sections.
Measures
Early childhood family income to needs
At each wave of data collection in early childhood at 1, 6, 15, 24, 36, and 54 months, the family reported their household income, family size, and family composition, and received an income to needs ratio score based on the ratio of household income to the federal poverty line at that time. Higher scores indicate more resources relative to needs, with scores below 1.00 indicative of poverty. For instance, in 1992, the poverty threshold for a family of four was an annual household income of $13,950 (Fisher, Reference Fisher1992); these families would have an income to needs ratio of 1.00.
Internal consistency reliability of the income to needs ratio scores across the six data collection waves in early childhood was excellent (α = 0.94). Following a method used by Fearon and Belsky (Reference Fearon and Belsky2004) in their work on attachment and social–contextual adversity in the SECCYD data set, we averaged family income to needs ratio scores across these six waves, yielding an average income to needs ratio score for early childhood.
Families with scores below 1.00 on the average income to needs ratio score are considered to be living in poverty (<100% poverty level), and families with scores between 1.00 and 1.99 are considered to be living in near poverty (between 100% and 199% poverty level). There was a precedent in the literature for referring to this 100%–199% poverty group as living in “near poverty” (e.g., Wadsworth et al., Reference Wadsworth, Evans, Grant, Cartere, Duffy and Cicchetti2016) with similar predictive validity for the <100% and 100%–199% groups. For instance, Newacheck et al. (Reference Newacheck, Hughes, Hung, Wong and Stoddard2000) found that the percentage of children with unmet health needs was 11.6% if <100% poverty, 11.9% if 100%–199% poverty, and 3.6% if >200% poverty. In the SECCYD data set, adolescent risk-taking behaviors differed significantly between children at or below 100% poverty level, t (952) = 4.16, p < .001, and at or below 200% poverty level, t (952) = 5.11, p < .001, providing empirical support that both the <100% group and the <200% group are vulnerable to long-term adverse outcomes.
Attachment in infancy
Infant–mother attachment security was assessed with the Ainsworth Strange Situation Procedure (Ainsworth, Blehar, Waters, & Wall, Reference Ainsworth, Blehar, Waters and Wall1978) at child age 15 months. Strange Situation videotapes were evaluated by trained coders who passed the University of Minnesota Attachment Test Tapes for A-B-C classifications (Fearon & Belsky, Reference Fearon and Belsky2004). In addition, coders had “previous experience coding Strange Situations from a variety of low- and high-risk samples, received additional training using master-coded tapes (including tapes coded by Mary Main), and intensive supervision continued during formal scoring to maintain expertise” (Fearon & Belsky, Reference Fearon and Belsky2004, p. 1680). Each Strange Situation videotape was analyzed and classified using the standard classifications: secure (B), insecure–avoidant (A), insecure–resistant (C), and disorganized (D). The subsample of infants who received B (n = 719) or D (n = 177) classifications is the primary focus of the current report. In addition, 102 children received a C classification and 160 an A classification.
Risk taking in adolescence
At age 15, adolescent risky behavior was assessed with a 55-item measure, “Things I Do,” designed for use in the SECCYD. Items were developed on the basis of work by Conger and Elder (Reference Conger and Elder1994), the Fast Track project (Conduct Problems Prevention Research Group, 2002), and the New Hope project (Huston et al., Reference Huston, Miller, Richburg-Hayes, Duncan, Eldred, Weisner and Redcross2003). Adolescents were asked how many times in the past year they engaged in 55 risky behaviors with response options not at all (0), once or twice (1), and more than twice (2). To score the risk-taking items, the SECCYD team recoded the items to be never (0) or once or twice or more than twice (1) and computed a total score from the sum of response values for each item. Items encompassed adolescent safety, violence-related behaviors, sexual behavior, and alcohol, tobacco, and marijuana use. Sample items are “driven a car without a seatbelt,” “done something dangerous on a dare,” “carried a hidden weapon,” “broken into a building to steal,” “smoked cigarettes/used tobacco,” and “had oral sex.” Internal consistency reliability of the 55 items was excellent, α = 0.90.
Parental monitoring in adolescence
Parental monitoring was assessed with an 11-item questionnaire for parents on parental supervision and monitoring of the adolescent's activities, such as knowledge of the teen's whereabouts after school and setting times to be home on school and weekend nights (Lamborn, Mounts, Steinberg, & Dornbusch, Reference Lamborn, Mounts, Steinberg and Dornbusch1991; Steinberg, Lamborn, Darling, Mounts, & Dornbusch, Reference Steinberg, Lamborn, Darling, Mounts and Dornbusch1994). Cronbach α for the 11 items was 0.77 for mothers and 0.84 for fathers. To create a parental monitoring score, the SECCYD team of investigators computed the mean of Items 1–11 for parents, with total possible scores ranging from 1 to 4. Higher scores indicate greater parental monitoring.
Family income to needs in adolescence
Consistent with how family income to needs was calculated in early childhood, families with scores below 1.00 on the average income to needs ratio score at adolescent age 15 are considered to be living in poverty (<100% poverty level) and families with scores between 1.00 and 1.99 are considered to be living in near poverty (between 100% and 199% poverty level; Newacheck et al., Reference Newacheck, Hughes, Hung, Wong and Stoddard2000).
Male child
Sex of the child was assessed with a single item from the first wave of study data collection at 1 month, male (1) or female (0).
Child ethnic minority status
Child race/ethnicity was assessed at the first wave of study data collection as American Indian, Eskimo, Aleutian (1), Asian or Pacific Islander (2), Black or African American (3), White (4), or other (5). Child ethnic minority status was indexed as a binary variable by recoding White as 0 and all other ethnic categories as 1.
Analysis plan
Hayes’ PROCESS method of moderation analysis is well suited to conducting moderation analysis with a multicategorical moderator. Using SPSS (version 22) with Hayes’ PROCESS for SPSS version 2.16.1, we specified a moderation model to test the interaction between childhood poverty (X) and infant–caregiver attachment classification (a multicategorical moderator with four levels: A, B, C, D) at age 15 months (W) in predicting risk-taking behavior in adolescence (Y) at age 15. The multicategorical moderator, attachment, was indicator-coded in PROCESS with the B (secure) group as the indicator group, yielding three “dummy” variables (A vs. B, C vs. B, and D vs. B, the focal comparison of this analysis). Additional model constraints controlled for the association of risk taking with sex of the child (male), child ethnic minority status, and parental monitoring and concurrent family socioeconomic adversity in adolescence. The parental monitoring variable was mean centered prior to the analysis.
First, we probed the significant XW interaction between childhood poverty and D versus B attachment in a two-stage process. In probing the XW interaction, we treated the moderator (W) as dichotomous (D vs. B) and focused only on the interaction between D versus B attachment and childhood poverty, controlling for all other variables and interaction terms in the analysis. We calculated simple slopes and plotted the association between X and Y at the two values of W (D vs. B attachment classification) using a web utility (Preacher, Curran, & Bauer, Reference Preacher, Curran and Bauer2006) and R web. Second, we calculated the region of significance for the XW interaction (Preacher et al., Reference Preacher, Curran and Bauer2006). In the case of a dichotomous moderator and continuous predictor, the region of significance refers to the specific values of X at which the regression of W on Y moves from nonsignificance to significance. To determine the region of significance, we employed the web utility by Preacher et al. (Reference Preacher, Curran and Bauer2006) that produces R syntax for generating confidence bands and a region of significance plot.
As mentioned previously, there was attrition in the SECCYD, with data missing at random and missing completely at random. The Hayes PROCESS macro used listwise deletion to exclude cases missing the age 15 outcome data on risk taking, and as such, there is the potential for PROCESS model estimates to be biased. However, in support of the PROCESS findings, an equivalent model specified in Mplus with full-information maximum likelihood using a template for Hayes’ PROCESS method of testing moderation using bootstrapping (Hayes, Reference Hayes2013; Stride, Gardner, Catley, & Thomas, Reference Stride, Gardner, Catley and Thomas2015) and a bivariate moderator yielded the same significant XW interaction between childhood poverty and D versus B attachment (Mplus model results available from the authors upon request).
Results
Across child age 1–54 months, 28.6% (n = 254) of children in the subsample of adolescents with secure or insecure–disorganized infant–caregiver attachment histories were living at or near poverty level (income to needs less than 200% of poverty level). At child age 15 months, 719 dyads were classified as B and 177 as D in the Strange Situation procedure, meaning that 19.75% of the analytic sample was classified as disorganized. Cumulative family income to needs across child age 1–54 months did not differ significantly between children with secure (M = 3.63, SD = 2.71) versus insecure–disorganized (M = 3.29, SD = 2.72) attachment histories, t (885) = –1.52, p = .129.
Table 1 presents frequencies of risk-taking behaviors at age 15 for the B/D subsample. The mean number of risk-taking behaviors in the B/D subsample was 5.93 (SD = 5.68). Riding a bike without a helmet or a car without a seatbelt were the most common risk-taking behaviors, reported by almost half of the sample. Almost a quarter of the sample had drunk alcohol at least once, and more than 10% had smoked cigarettes or used tobacco at least once. About 10% of the sample reported having sexual intercourse at least once, and about 10% reported having oral sex at least once.
Table 1. Frequencies of major risk-taking behaviors at age 15 for adolescents with histories of secure and insecure-disorganized attachment to caregivers

Note: N = 674 at Study of Early Child Care and Youth Development wave when child age 15. These 15 risk behaviors were selected from the 55-item questionnaire as representing risk taking in the major domains of substance use, sexual activity, and aggressive or otherwise endangering behaviors. Items are sorted from highest to lowest frequency of occurrence more than twice.
Table 2 presents model results from the main moderation analysis with the full sample at age 15 (N = 810). Consistent with our hypothesis about the main effect of infant–caregiver attachment history, adolescents with insecure–disorganized (D) attachment histories exhibited significantly more risk taking in adolescence than adolescents with B attachment histories, holding constant family income to needs in early childhood. Adolescents with insecure–avoidant (A) and insecure–resistant (C) attachment histories did not exhibit significantly more risk taking in adolescence than adolescents with secure attachment histories, holding constant family income to needs. As predicted, there was a significant main effect of family income to needs ratio across early childhood on adolescent risk taking. Across attachment history groups, higher family income to needs in early childhood predicted less risk taking in adolescence.
Table 2. PROCESS model results for the multicategorical moderation analysis

Note: N = 810. ITNR, mean family income to needs ratio across child age 1–54 months; A, B, C, and D, dyadic attachment classifications in the Ainsworth Strange Situation Procedure at child age 15 months; ITNR at age 15, a bivariate categorical variable coded as 1 if family ITNR was at or below 1.99 (i.e., 200% poverty) at child age 15 and 0 if above 1.99; Par. monitoring at age 15, a parent report of parental monitoring; LLCI, lower limit 95% bootstrap confidence interval; ULCI, upper limit 95% bootstrap confidence interval.
As predicted, childhood socioeconomic disadvantage and attachment at age 15 months interacted significantly to predict adolescent risk taking (see Figure 1 and Table 3). The main effects of family income to needs ratio and D versus B attachment history on risk taking remained significant alongside the interactive effect, providing support for partial, not full, moderation. If raised in poverty (family income to needs at or below 1.02, or 1 SD below the sample mean) compared to affluence (family income to needs at or above 6.16, or 1 SD above the sample mean) adolescents with secure attachment histories exhibited double the risk behaviors (7.56 vs. 3.78), simple slope B = –0.18 (0.09), t (798) = –2.04, p = .042. The association between childhood family poverty and risk taking was stronger for adolescents with disorganized attachment histories, who exhibited nearly five times the number of risk behaviors if raised in poverty (10.85 risk behaviors) than if raised in affluence (2.40 risk behaviors), simple slope B = –0.64 (0.18), t (798) = –3.51, p = .001. Thus, the effect of socioeconomic disadvantage on risk taking is dampened for adolescents with secure attachment histories, as compared to insecure–disorganized attachment histories (but not as compared to insecure–avoidant or insecure–resistant attachment histories). R 2 increase as a result of the interaction was only marginally significant, likely due to the lack of significant interaction between early childhood family income to needs and adolescent insecure–avoidant or insecure–resistant attachment histories, ΔR2 = .0073, F (3, 798) = 2.30, p = .076.

Figure 1. History of secure versus insecure–disorganized attachment to caregivers moderates the association between cumulative family income to needs ratio in early childhood and risk taking in adolescence.
Table 3. Descriptive statistics for the prediction of risky behaviors at age 15 from family income to needs ratio moderated by secure versus insecure–disorganized attachment history

Note: N = 674. Income, family income to needs ratio averaged across child age 1–54 months; Low, income to needs ratio of 1.02 (≤17th percentile, or 1 SD below the mean); Medium, income to needs ratio of 3.59 (18th–82nd percentile); High, income to needs ratio of 6.16 (≥83rd percentile, or 1 SD above the mean).
Calculation of the region of significance for the interaction between childhood socioeconomic disadvantage and D versus B attachment at age 15 months (see Figure 2) revealed that when raised in poverty or near poverty (family income to needs below 2.24, or below about 220% poverty level, corresponding to the 30th percentile of this sample), adolescents with histories of disorganized attachment to caregivers exhibited significantly more risk behaviors at age 15 (M = 9.93, SD = 8.28) than their peers with histories of secure (M = 6.73, SD = 4.97) attachment (B = 1.15, SE = 0.58, t = 1.96, p = .05). When raised in relative affluence (family income to needs 2.24 or above), number of risk-taking behaviors do not differ between adolescents with insecure–disorganized (M = 4.63, SD = 4.20) and secure (M = 5.35, SD = 5.65) attachment histories.
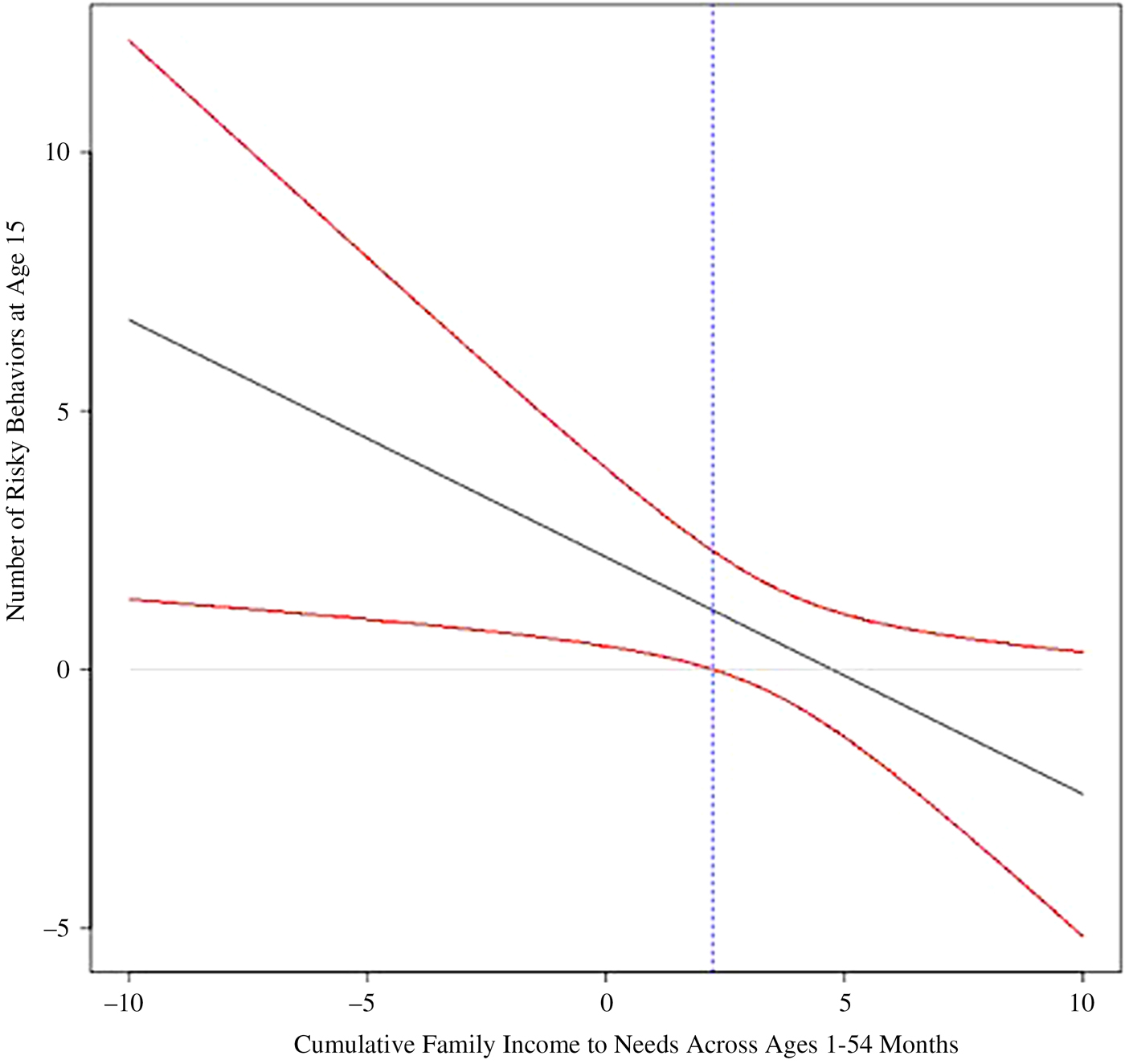
Figure 2. (Color online) Region of significance plot for the interaction between cumulative family income to needs ratio in early childhood and history of secure versus insecure–disorganized attachment to caregivers. The area to the left of the vertical dashed line to X = 0 represents the region of significance. A family income to needs ratio of 2.24, or about 220% poverty level, is the specific value at which the regression of disorganized (vs. secure) attachment history on risk taking moves from nonsignificance to significance.
This significant moderation finding was obtained while controlling for the effect of several covariates on risk taking. Male adolescents (M = 7.17, SD = 6.32) demonstrated significantly greater risk taking than females (M = 5.15, SD = 4.73).Footnote 1 Adolescents identified as ethnic minorities (M = 8.66, SD = 7.72) demonstrated significantly greater risk taking than White adolescents (M = 5.37, SD = 4.98). Moreover, the significant moderation finding held while controlling for the significant effects of concurrent parental monitoring and family income to needs at child age 15 on adolescent risk taking. Adolescents living in families with income to needs levels at or near poverty reported significantly more risk-taking behaviors (M = 8.10, SD = 6.28) than adolescents with family income to needs above this level (M = 5.58, SD = 5.34). The association between parental monitoring at age 15 and adolescent risk taking was in the expected direction, with increased parental monitoring associated with less adolescent risk-taking behavior.Footnote 2
Effect size
Overall, the multicategorical moderation model explained 16% of the variance in adolescent risk taking at age 15, R 2 = 0.16, F (11, 798) = 13.77, p < .001.
Discussion
The purpose of the present paper was to investigate infant–caregiver attachment security (vs. disorganization) as a buffer against the association between childhood socioeconomic adversity and risk taking in adolescence. The NICHD SECCYD data set provided an ideal basis for inquiry into risk/resilience mechanisms associated with early adversity and caregiver–child attachment. First, the sample was socioeconomically diverse, resulting in variability important for testing the differential influence of lower versus higher childhood family income on adolescent risk taking. Second, the large sample size of this national, multisite study resulted in a substantial subset of children who had been in insecure–disorganized attachment relationships in infancy, enabling an adequately powered test of differences associated with this relatively rare attachment classification. Third, the SECCYD's longitudinal data collection from birth to age 15 provided a unique opportunity to prospectively investigate long-term outcomes of early attachment.
Our findings support the role of early attachment quality as a partial moderator of the association between family economic hardship in early childhood and risk taking in adolescence. At the sample level, for adolescents with both secure and insecure attachment histories, economic hardship in early childhood predicted increased risk taking at age 15. The relation between early economic hardship and risk taking was dampened for adolescents with histories of secure (vs. insecure–disorganized, but not insecure–resistant or insecure–avoidant) attachment, pointing to a significant interaction between early attachment history and family income to needs in predicting risk taking at age 15. If raised in poverty (family income to needs at or below 1.02, or approximately 100% poverty level), compared to affluence (family income to needs at or above 6.16), adolescents with secure attachment histories exhibited two times the number of risk behaviors, whereas adolescents with disorganized attachment histories exhibited almost five times the number of risk behaviors (see Figure 1 and Table 3). The precise cutoff at which secure attachment history was associated with protective reductions in risk taking was a family income to needs ratio below 2.24, or approximately 220% poverty level. If raised in poverty or near poverty, adolescents with disorganized attachment histories reported significantly more risk-taking behaviors than adolescents with secure attachment histories. The long-term association between these early developmental contexts and later risk taking is particularly noteworthy when considering that the focal moderation finding was observed above and beyond the effect of concurrent family economic hardship in the child's adolescence.
Our findings offer points of both convergence with and divergence from theory and longitudinal research on early adversity and attachment as they relate to developmental psychopathology. The present finding that history of insecure–disorganized attachment to caregivers predicts increased risk taking in adolescence is consistent with longitudinal research demonstrating that early attachment disorganization relates to behavior problems throughout the school years and psychopathology at age 17.5 (Carlson, Reference Carlson1998). Moreover, in the current study, only history of insecure–disorganized attachment to caregivers, not insecure–avoidant or insecure–resistant attachment, predicted increased risk taking, highlighting the vulnerability of insecure–disorganized relative to insecure–organized attachment relationships. For instance, in a meta-analytic study, Fearon, Bakermans-Kranenburg, van IJzendoorn, Lapsley, and Roisman (Reference Fearon, Bakermans-Kranenburg, van IJzendoorn, Lapsley and Roisman2010) found that children with disorganized attachment histories demonstrated greater risk for externalizing behavior problems relative to children with insecure–avoidant or insecure–resistant histories.
Evidence suggests that when the persons on whom a child trusts or depends are sources of threat, as in the case of child maltreatment, sustained effects of these experiences on risk taking may be observed into adolescence and young adulthood (e.g., Weller, Leve, Kim, Bhimji, & Fisher, Reference Weller, Leve, Kim, Bhimji and Fisher2015). As such, insecure–disorganized attachment, a characteristic pattern among children with caregivers who are sources of fear and potential danger (Cyr, Euser, Bakermans-Kranenburg, & van IJzendoorn, Reference Cyr, Euser, Bakermans-Kranenburg and van Ijzendoorn2010; Main & Hesse, Reference Main, Hesse, Greenberg, Cicchetti and Cummings1990), may be associated prospectively with increased risk taking in adolescence due to disruptions in emotional processing generally (McLaughlin, Reference McLaughlin2016) and threat processing specifically (Bernstein & Freyd, Reference Bernstein and Freyd2014; Cassidy & Mohr, 2011; Ein-Dor, Mikulincer, & Shaver, Reference Ein-Dor, Mikulincer and Shaver2011; Forbes, Phillips, Silk, Ryan, & Dahl, Reference Forbes, Phillips, Silk, Ryan and Dahl2011). Of note, in the current study, the prospective association between insecure–disorganized attachment in infancy and risk taking in adolescence was qualified by a significant interaction between attachment and socioeconomic context across early childhood. As such, the current findings are consistent with a diathesis–stress model (Roisman et al., Reference Roisman, Newman, Fraley, Haltigan, Groh and Haydon2012) in which adolescents with insecure–disorganized attachment histories are most vulnerable to the adverse effects of early economic disadvantage. A diathesis–stress model has been supported by previous work on early adversity and attachment in the SECCYD data set (Belsky & Fearon, Reference Belsky and Fearon2002).
The finding that family income to needs predicts risk taking regardless of early attachment history or concurrent family income to needs in adolescence raises the important question of what specific dimensions of poverty or near poverty in early childhood, from age 1 month to 4.5 years, explain increased rates of risk taking for all adolescents. The unpredictable and potentially chaotic living conditions of low-income families (Evans, Gonnella, Marcynyszyn, Gentile, & Salpekar, Reference Evans, Gonnella, Marcynyszyn, Gentile and Salpekar2005) may contribute to both behavioral and psychobiological adaptations to this chronically stressful environment. For instance, the unpredictability, uncertainty about whether basic needs will be met, and punishing conditions of poverty may incentivize risk taking to avoid losses, a behavioral pattern seen in children exposed to chronic early adversity (Weller & Fisher, Reference Weller and Fisher2013). In addition, chronic environmental stress is known to shape the development of the body's stress physiology, resulting in alterations to neural systems and executive functions important for self-regulation (Blair & Raver, Reference Blair and Raver2012; Fisher et al., Reference Fisher, Beauchamp, Roos, Noll, Flannery and Delker2016). To the extent that risk taking involves deficits in self-regulation that remain stable from early childhood to adolescence (Boyer, Reference Boyer2006), the disinhibited phenotype associated with early adversity may partially explain the increased risk taking associated with family economic hardship. In a sample of adopted children, Laurent et al. (Reference Laurent, Neiderhiser, Natsuaki, Shaw, Fisher, Reiss and Leve2014) found that early-childhood exposure to family adversity (home chaos and high parental stress and psychopathology), and not simply shared genetic influences, contributed to hypothalamus–pituitary–adrenal axis hyper- and hypoactivity and to emotional dysregulation at child age 6. Further longitudinal research is needed to determine the extent to which these behavioral and neuroendocrine disruptions associated with early adversity place children on pathways associated with adolescent risk taking.
Children with histories of both early socioeconomic disadvantage and insecure–disorganized attachment to caregivers may experience a double dose of uncertainty and unpredictability in both the living environment and their relationships with caregivers, explaining the exacerbating effect of disorganized attachment history observed in the current study. For children with secure attachment histories, the stable, reliable “secure base” provided by the caregiver–child relationship may help these children develop an internal working model that serves as a persistent buffer against the inconsistency of the wider social environment. Future research on decision making in the face of risky outcomes can clarify how the decision-making process differs between adolescents with secure versus insecure–disorganized attachment histories, who were and were not exposed to socioeconomic disadvantage in early childhood. For instance, intriguing questions with implications for intervention are how adolescents with secure attachment histories and histories of socioeconomic disadvantage make decisions that protect them from risk, and whether adolescents with disorganized attachment histories and histories of socioeconomic disadvantage are unaware that the decisions they make are risky, or are aware of that risk but fail to heed it (Delker & Freyd, Reference Delker and Freyd2014).
Several potential implications for preventive intervention on adolescent risk taking emerge from the present findings. For children raised in poverty or near poverty, supporting early attachment security may be a particularly important prospective buffer against later risk taking and its associated morbidity and mortality. Of course, there are many other reasons why safe, stable, and nurturing early relationships with early caregivers benefit children's development (Centers for Disease Control and Prevention, 2009). In conceptualizing attachment security as a buffer against the deleterious impact of childhood poverty, we want to be careful that this empirical effort to identify protective factors in socioeconomically disadvantaged children's lives does not preclude addressing and intervening on the complex structural and systemic forces that perpetuate family poverty in the United States. Of additional clinical relevance, adolescents who were identified by their parents as ethnic minorities took more risks than their White peers, regardless of attachment history or family SES in early childhood and adolescence. This finding underscores the urgency of funding preventive interventions that will promote the well-being particularly of adolescents who are racial or ethnic minorities. In addition, more research is needed to understand individual differences in risk taking within racial and ethnic minority groups in the United States, along with racial and ethnic promotive or protective factors within and between groups (Neblett, Rivas-Drake, & Umaña-Taylor, Reference Neblett, Rivas-Drake and Umaña-Taylor2012).
While the present inquiry was focused on the early infant–caregiver attachment relationship as a moderator of the prospective association between early environmental risk and later functioning, it is important to acknowledge the strong association between concurrent parental behaviors in adolescence and risk taking. In the present study, the strongest predictor of adolescent risk taking was concurrent parental monitoring (i.e., supervision and knowledge) of adolescent activities. This finding is consistent with extensive prior research among sociodemographically diverse populations of adolescents demonstrating that parental monitoring of adolescent activities and peer environments is associated with a range of positive psychosocial outcomes, including reductions in problem behavior across early adolescence (Fosco, Stormshak, Dishion, & Winter, Reference Fosco, Stormshak, Dishion and Winter2012), less initiation of sexual activity across the transition from middle to high school (Ethier, Harper, Hoo, & Dittus, Reference Ethier, Harper, Hoo and Dittus2016), and fewer negative consequences associated with substance use (Branstetter & Furman, Reference Branstetter and Furman2013). As such, parental monitoring in adolescence remains an important target of preventive intervention on adolescent risk taking.
The present findings should be considered with regard to several limitations. First, while SECCYD recruitment was conducted to ensure adequate family demographic diversity, particularly high-risk families were underrepresented. For instance, no families with mothers younger than age 18 at the time of the child's birth were recruited into the study. As such, our finding on the buffering effect of secure attachment history may not extend to adolescents from the highest risk socioeconomic backgrounds, an empirical question that can be tested with future research. Second, while the longitudinal design of this study and its multimodal measurement methods lend credibility to the statistical moderation analysis, the data are of course correlational, and it remains possible that unidentified “third variables” explain the relation between early attachment and long-term development. This limits the strength of the current conclusions that can be drawn about the role of disorganized (vs. secure) attachment history in the development of risk taking, and of course, further replication of the present findings is needed. A longitudinal intervention study that supports security of infant–caregiver attachment among families living in poverty or near poverty and follows up with children in adolescence to measure rates of risk taking would help clarify the extent to which attachment plays a causal role in risk-taking outcomes (Cassidy, Jones, & Shaver, Reference Cassidy, Jones and Shaver2013). Third, an important question remains for developmental and clinical science: at what point does risk taking extend beyond the normative range for the developmental stage of adolescence and become a maladaptation?
The current study places adolescent risk taking in a social and developmental context by considering the role of the infant–caregiver attachment relationship in buffering adolescents from the deleterious outcomes associated with exposure to poverty and near poverty in the family of origin. In addition to contributing to the literature on the protective advantages of early attachment security, our findings contribute to the literature on diathesis–stress models of development, showing that early poverty is a particularly salient risk factor for development in the context of insecure–disorganized attachment to caregivers.





