



Early-life exposure to environmental stress has a central role in shaping long-term emotional and behavioral development (Boyce & Ellis, Reference Boyce and Ellis2005; Kessler et al., Reference Kessler, Davis and Kendler1997). Early exposure to adversities can cue biologically adaptive strategies for given environments (Belsky et al., Reference Belsky, Schlomer and Ellis2012); however, when that given environment changes (e.g., moving from home to kindergarten) the same adversities can compromise mental and physical health (McLaughlin, Green, et al., Reference McLaughlin, Green, Gruber, Sampson, Zaslavsky and Kessler2010). The overall impact of adversities on health and functioning is generally negative – even devastating for some − with evidence of a dose-dependent association of such exposures on risk for a range of developmental outcomes (Copeland et al., Reference Copeland, Shanahan, Hinesley, Chan, Aberg, Fairbank and Costello2018; Evans & Kim, Reference Evans and Kim2007; Sameroff et al., Reference Sameroff, Bartko, Baldwin, Baldwin, Seifer, Lewis and Feiring1998; Trentacosta et al., Reference Trentacosta, Hyde, Shaw, Dishion, Gardner and Wilson2008). At the same time, different adversities may affect children in different ways based upon distinct aspects of the adversities themselves as well as how the experience is perceived by the child. For example, violence within one’s neighborhood may be perceived as an ongoing threat or danger to the child while death of a parent or sibling from an illness may be perceived primarily as a significant loss to one’s family network. While the long-term negative impact of early adversities is well established, this study aims to test the long-term impact of specific dimensions of childhood adversity. Two recent theories have revived this discussion: one focused on maladaptive development of psychopathology (McLaughlin et al., Reference McLaughlin, Sheridan and Lambert2014; Sheridan & McLaughlin, Reference Sheridan and McLaughlin2014), and the other focused on evolutionarily adaptive development (Ellis et al., Reference Ellis, Figueredo, Brumbach and Schlomer2009). Each model posits and finds empirical evidence for, distinct core dimensions of early adversity.
A dimensional model of neurodevelopmental adversity
The dimensional model of adversity and psychopathology (DMAP) theory aims to identify central mechanisms underlying the strong link between childhood adversity and subsequent psychopathology (Sheridan & Mclaughlin, Reference Sheridan and McLaughlin2014). In this work, Sheridan and McLaughlin theorize and empirically examine how two core, nonindependent dimensions of childhood exposures exhibit distinct negative influences on neural development, which, in turn, increase risk for psychopathology (McLaughlin et al., Reference McLaughlin, Sheridan and Lambert2014; Miller et al., Reference Miller, Sheridan, Hanson, McLaughlin, Bates, Lansford and Dodge2018; Sheridan et al., Reference Sheridan, Peverill, Finn and McLaughlin2017). They propose that exposure to deprivation, a lack of cognitive stimulation and learning opportunities, leads to dramatic increases in synaptic pruning in association cortex, impairing cognitive functioning whereas exposure to threat, involving harm or threat of harm, leads to biasing of biological fear learning systems and subsequently impaired emotion regulation.
These child adversity dimensions may yield distinct transdiagnostic markers of psychopathology, proximal to their theorized neurocognitive mechanism. For instance, early exposure to deprivation has been found to contribute specifically to the proximal outcome, poor cognitive functioning (Bos et al., Reference Bos, Fox, Zeanah and Nelson Iii2009; Eigsti et al., Reference Eigsti, Weitzman, Schuh, de Marchena and Casey2011; Pollak et al., Reference Pollak, Nelson, Schlaak, Roeber, Wewerka, Wiik and Gunnar2010; Sheridan et al., Reference Sheridan, Peverill, Finn and McLaughlin2017; Tibu et al., Reference Tibu, Sheridan, McLaughlin, Nelson, Fox and Zeanah2016), when measured by results from neuropsychological testing, questionnaires of executive functioning, and neural functioning during cognitive control tasks (Johnson et al., Reference Johnson, Policelli, Li, Dharamsi, Hu, Sheridan and Wade2021). Early exposure to threat has been found to contribute specifically to the proximal outcome, emotion regulation, when measured by attention to emotional faces and fMRI results from mood induction paradigms (Gold et al., Reference Gold, Sheridan, Peverill, Busso, Lambert, Alves and McLaughlin2016; McCrory et al., Reference McCrory, De Brito, Kelly, Bird, Sebastian, Mechelli and Viding2013; McLaughlin et al., Reference McLaughlin, Peverill, Gold, Alves and Sheridan2015; Pollak & Tolley-Schell, Reference Pollak and Tolley-Schell2003). However, as theorized, specificity becomes mixed when general psychiatric problem types are measured as outcomes (Henry et al., Reference Henry, Gracey, Shaffer, Ebert, Kuhn, Watson and Compas2021; Miller et al., Reference Miller, Sheridan, Hanson, McLaughlin, Bates, Lansford and Dodge2018, Reference Miller, Machlin, McLaughlin and Sheridan2021). Results from Miller et al. (Reference Miller, Sheridan, Hanson, McLaughlin, Bates, Lansford and Dodge2018, Reference Miller, Machlin, McLaughlin and Sheridan2021) support their hypotheses, finding that although deprivation and threat both uniquely contributed to broad-band externalizing symptoms, only deprivation was mediated by cognitive functioning mechanisms (language). Dimensions of childhood adversity, therefore, may be more likely to exhibit specificity to mechanism-proximal outcomes (i.e., deprivation to cognitive functioning), and less so to psychiatric disorders (i.e., deprivation to externalizing vs. internalizing problems), which are inherently influenced via multiple neurodevelopmental systems.
A dimensional model of evolutionary risk and adaption
The life history (LH) theory explains developmental biological strategies that link childhood exposures to evolutionary-fitness outcomes (Ellis et al., Reference Ellis, Figueredo, Brumbach and Schlomer2009). This theory is distinct from other models in emphasizing how core dimensions of childhood exposures cue strategies for individuals to be successful given the specific demands of their environment (i.e., biological adaptation). The theory argues that from an evolutionary perspective the maladaptive psychiatric outcomes are tradeoffs resulting from developmental adaptations to stress. Thus, the focus should be on how such experiences affect functional outcomes that relate to LH strategies. The core dimensions of childhood adversity that both uniquely contribute to an individual’s adaptive biological strategy are cues of the morbidity-mortality rate in the environment called Harshness and the in/consistency of that rate over time called Unpredictability. These experiences determine whether reproductive strategies will be fast, such as engaging in more sexual activity early in life to increase the odds of early reproduction, or slow, such as engaging in less sexual activity early in life to delay reproduction and be able to invest more time and effort in offspring. Higher Harshness and more Unpredictability in one’s early environment are hypothesized to each contribute to faster reproductive strategies due to risk of early death and/or more uncertainty in their future opportunities to reproduce.
These hypotheses were tested by the theorists themselves in a longitudinal study that followed children from birth to 17 years using maternal report and observational methods (Belsky et al., Reference Belsky, Schlomer and Ellis2012). Harshness – cueing of morbidity-mortality rate – was operationalized as family poverty status (adjusted for family size) and unpredictability as an accumulation of paternal transitions, parental job transitions, and household moves. Both were assessed across 17 interviews during early childhood (0–5 years). As predicted, both adversity dimensions were associated with more sexual partners in early adolescence (age 15). Although the focus in that analysis was on an outcome relating to reproductive success (i.e., sexual partners), Ellis and Belsky theorized that additional outcomes relating to “growing, mating, and eventually reproducing” such as cognitive, emotional, physiological, and behavioral functioning would also be affected. This theory was supported in another longitudinal study demonstrating that individuals with high Unpredictability in early childhood (0–5 years) not only had more sexual partners at age 23 but also exhibited more criminal activity and aggressive behaviors (Simpson et al., Reference Simpson, Griskevicius, Kuo, Sung and Collins2012).
How risk unfolds across development
Both theories have generated hypotheses about core dimensions of child adversity strongly forecasting proximal (closely related to theorized neural mechanism or reproductive success) outcomes, and perhaps to a lesser extent, distal outcomes (generally related to theorized neural mechanisms such as psychiatric diagnoses, or evolutionary-fitness outcomes such as functional outcomes of general health, economic status, conduct/criminality, and social relationship quality). These complex relationships are further complicated by time and the developmental transitions it brings. The effect of time is person-dependent. For instance, child adversity impact may be attenuated as individuals have time to recover or find ways to cope (Graber et al., Reference Graber, Seeley, Brooks-Gunn and Lewinsohn2004). Thus, it could be that results demonstrating dimension-outcome specificity concurrently are no longer associated, or less strongly associated, over longer periods of time. Alternatively, early adversity may alter the course of development long-term contributing to developmental cascades of difficulties wherein early specific problems end up affecting a broader range of domains over time (Masten & Cicchetti, Reference Masten and Cicchetti2010). In this way, dimension-outcome specificity in the short term may become widespread and endemic in the long term.
A few studies have tested such long-term outcomes of the DMAP and LH theories. In DMAP theory, Miller Reference Miller, Sheridan, Hanson, McLaughlin, Bates, Lansford and Dodge2018 and Reference Miller, Machlin, McLaughlin and Sheridan2021) found that early Threat and Deprivation (age 3–6) both uniquely contributed to externalizing problems at ages 5, 9, 15, and 17, via distinct pathways such that only Deprivation was mediated by language ability. For LH theory, researchers found that Harshness and Unpredictability in the first 5 years of life both uniquely contributed to number of sexual partners at age 15 and 23 and as criminal and aggressive behaviors (Belsky et al., Reference Belsky, Schlomer and Ellis2012; Simpson et al., Reference Simpson, Griskevicius, Kuo, Sung and Collins2012). Results from DMAP and LH longitudinal studies suggest proximal outcomes remain significant over time and there also may be robust impact on distal outcomes. Theory-proximity and timing may each moderate the association strength and specificity of child adversity dimensions impact on outcomes.
Other dimensions
The LH dimension of harshness is heterogeneous both in terms of its definition – anything that cues morbidity and mortality – and in how it has been operationalized. In describing harshness, the following examples are provided: residence in a dangerous neighborhood low socioeconomic status, and repeatedly attending funerals (Ellis et al., Reference Ellis, Figueredo, Brumbach and Schlomer2009, p. 253). In empirical studies, harshness has been defined as income-to-need to income ratio (Belsky et al., Reference Belsky, Schlomer and Ellis2012), and self-reported exposure to violence (Brumbach et al., Reference Brumbach, Figueredo and Ellis2009), These examples and measures suggest a broad range of experiences including many that are typically included in threat and deprivation dimensions (Lambert et al., Reference Lambert, King, Monahan and McLaughlin2017; Miller et al., Reference Miller, Machlin, McLaughlin and Sheridan2021; Sheridan et al., Reference Sheridan, Peverill, Finn and McLaughlin2017), but also experiences that involve loss. To address this heterogeneity, we examine components of harshness in the DMAP theory (i.e., threat and deprivation) separately. In addition, we introduce a third component of harshness, loss.
Loss events including those involving death of a friend or loved one been suggested as another core dimension of child adversity (McLaughlin et al., Reference McLaughlin, Sheridan and Lambert2014), which has been shown to operate on a distinct set of neuro-correlates from deprivation and/or threat (Gündel et al., Reference Gündel, O’Connor, Littrell, Fort and Lane2003). Loss has been studied extensively as a dimension of child adversity and has been associated with multiple domains of functioning (psychiatric and functional impairment (Luecken, Reference Luecken, Stroebe, Hansson, Schut and Stroebe2008; Pham et al., Reference Pham, Porta, Biernesser, Walker Payne, Iyengar, Melhem and Brent2018), however, it has not been modeled in relation to other core dimensions of child adversity. Here we include loss as another dimension of early adversity.
Finally, all of these dimensions taken together: threat, deprivation, unpredictability, and loss, do not account for all early childhood risks that may affect later functioning. Other stressful and potentially traumatic events include incidental, often natural, noninterpersonal events (e.g., natural disasters, car accidents, sickness) and such experiences have been found to have an important role in the development of physical and psychological problems (McLaughlin, Conron, et al., Reference McLaughlin, Conron, Koenen and Gilman2010; Monroe, Reference Monroe2008). Such events must be accounted for to estimate the individual contribution of each of the adversity dimensions accurately. Therefore, all analyses will include a scale of other adverse childhood experiences to avoid omitted variable bias and provide a robust test of the unique contribution of each dimension.
The current study
This study proposes to test the effect of these multiple childhood adversity dimensions on a broad range of adult outcomes both proximal and distal to DMAP and LH theories including outcomes that specifically index “real-world” functioning. This study will test which dimensions have effects that persist into adulthood (long-term risk), on which outcomes (differential impact), and in what manner (risk or adaptive effects). In addition, by looking at multiple dimensions at the same time, the study has the potential to compare the associations observed with this dimension-based approach to a cumulative adversity approach in which all events are summed into a single heterogeneous scale without respect to underlying features of the events. Even for distal outcomes, a cluster of carefully constructed individual dimensions may better predict outcome better than a broad scale of adversities with indiscriminate weighting. This study will compare these two approaches to understanding long-term risk.
Method
Procedure
The Great Smoky Mountains Study is a longitudinal, representative study of children in 11 predominantly rural counties of North Carolina (see Costello et al., Reference Costello, Mustillo, Erkanli, Keeler and Angold2003). Three cohorts of children, ages 9, 11, and 13 years at intake, were recruited from a pool of some 12,000 children in the area using a household equal probability, accelerated cohort design. The accelerated cohort design means that each cohort reaches a given age in a different year, controlling for cohort effects. First, potential participants were randomly selected from the population using a household equal probability design. Next, participants were screened for risk of psychopathology; participants screening high were oversampled in addition to a random sample of the rest. About 8% of area residents and sample are African American and fewer that 1% are Hispanic. American Indians makeup 3% of the population of the study, but were oversampled to constitute 25% of the sample. This design resulted in N = 1,420 participants (49% female). Sampling weights are applied to adjust for differential probability of selection. Thus, the statistical estimates presented here are representative of the population from which the sample was drawn.
Annual assessments were completed on the 1,420 children until age 16 (6,674 observations of 1,420 individuals; 1993–2000) and then again at ages 19, 21, 25, and 30 (4,556 observations of 1,336 participants; 1999–2015) for a total of 11,230 total assessments. Interviews were completed by a parent figure and the participant to age 16, and by the participant only thereafter. Before any interviews, the parent and child signed informed consent/assent forms. The study protocol and consent forms were approved by the Duke University Medical Center Institutional Review Board. Each respondent received an honorarium for their participation.
Missing data
Across all waves, 81.8% of all possible interviews were completed ranging from 74% to 94%. 100% of participants completed at least 1 assessment by age 16 (period childhood adversity assessed) and 94.3% had 3 or more assessments (median = 7). Ninety-three percent of living participants had an adult assessment (ages 25 or 30 when outcomes assessed). Three of the four childhood adversity dimensions were associated with attrition before age 25. Participants who continued in the study (n = 1,274) compared to those with missing data at age 25 and 30 (n = 145) experienced less Threat, Material Deprivation, and Unpredictability, but there were no differences in Loss.
Measures
Childhood adversity dimensions
All childhood adversity dimension items except where noted (e.g., deprivation, maternal depression) were assessed using the Child and Adolescent Psychiatric Assessment (CAPA) interview (Angold & Costello, Reference Angold and Costello1995, Reference Angold and Costello2000), which was administered to the participants and their primary caregiver annually from study entry (9, 11, or 13) until 16. Most events were collected as part of the Life Events module which has been shown to display test-retest reliability and discriminant validity (Costello et al., Reference Costello, Angold, March and Fairbank1998). If either information endorsed the event at any interview up to age 16, it was marked as present. Events were sorted into child adversity dimensions based upon previous empirical works examining that dimension (Lambert et al., Reference Lambert, King, Monahan and McLaughlin2017; Miller et al., Reference Miller, Sheridan, Hanson, McLaughlin, Bates, Lansford and Dodge2018; Sheridan et al., Reference Sheridan, Peverill, Finn and McLaughlin2017) for DMAP and (Belsky et al., Reference Belsky, Schlomer and Ellis2012) for LH). A child received a “1” if they ever experienced an event and a “0” if not, and all events were summed within each dimension. All dimension and cumulative scores were winsorized at 96% or above (Kokic & Bell, Reference Kokic and Bell1994).
DMAP dimensions
Previous definitions of Threat have included direct or indirect exposure to school, home or neighborhood violence, physical discipline, physical abuse, sexual abuse, and emotional abuse (Lambert et al., Reference Lambert, King, Monahan and McLaughlin2017; Miller et al., Reference Miller, Sheridan, Hanson, McLaughlin, Bates, Lansford and Dodge2018; Sheridan et al., Reference Sheridan, Peverill, Finn and McLaughlin2017). We created a threat dimension using the following 14 items: violent death of a first (2.4%) and second (0.1%) loved one, violent death of a first (14.5%) and second (2.6%) peer, being exposed to war or terror (0.1%), witnessing of life traumatic event (23.8%), victim of physical violence (not abuse) (3.1%), victim of physical abuse by a family member (7.3%), being held in captivity (0.9%), victim of sexual abuse (10.9%), rape (1.2%), sexual coercion (4.3%), witnessing parental violence (8.1%) and living in a chronically unsafe environment due to violence (7.8%).
Previous definitions of Deprivation have focused on deprivation of cognitive, social, and material resources (Lambert et al., Reference Lambert, King, Monahan and McLaughlin2017; Miller et al., Reference Miller, Sheridan, Hanson, McLaughlin, Bates, Lansford and Dodge2018; Sheridan et al., Reference Sheridan, Peverill, Finn and McLaughlin2017). Due to the items assessed, we have focused on material deprivation only. This dimension includes the following items: an interviewer-rated item from the Child and Adolescent Functional Assessment Scale on whether the child’s basic needs were met for food, housing, clothing, medical attention, or neighborhood safety (15.4%), a measure of whether or not the reported household income was below the federal poverty level for the family size (35%), and a parent-report item about lack of general medical care insurance (61%).
LH dimensions
Previous definitions of Unpredictability included paternal transitions (e.g., mother’s partner was no longer living in home), household moves, and parental employment transitions (Belsky et al., Reference Belsky, Schlomer and Ellis2012). We created an unpredictability dimension using the following four items: parental transitions (dichotomous, endorsed if change of parent) (27.4%), household moves (dichotomous, endorsed if moved 4+ times) (8.7%), reduced standard of living (family’s standard of living was reduced noticeably in the last 3 months, as evidenced, for example by inability to pay bills, need to sell things, need to move) (14.7%), and change of school without friends (17.1%).
Loss
Due to the broadness in how it has been defined and the heterogeneity in how it has been operationalized, we propose to study harshness via the already described dimensions of threat and material deprivation along with a dimension of loss (Brown et al., Reference Brown, Harris and Copeland1977; Luecken, Reference Luecken, Stroebe, Hansson, Schut and Stroebe2008; Pham et al., Reference Pham, Porta, Biernesser, Walker Payne, Iyengar, Melhem and Brent2018). We created a loss dimension using the following items: termination of a pregnancy (1.2%), death of a first (8%) and second (0.8%) loved one, death of a first (17.6%), and second peer (4.1%), loss of a best friend via a move (12.8%), break up with best friend (9.6%) and break up with romantic partner (15.8%) and parental separation or divorce (9.5%). Items related to separation from friends and romantic breakups were included based upon previous work about the similar effects of these events on psychopathology as observed with other loss events (Brown et al., Reference Brown, Harris and Hepworth1995; Monroe et al., Reference Monroe, Rohde, Seeley and Lewinsohn1999).
Other adversities
Other early adversities that were not otherwise included in one of the dimensions described above were summed in a separate Other Adversity scale. These included the following events: being involved in a serious accident (11.6%), exposed to a noxious agent (3.3%), serious physical illness (11%), natural disaster (13.4%), and fire (5.9%) as well as maternal self-rated depression (present if score was above 8 on the Mood and Feelings Questionnaire; Angold et al., Reference Angold, Costello, Messer and Pickles1995) (16.1%), parent self-report of criminal arrest (5.1%), and parents substance problems (16.1%).
Finally, a Cumulative Adversity measure was derived by summing the four adversity dimensions with the other adversity scale.
Adult outcomes
All outcomes except where noted (e.g., official criminal records) were assessed using the young adult psychiatric assessment (Angold et al., Reference Angold, Cox, Prendergast, Rutter, Simonoff, Costello and Ascher1999) an upward extension of the CAPA interview administered to the participants at ages 19, 21, 25, and 30. The assessment of adults resembled that of childhood but with only self-report and not parent reports.
Psychiatric outcomes
For psychiatric symptoms, the CAPA focuses on the 3 months immediately preceding the interview to minimize recall bias. Scoring programs written in SAS statistical software (SAS Institute Inc) combine information about the date of onset, duration, and intensity of each symptom to create DSM diagnoses. Test−retest reliability and validity of the young adult psychiatric assessment diagnoses are similar to other psychiatric interviews (Angold et al., Reference Angold, Cox, Prendergast, Rutter, Simonoff, Costello and Ascher1999). Psychiatric disorders assessed included Anxiety disorders, Depressive disorder, Alcohol Use Disorder, and Cannabis Use Disorder. Psychosis and bipolar disorder were not included in analyses owing to very low prevalence (<1%) in the community. The participant was positive for diagnosis if criteria were met at any adult observation.
Functional outcomes
Scales were derived to provide a broad profile of adult functioning across four domains: health problems, economic (financial and/or educational) problems, conduct, problems, and social problems. These scales were summed from dichotomous indictors in each domain. In some cases the indicators were positive if reported at any point in adulthood; in other cases (e.g., educational attainment) the last observation was used to determine status.
Health problems. Health problems included being diagnosed with a serious illness, or being in a serious accident, having a sexually transmitted disease, obesity (>30 kg/m2), DSM-IV psychiatric diagnosis (anxiety, depressive, and antisocial personality disorder), self-reported perceived poor health, high illness contagion risk, and slow illness recovery.
Economic problems. Economic (financial/educational) problems included being impoverished (based on income and family size), high school dropout and completion of any college education, being dismissed or fired from a job and quitting a job without economic preparations, and extended unemployment as well as failing to honor debts or economic obligations, being a poor manager of one’s finances, and no health insurance.
Conduct problems. Conduct problems included official felony charges, self-reported police contact, often lying to others, frequent physical fighting, breaking into another home/business/property, begin spiteful/vindictive, harassment, mistreatment of one’s children, setting fires, life-threatening hobbies, drunk driving, gambling and one-time sexual encounters with strangers.
Social problems. Social problems included marital, parenthood, and divorce status, poor quality of the participant’s relationship with their parents, spouse/significant other, and friends, any violence in a primary relationship, no best friend or confidante, and problems making or keeping friends.
Theory proximal outcomes
We define theory proximal outcomes as outcomes closely related to the neural pathways or reproductive successes theorized and/or measured in previous empirical works of DMAP and LH.
DMAP-proximal. In previous works, DMAP researchers have operationalized cognitive functioning as language ability, memory, attention, and learning (Bos et al., Reference Bos, Fox, Zeanah and Nelson Iii2009; Machlin et al., Reference Machlin, Miller, Snyder, McLaughlin and Sheridan2019; Pollak et al., Reference Pollak, Nelson, Schlaak, Roeber, Wewerka, Wiik and Gunnar2010). Herein, we operationalize cognitive functioning as estimated full IQ. A subsample of participants was administered the Wechsler Abbreviated Scale of Intelligence-Second Edition at age 25 (Wechsler, Reference Wechsler2011).
LH proximal. Ellis et al. (Reference Ellis, Figueredo, Brumbach and Schlomer2009) theorized that Harshness and Unpredictability contribute to LH adaptive biological strategies, suggesting that earlier age of birthing a child as a proximal outcome for faster LH strategy. In their empirical work, Belsky et al. (Reference Belsky, Schlomer and Ellis2012) use the outcome of number of sexual partners at age 15. Herein, we use both the suggested and empirically supported outcomes of number of sexual partners (at age 16), and the age at which participants who are parents had their first biological child (aggregated into groups of less than 18, 19–24, 25–30, and not a parent by age 30).
Statistical models
Each participant was assigned a sampling weight inversely proportional to their probability of selection. Consistent with common conventions, all percentages provided in the results are weighted and sample sizes are unweighted in descriptive tables.
Child sex and race/ethnicity (White vs. Minority) were included as covariates in all regression models. First, a series of models tested associations of each adversity dimension with each outcome individually. If significant in the individual model, the dimension was entered into a multivariable model testing all significance dimensions for each adult outcome simultaneously. Psychiatric diagnoses were run using logistic regression models, and all other outcomes were run using linear regression models yielding 77 hypothesized models total. Findings were considered statistically significant at 2-sided p < .026 using the Benjamini & Hochberg (Reference Benjamini and Hochberg1995) FDR method (referenced as BH-FDR in subsequent literature (Narum, Reference Narum2006; White et al., Reference White, van der Ende and Nichols2019). The BH-FDR method has been demonstrated to minimize both false positives and false negatives, while still controlling the false detection rate. This method shows similar minimization of false positives as Bonferroni, but has a lower false-negative rate (White et al., Reference White, van der Ende and Nichols2019).
Table 1. Frequencies of childhood adversity dimensions between ages 11–16

Note. All continuous variables winsorized at >96%.
Table 2. Correlation matrix of childhood adversity

Note. Bold indicates significance at p < .001.
Table 3. Descriptive information of outcome data

Note. W = Winsorized at 96%.
Results
Descriptive information
About half of all participants experienced Threat (49.6%), Unpredictability (43.7%), and Loss (51.9%), whereas more participants experienced Material Deprivation (67.9%) and Other Adversity (75.6%) (see Table 1). Intercorrelations among dimensions ranged from weak to moderate (see Table 2). Altogether, adversity exposure was very common (see Figure 1) with 91.4% of participants experiencing at least 1 adversity (M = 4.54, SD = 2.85). All childhood adversity dimension means significantly differed by gender (see Figure 2) such that females experienced more Threat, Unpredictability, and Loss and males experienced more Deprivation and Other Adversity. Three adversity dimension means significantly differed by race/ethnicity (see Figure 3) such that persons with minoritized race/ethnicity identities experienced more Threat, Deprivation, and Unpredictability, but similar levels of Loss or Other Adversity. Descriptive information for all outcomes is provided in Table 3.

Figure 1. Histogram of cumulative adversity.

Figure 2. Mean differences of number of child adversity events by type by race/ethnicity (minority vs white) with standard error. *indicate significant difference.

Figure 3. Mean differences of number of child adversity events by type by sex (male/female) with standard error. *indicate significant difference.
Table 4. Simultaneous logistic regression models including childhood adversity dimensions and cumulative adversity with psychiatric outcomes

Significant at p < 0.05.
Table 5. Simultaneous linear regression models including childhood adversity dimensions and cumulative adversity with functional outcomes

Significant at p < 0.05.
Table 6. Simultaneous linear regression models including childhood adversity dimensions and cumulative adversity with DMAP and LH proximal outcomes

Significant at p < 0.05.
Table 7. Summary table of significant associations among childhood adversity types and cumulative adversity with outcomes
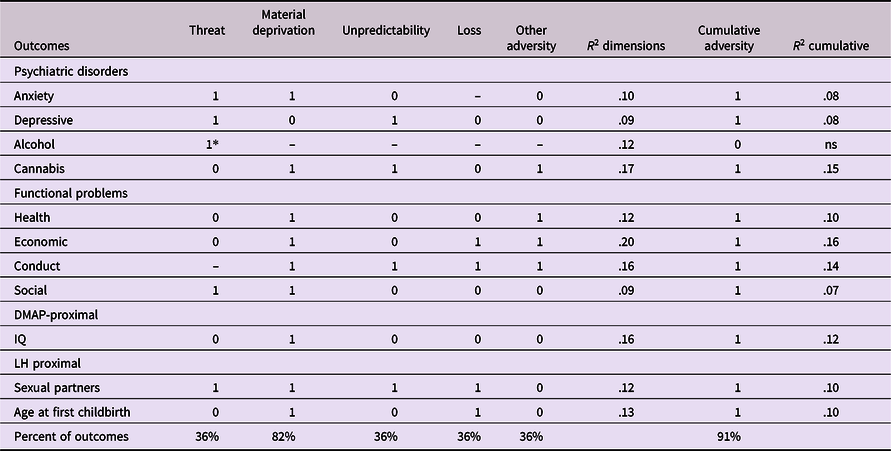
Note. * = unexpected direction of association.
Regression model analyses
Results of multivariable model testing all significance dimensions for each adult outcome simultaneously are presented in Tables 4–6. Significant associations of childhood adversity dimensions and outcomes are summarized in Table 7 indicated with 1’s (significant) and 0’s (nonsignificant).
DMAP dimensions
Material Deprivation and Threat were significantly associated with 82% and 36% of the 11 outcomes, respectively. In terms of proximal outcomes, as hypothesized in the DMAP theory, Material Deprivation, but not Threat, Unpredictability, Loss, or other adversities was associated with IQ in early adulthood. In terms of distal outcomes, Deprivation was associated with only 2 of 4 psychiatric disorders (Anxiety and Cannabis Use) but was associated with 4 of 4 functional outcomes (Health, Economic, Conduct, and Social) and both LH outcomes (i.e., number of sexual partners at 16, and Age at First Childbirth). Threat was associated with 2 of 4 psychiatric disorders in the expected direction (Anxiety, and Depression) and 2 of 4 functional outcomes (Conduct and Social). It should be noted that Threat was the only dimension associated with Alcohol Use disorder, but unexpectedly less Threat was linked to higher likelihood of the disorder (denoted by an * in Table 7). Threat was associated with one LH outcome (number of sexual partners at 16, but not Age at First Childbirth.
LH dimensions
Unpredictability was associated with 4 of the 11 outcomes (36%). Consistent with the LH theory, Unpredictability was associated with number of sexual partners at 16. However, Unpredictability was not associated with Age at First Childbirth. Unpredictability was associated with 2 of 4 psychiatric disorders (Depressive and Cannabis Use) and 1 of 4 functional outcomes (Conduct). Unpredictability was not associated with IQ.
Loss, one operationalization of Harshness, was also associated with 4 of the 11 outcomes (36%). Consistent with the LH theory, Loss was associated with both LH outcomes. Loss was associated with 0 of 4 psychiatric disorders, but 2 of 4 functional outcomes (Economic and Conduct). Loss was not associated with IQ.
Other adversity
Other Adversity was also associated with 4 of 11 outcomes (36%). Specifically, it was associated with 1 of 4 psychiatric disorders (Cannabis Use) and 3 of 4 functional outcomes (Health, Economic and Conduct). Other Adversity was not associated with any DMAP or LH proximal outcomes.
Cumulative adversity
Cumulative Adversity was associated with all outcomes with the exception of Alcohol Use Disorder (91%). Cumulative adversity univariable models predicted about 2% more variance (R 2 = .07–.16) than multivariable models (R 2 = .09–.20) across outcomes.
Discussion
This analysis had three broad aims: (1) to conduct the broadest test yet of the long-term impact of multiple childhood adversity dimensions on adult health and functioning; (2) to test for differential impact of individual childhood adversity dimensions on proximal and distal outcomes; and (3) to compare the long-term prediction of individual adversity dimension approach to a cumulative adversity approach. To meet these aims, the study combined four adversity dimensions measured repeatedly in childhood and adolescence with a broad range of psychiatric and functional outcomes measures up to two decades later in adulthood. Overall, the pattern of findings supports and extends previous work suggesting the following: (1) consistent evidence of long-term associations of all adversity dimensions with adult psychiatric and functional outcomes; (2) evidence of differential impact of dimensions of adversity exposure on proximal outcomes; and (3) similar levels of prediction between the best set of individual adversity scales and a single cumulative adversity measure when considering distal outcomes. Each of these findings is discussed in more detail below along with study limitations and conclusions.
Long-term impact of early adversity
Every child adversity dimension was associated with at least two adult outcomes, and most of the 11 outcomes (except Alcohol Use Disorder, IQ, and Health) were predicted by at least two of the four adversity dimensions when they were simultaneously controlled in a single model. When all dimensions were considered together, Cumulative risk, measured in childhood was associated with all but one adult outcome (Alcohol Use Disorder). This symmetry suggests that multiple dimensions of childhood adversity have lasting effects on adult outcomes. This pattern of findings is consistent with results from other longitudinal studies which increasingly suggest no upper limit on the period of time across which an adversity-outcome association may be observed (Raposo et al., Reference Raposo, Mackenzie, Henriksen and Afifi2014). This is concerning as this study and others confirm that the experience of childhood adversity is not at all rare (McLaughlin et al., Reference McLaughlin, Greif Green, Gruber, Sampson, Zaslavsky and Kessler2012), but relatively common with almost half this sample having between 1 and 4 such exposures. This is a concern only insofar as such adversities are causal risk factors for the adult outcomes rather than proxy markers of other causal factors. On that point, this study is limited by the observational design and cannot weigh in. However, efforts to evaluate effects of early individual adversities like abuse, neglect, and peer bullying using designs that allow for causal inferences, however, have found support for causal effects (Dinwiddie et al., Reference Dinwiddie, Heath, Dunne, Bucholz, Madden, Slutske and Martin2000; Humphreys et al., Reference Humphreys, McGoron, Sheridan, McLaughlin, Fox, Nelson and Zeanah2015; Schaefer et al., Reference Schaefer, Moffitt, Arseneault, Danese, Fisher, Houts and Caspi2018). Adversity exposures that occur early in development are relatively common and demonstrate causal effects on multiple long-term outcomes have the potential to have the greatest public health burden across the life span. Efforts to protect children from these experiences are important to ensuring the ongoing health and well-being of the population across a wide range of outcomes in to adulthood.
Differential impact
The hypothesis that different adversities or dimensions of adversity might vary in their effect on later outcomes has a long history in developmental psychopathology. However, recent neurodevelopmental and evolutionary theories offer strong theoretical rationales to support such claims (Sheridan & McLaughlin, Reference Sheridan and McLaughlin2014). In addition, these more recent theories have re-conceptualized the specificity/cumulative risk argument in terms of dimensions whereby theoretically related adversities are expected to accumulate to impact some outcomes (e.g., McLaughlin et al., Reference McLaughlin, Sheridan, Humphreys, Belsky and Ellis2021). Data from this study is consistent with many of these claims.
Consistent with the DMAP theory, Material Deprivation was the only dimension associated with the predicted proximal outcome: young adult IQ. For distal outcomes, Material Deprivation showed the broadest pattern of associations. In all, it was associated with 9 of 11 outcomes including adult anxiety and cannabis use disorders as well as all functional outcomes (Health, Economic, Conduct, and Social). This is consistent with previous findings that IQ is a strong predictor of many adult functional outcomes (Nisbett et al., Reference Nisbett, Aronson, Blair, Dickens, Flynn, Halpern and Turkheimer2012) and is a potent protective factor against the emergence of psychopathology (Garmezy et al., Reference Garmezy, Masten and Tellegen1984). Indeed, there are many reasons why Material Deprivation exhibited this broad impact but one reason, predicted by the DMAP theory, is that one pathway through which Material Deprivation increases risk in many other domains is by an impact on cognition, here measured by IQ. None of the predicted proximal outcomes for the Threat dimension were measured in this study; however, Threat had a specific impact on adult emotional functioning as the only dimension associated with both adult Anxiety and Depressive disorders as well as two functional outcomes (Conduct and Social). This pattern of results is consistent with the DMAP theory whereby the impact of threat is expected to be on emotional reactivity and the sequala of heightened emotional reactivity.
The LH model focuses on impact of adversity dimensions on reproductive strategies in adolescence (Belsky et al., Reference Belsky, Schlomer and Ellis2012). Here, Unpredictability was associated with sexual partners at 16, replicating Belsky et al. (Reference Belsky, Schlomer and Ellis2012) prior work using a similar Unpredictability measure. Unpredictability was also informative about adult health and functioning showing associations with two psychiatric disorders and one functional outcome. This connection with adult conduct and criminality specifically, replicates earlier work showing associations between early Unpredictability and young adult aggression and criminality (Simpson et al., Reference Simpson, Griskevicius, Kuo, Sung and Collins2012). Examples of Harshness measures range from neighborhood violence to poverty and the funerals attended, measures that cross Threat, Deprivation, and Loss dimensions. In this sense, harshness is the most general construct of negative early experiences. Consistent with the LH theory, we observed that the Loss and Deprivation dimensions were associated number of sexual partners and age at first birth, and Threat with number of sexual partners. Interestingly, in a recent meta-analysis Deprivation specifically, was not associated with accelerated LH strategies in childhood as measured by early-onset puberty (Colich et al., Reference Colich, Rosen, Williams and McLaughlin2020). It is possible that the difference in assessing LH strategies or the age at which these outcomes were assessed explains the differences in these findings. Together, these findings suggest an longitudinal association between LH dimensions and reproductive strategies, although conclusions about specificity are somewhat limited in this case because all the dimensions of adversity measured in this study except the "other adversities" category have been posited to be examples of Harshness or Unpredictability in the existing literature (Ellis et al., Reference Ellis, Figueredo, Brumbach and Schlomer2009).
Individual dimensions versus cumulative adversity
The individual dimensions were used to develop multivariable models predicting each of the adult outcomes while excluding dimensions not associated with the outcomes. Such an approach maximizes the potential childhood adversity-adult outcomes associations. These models accounted for between 9% and 20% of the variance in adult psychiatric and functional outcomes despite the decade plus gap between the adversities and the outcomes. In addition, much of the specificity of effect theorized by the authors of these approaches was realized. Every case where a proximal outcome could be tested in the current data set (Deprivation, Harshness, Unpredictability) the proximal outcome was associated as predicted in the LH and DMAP model. At the same time, these models performed only slightly better than the single cumulative adversity scale (which sums all childhood adversities and weighted them equally regardless of their individual association with the outcome) when predicting distal outcomes (e.g., psychiatric disorders or adult functional outcomes). The exception to this rule was in the case of alcohol use disorder where the cumulative adversity measure was not statistically significant. If the goal is simply to estimate one’s relative risk for adult outcomes, these findings strongly support the use of the parsimonious cumulative adversity scale over a focus on individual adversity dimensions or profiles. However, if a mechanistic understanding is sought, where pathways linking childhood adversity to adult outcomes are identified, these findings support taking a dimensional approach.
A broader point, however, is that both approaches accounted for significant variation in adult outcomes and, in every case except IQ, the final multivariable model predicting a given adult outcome had at least two significant childhood adversity dimension and often more. Many research studies continue to focus on individual risk experiences (e.g., divorce, maltreatment) in the absence of information about the totality of the child’s adverse experiences. The findings from this work and many other studies suggest that adversities (and the dimensions they index) accumulate to predict adult psychiatric and functional outcomes. The relative importance of any given adversity may be the degree to which it reduces resources the child has available to cope with another adversity.
Limitations
The study is not without caveats. Many studies have examined core dimensions of child adversity within a sensitive window in early childhood, often 0–5 years and also 5–7 years (e.g., Belsky et al., Reference Belsky, Steinberg and Draper1991). Our study examined child adversity dimensions during middle childhood and early adolescence 9–16 years, inclusive of childhood adversity since birth. This age range expands outside solely “early childhood” which could impact specificity and strength of associations with outcomes due to sensitivity window and/or recency effects (Simpson et al., Reference Simpson, Griskevicius, Kuo, Sung and Collins2012). Additionally, this study did not conduct mediation analyses as prior theory work has done (Miller et al., Reference Miller, Machlin, McLaughlin and Sheridan2021), to estimate the pathways through which early adversity affects distal outcomes across development. In examining proximal outcomes, we have attempted to replicate prior empirical works; however, across previous studies operationalizations of specific dimensions have often varied. For instance, deprivation has been operationalized as poverty, as in this study, but is more commonly operationalized as a combination of caregiver neglect, low parental education, and low number of books in the home (Lambert et al., Reference Lambert, King, Monahan and McLaughlin2017; Machlin et al., Reference Machlin, Miller, Snyder, McLaughlin and Sheridan2019; Miller et al., Reference Miller, Sheridan, Hanson, McLaughlin, Bates, Lansford and Dodge2018; Rosen et al., Reference Rosen, Sheridan, Sambrook, Meltzoff and McLaughlin2018; Sheridan et al., Reference Sheridan, Peverill, Finn and McLaughlin2017). Such differences may have important effects on association with outcome. The challenge of specifying how to define deprivation and threat is specifically addressed in Berman et al., this issue. Finally, this sample has a number of useful features for studying these questions by combining a community-representative design with broad assessment of early risk and repeated follow-ups both within childhood and into adulthood. At the same time, this study is representative of a mixed urban-rural area in the Southeast US, not of the US population and the study was not designed to assess these particular dimensions of adversity.
Conclusion
Our findings show long-term associations of different dimensions of adversity with a broad range of adult psychiatric and functional outcomes decades later. One of the central insights of developmental psychopathology is that adversity and its dimensions are both relatively common and commonly comorbid. Here, about half of the sample had been exposed to at least three or more such adversity dimensions. At the same time, the paradox of these results was that while multiple risk dimensions were associated with similar distal outcomes there was also evidence that dimensions these may act via distinct proximal pathways.
Funding statement
The work presented here was supported by the National Institute of Mental Health (MH117559), the National Institute on Drug Abuse (DA023026), the National Institute of Child Health and Development (HD093651) and the National Institute of Aging (AG072459). Also supported by the National Institute of Mental Health Career Development Award (Dr. McGinnis: MH123031-01A1).
Conflicts of interest
None.










