


Exposure to maltreatment in childhood is a potent risk factor for psychopathology that accounts for a substantial proportion of mental disorders in the population (Green et al., Reference Green, McLaughlin, Berglund, Gruber, Sampson, Zaslavsky and Kessler2010; Kessler et al., Reference Kessler, McLaughlin, Green, Gruber, Sampson, Zaslavsky and Williams2010; McLaughlin et al., Reference McLaughlin, Green, Gruber, Sampson, Zaslavsky and Kessler2012). US population-based studies estimate that approximately between 1 in 10 and 1 in 4 children will experience physical, sexual, or emotional abuse or exposure to some other form of violence within the family by the time they reach adulthood (Finkelhor, Shattuck, Turner, & Hamby, Reference Finkelhor, Shattuck, Turner and Hamby2014; Finkelhor, Turner, Shattuck, & Hamby, Reference Finkelhor, Turner, Shattuck and Hamby2013; McLaughlin et al., Reference McLaughlin, Green, Gruber, Sampson, Zaslavsky and Kessler2012). Exposure to child maltreatment is associated with elevated risk for virtually all forms of psychopathology, including mood, anxiety, disruptive behavior, substance abuse, and psychotic disorders (Cicchetti & Toth, Reference Cicchetti and Toth2005; Green et al., Reference Green, McLaughlin, Berglund, Gruber, Sampson, Zaslavsky and Kessler2010; Kessler et al., Reference Kessler, McLaughlin, Green, Gruber, Sampson, Zaslavsky and Williams2010; McGrath et al., Reference McGrath, Saha, Lim, Aguilar-Gaxiola, Alonso, Andrade and Wojtyniak2017; McLaughlin et al., Reference McLaughlin, Green, Gruber, Sampson, Zaslavsky and Kessler2012; Schaefer et al., Reference Schaefer, Moffitt, Arseneault, Danese, Fisher, Houts and Caspi2018). Identifying mechanisms linking child maltreatment to the onset of psychopathology is critical for developing more effective early interventions. In this paper, we examine relationships between maltreatment and emotion regulation strategies within the framework of a leading conceptual model of emotion regulation. We additionally evaluate whether the associations between maltreatment and emotion regulation strategies vary across development, and test whether emotion dysregulation serves as a mechanism linking maltreatment with transdiagnostic risk for psychopathology.
Emotion Regulation and the Process Model
Emotion regulation has been defined as the “processes responsible for monitoring evaluating and modifying emotional reactions, especially their intensive and temporal features, to accomplish one's goals” (Thompson, Reference Thompson1994). Emotion regulation encompasses a wide range of specific component processes that can occur at different points in the emotion generation process. The process model of emotion regulation (Gross, Reference Gross1998b, Reference Gross and Gross2014; Gross & Thompson, Reference Gross and Levenson2007) is a leading conceptual framework for organizing emotion regulation strategies. This model outlines four temporal stages involved in the generation and expression of an emotional response: (a) an emotional response is triggered by an internal or external situation; (b) attention is allocated to that situation; and (c) an appraisal is generated. An emotional response occurs when a situation is appraised as being relevant to one's goals, and a wide range of (d) responses can occur following that emotional experience.
Emotion regulation can occur at every stage of this process (Gross, Reference Gross1998b, Reference Gross and Gross2014; Gross & Thompson, Reference Gross, Thompson and Gross2007). Individual strategies for emotion regulation can be either adaptive or maladaptive (Aldao & Nolen-Hoeksema, Reference Aldao and Nolen-Hoeksema2010, Reference Aldao and Nolen-Hoeksema2012b) and vary in their efficacy at influencing emotional reactions (Gross, Reference Gross1998a; Gross & John, Reference Gross and John2003; Webb, Miles, & Sheeran, Reference Webb, Miles and Sheeran2012). These strategies generally fall into one of two categories: “antecedent focused” or “response focused.” Antecedent-focused strategies occur before or during the first three stages of the emotion process (situation, attention, and appraisal) and have been shown be effective at modulating the intensity and duration of emotional responses (Gross, Reference Gross1998a; Gross & John, Reference Gross and John2003; Webb et al., Reference Webb, Miles and Sheeran2012). Response-focused strategies, in contrast, occur during the response phase of the emotion regulation model and, paradoxically, may actually increase emotion intensity (Gross, Reference Gross1998a; Gross & Levenson, Reference Gross and Levenson1997; John & Gross, Reference John and Gross2004). For that reason, response-focused strategies are generally considered to be maladaptive (Gross & John, Reference Gross and John2003; Nolen-Hoeksema & Aldao, Reference Nolen-Hoeksema and Aldao2011).
Two common antecedent-focused emotion regulation strategies include cognitive reappraisal and attention deployment. Cognitive reappraisal involves thinking about an emotional situation in a different way in order to alter one's emotional response, and is considered an effective and adaptive form of emotion regulation in most situations (Aldao & Nolen-Hoeksema, Reference Aldao and Nolen-Hoeksema2010, Reference Aldao and Nolen-Hoeksema2012a, Reference Aldao and Nolen-Hoeksema2012b; Gross & John, Reference Gross and John2003; Nolen-Hoeksema & Aldao, Reference Nolen-Hoeksema and Aldao2011; Webb et al., Reference Webb, Miles and Sheeran2012). Attention deployment involves the manipulation of attention either toward or away from an emotional stimulus. Habitual biases toward particular types of emotion-generating stimuli can be considered a rapid, unconscious form of attention deployment (Todd, Cunningham, Anderson, & Thompson, Reference Todd, Cunningham, Anderson and Thompson2012).
Response-focused strategies include expressive suppression and rumination. Expressive suppression involves modulation of the outward expression of emotion. Its efficacy at modulating emotional responses is limited to their expression, however, and both the physiological and subjective experience of emotions is intensified by use of this strategy (Gross, Reference Gross1998a; Gross & Levenson, Reference Gross and Levenson1997). Rumination involves passive, repetitive self-focused thinking about the causes and consequences of distress, while failing to engage in problem solving to alleviate the source of distress (Nolen-Hoeksema & Morrow, Reference Nolen-Hoeksema and Morrow1991; Nolen-Hoeksema, Wisco, & Lyubomirsky, Reference Nolen-Hoeksema, Wisco and Lyubomirsky2008). Experimental evidence suggests that rumination increases negative affect (McLaughlin, Borkovec, & Sibrava, Reference McLaughlin, Borkovec and Sibrava2007), leads to other forms of negative, maladaptive thinking (Lyubomirsky, Caldwell, & Nolen-Hoeksema, Reference Lyubomirsky, Caldwell and Nolen-Hoeksema1998), and reduces engagement in more effective strategies to alleviate negative mood (Lyubomirsky & Nolen-Hoeksema, Reference Lyubomirsky and Nolen-Hoeksema1993).
Development of Emotion Regulation and Reactivity
The utilization of specific emotion regulation strategies and the effectiveness of particular strategies at modulating emotional responses varies from middle childhood through adolescence (Gresham & Gullone, Reference Gresham and Gullone2012; Gullone, Hughes, King, & Tonge, Reference Gullone, Hughes, King and Tonge2010; Silvers et al., Reference Silvers, McRae, Gabrieli, Gross, Remy and Ochsner2012, Reference Silvers, Insel, Powers, Franz, Helion, Martin and Ochsner2017b). Attention biases toward threat are detectable as early as infancy (Lobue & Deloache, Reference Lobue and Deloache2010) and tend to decrease with age from childhood through adolescence (Lonigan & Vasey, Reference Lonigan and Vasey2009; Reinholdt-Dunne, Mogg, Esbjorn, & Bradley, Reference Reinholdt-Dunne, Mogg, Esbjorn and Bradley2012). This developmental shift may indicate an increasing capacity to effortfully direct attention away from threat as an emotion regulation strategy (Morales, Fu, & Pérez-Edgar, Reference Morales, Fu and Pérez-Edgar2016). The strength of the association between anxiety and attention biases toward threat increases with age (Dudeney, Sharpe, & Hunt, Reference Dudeney, Sharpe and Hunt2015), suggesting that a failure to develop this emotion regulatory strategy may contribute to psychopathology. The use of cognitive reappraisal has been found to remain relatively consistent across development (Gresham & Gullone, Reference Gresham and Gullone2012; Gullone et al., Reference Gullone, Hughes, King and Tonge2010), but the effectiveness of cognitive reappraisal use at reducing negative affect increases from middle childhood through adolescence (McRae et al., Reference McRae, Gross, Weber, Robertson, Sokol-Hessner, Ray and Ochsner2012; Silvers et al., Reference Silvers, McRae, Gabrieli, Gross, Remy and Ochsner2012, Reference Silvers, Insel, Powers, Franz, Helion, Martin and Ochsner2017a). Use of expressive suppression decreases from childhood to middle adolescence, then remains at the same level into adulthood (Gresham & Gullone, Reference Gresham and Gullone2012; Gullone et al., Reference Gullone, Hughes, King and Tonge2010). The observed developmental trajectories of rumination across middle childhood and adolescence are inconsistent across studies (Abela, Hankin, Sheshko, Fishman, & Stolow, Reference Abela, Hankin, Sheshko, Fishman and Stolow2012; Hankin, Reference Hankin2008; Jose & Brown, Reference Jose and Brown2008), but individual differences in the tendency to engage in rumination are quite stable (Ziegert & Kistner, Reference Ziegert and Kistner2002), bolstered by reciprocal relations between rumination and psychopathology over time (Nolen-Hoeksema, Stice, Wade, & Bohon, Reference Nolen-Hoeksema, Stice, Wade and Bohon2007).
The continued development of emotion regulation tendencies and competency across adolescence corresponds with a concurrent peak in emotional reactivity, as indicated by greater emotional volatility and intensity compared to childhood and adulthood (Gunnar, Wewerka, Frenn, Long, & Griggs, Reference Gunnar, Wewerka, Frenn, Long and Griggs2009; Guyer, Silk, & Nelson, Reference Guyer, Silk and Nelson2016; Larson, Moneta, Richards, & Wilson, Reference Larson, Moneta, Richards and Wilson2002; Stroud et al., Reference Stroud, Foster, Papandonatos, Handwerger, Granger, Kivlighan and Niaura2009). This peak in emotional reactivity in adolescence, while systems of cognitive control and emotion regulation are still developing, is the basis of influential models explaining the rise in risk-taking behaviors and the emergence of psychopathology in adolescence (Ernst, Pine, & Hardin, Reference Ernst, Pine and Hardin2006; Shulman et al., Reference Shulman, Smith, Silva, Icenogle, Duell, Chein and Steinberg2016; Somerville, Jones, & Casey, Reference Somerville, Jones and Casey2010).
Maltreatment and Emotion Dysregulation
Emotion dysregulation has been conceptualized as a key mechanism linking child maltreatment with multiple forms of psychopathology (Beauchaine, Reference Beauchaine2015; Heleniak, Jenness, Vander Stoep, McCauley, & McLaughlin, Reference Heleniak, Jenness, Vander Stoep, McCauley and McLaughlin2016; Kim & Cicchetti, Reference Kim and Cicchetti2010; Maughan & Cicchetti, Reference Maughan and Cicchetti2002; McLaughlin & Lambert, Reference McLaughlin and Lambert2017). Emotion dysregulation is a pattern of emotion regulation that interferes with an individual's goals (Beauchaine, Reference Beauchaine2015; Cole, Hall, & Hajal, Reference Cole, Hall, Hajal, Beauchaine and Hinshaw2017), either because of more habitual use of maladaptive emotion regulation strategies or because of failure to effectively implement adaptive emotion regulation strategies. Because emotion dysregulation involves the presence instead of the absence of problematic behavior or experiences, it may be easier to identify and observe than effective emotion regulation (Beauchaine, Reference Beauchaine2015). Maltreated children may lack adaptive emotion regulation skills because rather than scaffolding these skills, caregivers may model maladaptive strategies and punish emotional expressions (Cicchetti, Ackerman, & Izard, Reference Cicchetti, Ackerman and Izard1995; Kim & Cicchetti, Reference Kim and Cicchetti2010). Further, in an environment characterized by high levels of threat, regulatory patterns that promote vigilance to potential threats may contribute to immediate self-preservation, with trade-offs for adaptive functioning in other contexts (Frankenhuis & Del Giudice, Reference Frankenhuis and Del Giudice2012).
Child maltreatment has been associated with emotion dysregulation, as indicated by parent reports (Kim & Cicchetti, Reference Kim and Cicchetti2010) and behavioral observations (Maughan & Cicchetti, Reference Maughan and Cicchetti2002; Shields & Cicchetti, Reference Shields and Cicchetti1997) in prior research. Moreover, child maltreatment has been linked to differences in many specific forms of emotion regulation (Heleniak et al., Reference Heleniak, Jenness, Vander Stoep, McCauley and McLaughlin2016; McLaughlin & Lambert, Reference McLaughlin and Lambert2017). Critically, although the use and efficacy of emotion regulatory strategies varies across development (Dudeney et al., Reference Dudeney, Sharpe and Hunt2015; Gullone et al., Reference Gullone, Hughes, King and Tonge2010; Silvers et al., Reference Silvers, McRae, Gabrieli, Gross, Remy and Ochsner2012), few studies have examined whether the association of child maltreatment with specific types of emotion regulation strategies varies by age.
Child maltreatment, particularly exposure to abuse, is associated with abnormal attention deployment to threatening stimuli (e.g., angry faces). Children who have experienced abuse are more perceptually sensitive to detecting anger in faces (Pollak, Cicchetti, Hornung, & Reed, Reference Pollak, Cicchetti, Hornung and Reed2000; Pollak & Kistler, Reference Pollak and Kistler2002; Pollak & Sinha, Reference Pollak and Sinha2002) and demonstrate patterns of neural activity that suggest greater attentional engagement toward and difficulty disengaging attention from angry faces (Pollak, Reference Pollak2003; Pollak & Tolley-Schell, Reference Pollak and Tolley-Schell2003; Shackman, Shackman, & Pollak, Reference Shackman, Shackman and Pollak2007). Consistent with this increased sensitivity and attention to threat, children, adolescents, and young adults exposed to abuse and other forms of violence exhibit greater attention bias toward angry faces than those without a history of violence exposure (Briggs-Gowan et al., Reference Briggs-Gowan, Pollak, Grasso, Voss, Mian, Zobel and Pine2015; Miller, Reference Miller2015; Pollak & Tolley-Schell, Reference Pollak and Tolley-Schell2003; Swartz, Graham-Bermann, Mogg, Bradley, & Monk, Reference Swartz, Graham-Bermann, Mogg, Bradley and Monk2011). However, several studies have also documented associations between maltreatment and attention biases away from threat in middle childhood and early adolescence (Kelly et al., Reference Kelly, Viding, Puetz, Palmer, Mechelli, Pingault and McCrory2015; Pine et al., Reference Pine, Mogg, Bradley, Montgomery, Monk, McClure and Kaufman2005), suggesting avoidance of threat cues among maltreated children in this age range. This may be indicative of age-specific engagement of attentional avoidance as an emotion regulation strategy among maltreated youth during the transition to adolescence.
To our knowledge, no published studies have investigated the relation between child maltreatment and habitual use of cognitive reappraisal. However, in a neuroimaging study in which participants were trained to use reappraisal to downregulate emotional reactivity to emotional stimuli, reappraisal efficacy based on self-reported affect did not differ between maltreated and control participants. However, maltreated participants engaged prefrontal cortex regions associated with cognitive control to a greater degree than controls during cognitive reappraisal, perhaps indicating greater regulatory effort required to decrease negative affect (McLaughlin, Peverill, Gold, Alves, & Sheridan, Reference McLaughlin, Peverill, Gold, Alves and Sheridan2015).
Greater effort might be required to effectively modulate negative emotions among maltreated children, in part, because they experience emotions more intensely than their nonmaltreated peers. Maltreatment has been consistently associated with heightened emotional reactivity, as indicated by self-reported reactivity to stress among adolescents and adults exposed to child maltreatment (Glaser, van Os, Portegijs, & Myin-Germeys, Reference Glaser, van Os, Portegijs and Myin-Germeys2006; Heleniak et al., Reference Heleniak, Jenness, Vander Stoep, McCauley and McLaughlin2016; McLaughlin et al., Reference McLaughlin, Kubzansky, Dunn, Waldinger, Vaillant and Koenen2010). In addition, maltreatment is associated with greater reactivity to negative stimuli in brain regions known to respond to emotional salience, including the amygdala (Hein & Monk, Reference Hein and Monk2017; McCrory et al., Reference McCrory, De Brito, Sebastian, Mechelli, Bird, Kelly and Viding2011; McLaughlin et al., Reference McLaughlin, Peverill, Gold, Alves and Sheridan2015; Viding et al., Reference Viding, Sebastian, Dadds, Lockwood, Cecil, De Brito and McCrory2012). Thus, maltreated children and adolescents experiencing more intense emotions may both contribute to and result from difficulties with emotion regulation.
Response-focused emotion regulation strategies have also been associated with child maltreatment. Parenting practices characterized by low monitoring, inconsistent discipline, and corporal punishment are associated with greater use of expressive suppression in children (Balan, Dobrean, Roman, & Balazsi, Reference Balan, Dobrean, Roman and Balazsi2017). Exposure to multiple types of stressors in development, including maltreatment, is associated with greater propensity to engage in rumination (Conway, Mendelson, Giannopoulos, Csank, & Holm, Reference Conway, Mendelson, Giannopoulos, Csank and Holm2004; Heleniak et al., Reference Heleniak, Jenness, Vander Stoep, McCauley and McLaughlin2016; LeMoult et al., Reference LeMoult, Humphreys, King, Colich, Price, Ordaz and Gotlib2018; McLaughlin & Hatzenbuehler, Reference McLaughlin and Hatzenbuehler2009; Michl, McLaughlin, Shepherd, & Nolen-Hoeksema, Reference Michl, McLaughlin, Shepherd and Nolen-Hoeksema2013). Children and adolescents exposed to maltreatment may attempt to suppress intrusive and intense negative emotions, and, when unsuccessful, dwell on those feelings, thereby increasing their duration. Taken together, these findings suggest that maltreatment exposure may interfere with children and adolescents’ ability to employ adaptive, antecedent-focused emotion regulation strategies, while increasing their emotional reactivity and tendency to utilize maladaptive, response-focused strategies. These specific manifestations of emotion dysregulation are likely to be a key pathway explaining increased risk for psychopathology following child maltreatment.
Emotion Dysregulation and Psychopathology
Emotion dysregulation is a transdiagnostic mechanism contributing to virtually all common types of psychopathology in adults and adolescents (Aldao, Nolen-Hoeksema, & Schweizer, Reference Aldao, Nolen-Hoeksema and Schweizer2010; Burns, Jackson, & Harding, Reference Burns, Jackson and Harding2010; O'Mahen, Karl, Moberly, & Fedock, Reference O'Mahen, Karl, Moberly and Fedock2015) as well as comorbidity across different forms of psychopathology (McLaughlin, Aldao, Wisco, & Hilt, Reference McLaughlin, Aldao, Wisco and Hilt2014; McLaughlin & Nolen-Hoeksema, Reference McLaughlin and Nolen-Hoeksema2011; Messman-Moore & Bhuptani, Reference Messman-Moore and Bhuptani2017). Emotion dysregulation resulting from early adversity is thought to exacerbate traitlike vulnerabilities, such as impulsivity or behavioral inhibition, leading to more severe manifestations of psychopathology symptoms transdiagnostically (Beauchaine, Reference Beauchaine2015). Emotion dysregulation has been found to mediate associations between maltreatment and several specific types of psychopathology, including depression (O'Mahen et al., Reference O'Mahen, Karl, Moberly and Fedock2015), self-harm (Peh et al., Reference Peh, Shahwan, Fauziana, Mahesh, Sambasivam, Zhang and Subramaniam2017), posttraumatic stress disorder (PTSD; Burns et al., Reference Burns, Jackson and Harding2010), and comorbid substance use, eating disorders, and borderline personality disorder among those with PTSD (Messman-Moore & Bhuptani, Reference Messman-Moore and Bhuptani2017). Given these associations, it is likely that emotion dysregulation represents a transdiagnostic mechanism that contributes to elevated risk for many forms of psychopathology following exposure to child maltreatment (Beauchaine & Zisner, Reference Beauchaine and Zisner2017; Carver, Johnson, & Timpano, Reference Carver, Johnson and Timpano2017).
One approach to capturing the nonspecific relationship between emotion dysregulation and psychopathology involves the use of a hierarchical measure of general psychopathology labeled the “p factor.” Conceptually similar to the “g factor” of general intelligence, “p” captures shared liability to common mental disorders across the internalizing and externalizing psychiatric spectra and predicts general life impairment, including educational attainment, employment, social service use, and criminal activity (Caspi et al., Reference Caspi, Houts, Belsky, Goldman-Mellor, Harrington, Israel and Moffitt2014; Lahey et al., Reference Lahey, Applegate, Hakes, Zald, Hariri and Rathouz2012; Lahey, Krueger, Rathouz, Waldman, & Zald, Reference Lahey, Krueger, Rathouz, Waldman and Zald2017; Patalay et al., Reference Patalay, Fonagy, Deighton, Belsky, Vostanis and Wolpert2015). Since its first presentation in initial reports, “p” has been computed with similar structure and correlates in studies of children, adolescents, and adults; across studies from many different parts of the world; and across studies that assess psychiatric symptoms using different measures, including self-reports, parent reports, and teacher reports (Caspi et al., Reference Caspi, Houts, Belsky, Goldman-Mellor, Harrington, Israel and Moffitt2014; Castellanos-Ryan et al., Reference Castellanos-Ryan, Briere, O'Leary-Barrett, Banaschewski, Bokde and Bromberg2016; Gomez, Stavropoulos, Vance, & Griffiths, Reference Gomez, Stavropoulos, Vance and Griffiths2018; Laceulle, Vollebergh, & Ormel, Reference Laceulle, Vollebergh and Ormel2015; Martel et al., Reference Martel, Pan, Hoffmann, Gadelha, do Rosário, Mari and Salum2017; Murray, Eisner, & Ribeaud, Reference Murray, Eisner and Ribeaud2016; Neumann et al., Reference Neumann, Pappa, Lahey, Verhulst, Medina-Gomez, Jaddoe and Tiemeier2016; Patalay et al., Reference Patalay, Fonagy, Deighton, Belsky, Vostanis and Wolpert2015; Schaefer et al., Reference Schaefer, Moffitt, Arseneault, Danese, Fisher, Houts and Caspi2018; Snyder, Young, & Hankin, Reference Snyder, Young and Hankin2017). Critically, several studies have shown that child maltreatment increases this transdiagnostic psychopathology with no residual associations with specific symptoms types after accounting for the links with this latent factor (Caspi et al., Reference Caspi, Houts, Belsky, Goldman-Mellor, Harrington, Israel and Moffitt2014; Keyes et al., Reference Keyes, Eaton, Krueger, McLaughlin, Wall, Grant and Hasin2012). The p factor is therefore a useful tool for quantifying, in a single variable, co-occurrence of multiple types of psychopathology symptoms associated with childhood maltreatment. Emotion dysregulation may be a key mechanism through which maltreatment increases risk for general psychopathology (Beauchaine & Zisner, Reference Beauchaine and Zisner2017; Carver et al., Reference Carver, Johnson and Timpano2017).
The Current Study
The current study investigated the role of emotion dysregulation as a transdiagnostic mechanism linking childhood maltreatment to the development of psychopathology. First, we hypothesized that child maltreatment would be associated with lower levels of adaptive, antecedent-focused emotion regulation strategies (i.e., attention deployment and cognitive reappraisal) and greater use of maladaptive, response-focused emotion regulation strategies (i.e., expressive suppression and rumination). We also expected to replicate the well-established finding of heightened emotional reactivity in children who had been maltreated. Second, we expected that maltreatment would interact with age in relation to attention biases toward threat, such that younger participants exposed to maltreatment would show larger attentional biases toward threat than older participants exposed to maltreatment, who might be more capable of effortfully regulating their attention. Third, we predicted that lower use of adaptive antecedent-focused emotion regulation strategies, greater use of maladaptive response-focused emotion regulation strategies, and heightened emotional reactivity would each be associated with higher scores on our measure of general psychopathology, and would mediate the association between child maltreatment and this outcome.
Method
Sample
Youth aged 8–16 years and a parent or guardian were recruited to participate in a study examining child trauma exposure, emotion regulation, and psychopathology. A total of 262 youth aged 8–16 years were enrolled into the study. Exposure to maltreatment and other inclusion and exclusion criteria were assessed during the first study visit, along with several behavioral and self-report measures of emotion regulation. Youth and caregivers were recruited for participation at schools, after-school and prevention programs, adoption programs, food banks, shelters, parenting programs, medical clinics, and the general community in Seattle, Washington, between January 2015 and June 2017. Recruitment efforts were targeted at recruiting a sample with variation in exposure to maltreatment-related trauma. To do so, we recruited from neighborhoods with high levels of violent crime, from clinics that served a predominantly low-socioeconomic status catchment area, and agencies that work with families who have been victims of violence (e.g., domestic violence shelters and programs for parents mandated to receive intervention by Child Protective Services). Inclusion criteria for the maltreated group included exposure to physical or sexual abuse or direct witnessing of domestic violence. Children in the control group were matched to children in the maltreated group on age, sex, and handedness; inclusion criteria required an absence of exposure to maltreatment or other forms of significant interpersonal violence. Exclusion criteria included IQ < 80, presence of pervasive developmental disorder, active psychotic symptoms or mania, active substance abuse, and presence of safety concerns. IQ was measured with the Wechsler Abbreviated Intelligence Scale (Wechsler, Reference Wechsler2011) in the first study visit. Pervasive developmental disorders were assessed via parent report. Of the 262 children enrolled in the first study visit, 3 were excluded from all analysis due to low IQ (n = 1), presence of pervasive developmental disorder (n = 1), and presence of psychotic symptoms and drug abuse (n = 1). The total sample size for the present analysis was 259 children and adolescents. A longitudinal follow-up assessment was conducted approximately 2 years following the baseline assessments (M = 21.96 months, SD = 7.88 months) to assess symptoms of psychopathology. A total of 198 children and adolescents (76.4%) completed a follow-up visit. Of the 65 children who dropped out, 44 were maltreated (28% attrition) and 21 were not (20% attrition; χ2 = 2.38, p = .123).
All procedures were approved by the institutional review board at the University of Washington. Written informed consent was obtained from legal guardians; children provided written assent. Maltreatment not previously reported to the relevant authorities was reported to Child Protective Services using standard clinical procedures. Children with active safety concerns were not enrolled in the study. See Table 1 for sociodemographic characteristics of the sample.
Table 1. Descriptive statistics and intercorrelations

M, mean. SD, standard deviation. All pairwise, Pearson correlations. *p < .05.
Measures
For younger children in the study (8–10 year olds) and those who had difficulty reading, all questionnaires were read out loud by a study team member to ensure comprehension of all items.
Child maltreatment
For the purposes of this study, child maltreatment was defined as exposure to traumatic violence or abuse within the family, including physical, sexual, and emotional abuse, and chronic exposure to domestic violence. We used a multi-informant, multimethod approach for assessing exposure to child maltreatment. Children completed two interviews with a trained member of our research team assessing child maltreatment experiences and exposure to interpersonal violence: the Childhood Experiences of Care and Abuse (CECA) Interview (Bifulco, Brown, & Harris, Reference Bifulco, Brown and Harris1994) and the Violence Exposure Scale for Children—Revised (VEX-R; Raviv et al., Reference Raviv, Erel, Fox, Leavitt, Raviv, Dar and Greenbaum2001; Raviv, Raviv, Shimoni, Fox, & Leavitt, Reference Raviv, Raviv, Shimoni, Fox and Leavitt1999). The CECA assesses caregiving experiences, including physical, sexual, and emotional abuse. We modified the interview to ask parallel questions about witnessing domestic violence (i.e., directly observing violence directed at a caregiver). Interrater reliability for maltreatment reports is excellent, and validation studies suggest high agreement between siblings on maltreatment reports (Bifulco, Brown, Lillie, & Jarvis, Reference Bifulco, Brown, Lillie and Jarvis1997). The VEX-R assesses the frequency of exposure to different forms of violence. Children are presented with a cartoon and caption depicting a child of the same sex witnessing a type of violence (e.g., “Chris sees a person slap another person really hard”) and experiencing that same type of violence (e.g., “A person slaps Chris really hard”). Children are then asked to report how frequently they have witnessed or experienced that type of violence (e.g., “How many times have you seen a person slap another person really hard?” or “How many times has a person slapped you really hard?”) on a Likert scale ranging from 0 (never) to 3 (lots of times). We added follow-up questions for each item that was endorsed to gather additional information (e.g., the perpetrator or age of onset). The VEX-R demonstrates good reliability and has been validated with children as young as second grade (Raviv et al., Reference Raviv, Raviv, Shimoni, Fox and Leavitt1999, Reference Raviv, Erel, Fox, Leavitt, Raviv, Dar and Greenbaum2001).
Children also completed two self-report measures: the Childhood Trauma Questionnaire (CTQ; Bernstein, Ahluvalia, Pogge, & Handelsman, Reference Bernstein, Ahluvalia, Pogge and Handelsman1997) and the UCLA PTSD Reaction Index (PTSD-RI; Steinberg, Brymer, Decker, & Pynoos, Reference Steinberg, Brymer, Decker and Pynoos2004). The CTQ is a 28-item scale that assesses the frequency of maltreatment during childhood, including physical and sexual abuse. Validated thresholds for exposure to physical and sexual abuse (Walker et al., Reference Walker, Unutzer, Rutter, Gelfand, Saunders, VonKorff and Katon1999) were applied here in evaluating abuse exposure based on the CTQ. The CTQ has excellent psychometric properties including internal consistency, test–retest reliability, and convergent and discriminant validity with interviews and clinician reports of maltreatment (Bernstein et al., Reference Bernstein, Fink, Handelsman, Foote, Lovejoy, Wenzel and Ruggiero1994, Reference Bernstein, Ahluvalia, Pogge and Handelsman1997). The PTSD-RI includes a trauma screen that assesses exposure to numerous traumatic events, including physical abuse, sexual abuse, and domestic violence, and additionally assesses PTSD symptoms. The PTSD-RI has good internal consistency and convergent validity (Steinberg et al., Reference Steinberg, Brymer, Kim, Briggs, Ippen, Ostrowski and Pynoos2013).
Caregivers completed three self-report measures: the Conflict Tactics Scale—Parent Child Version (CTS; Straus, Hamby, Finkelhor, Moore, & Runyan, Reference Straus, Hamby, Finkelhor, Moore and Runyan1998), the Juvenile Victimization Questionnaire (JVQ) lifetime caregiver report (Finkelhor, Hamby, Ormrod, & Turner, Reference Finkelhor, Hamby, Ormrod and Turner2005), and the caregiver version of the PTSD-RI. The CTS includes 22 items assessing caregiver responses to child disobedience or misbehavior in the past year. Caregivers indicate how frequently they have used each strategy (e.g., shook him/her) on a Likert scale ranging from 0 (this has never happened) to 6 (more than 20 times in the past year) and can also indicate if they have used the strategy in the past but not in the last year. The CTS has adequate reliability and good discriminant and construct validity (Straus et al., Reference Straus, Hamby, Finkelhor, Moore and Runyan1998). The JVQ includes 34 items assessing exposure to crime, child maltreatment, peer and sibling victimization, sexual victimization, and witnessing and indirect victimization and has excellent psychometric properties, including test–retest reliability and construct validity (Finkelhor et al., Reference Finkelhor, Hamby, Ormrod and Turner2005). Caregivers endorsed whether their child had experienced each event in his/her lifetime. Caregivers also completed the trauma screen included in the PTSD-RI, described above. A trained interviewer followed up with the caregiver if he/she endorsed any form of abuse or domestic violence to gather additional information about the experience.
Children were classified as experiencing physical or sexual abuse if abuse was endorsed by the child (on the CECA interview, PTSD-RI trauma screen, or above the validated CTQ threshold) or parent (on the CTS, JVQ, or PTSD-RI trauma screen). A total of 100 children (38.6%) experienced physical or sexual abuse. Interrater reliability was fair to good for child and caregiver reports (82.0% agreement; κ = .62). Exposure to emotional abuse (above the validated threshold on either the CECA or the CTQ) and domestic violence (on the VEX-R interview or the PTSD-RI trauma screen) was determined based on child report only. A total of 82 children (31.7%) reported experiencing emotional abuse, and 99 children (38.2%) reported witnessing domestic violence.
A maltreatment severity score was created by summing the total number of types of maltreatment and violence exposure experienced by the child, including physical abuse, sexual abuse, emotional abuse, domestic violence, and exposure to violence in the broader community. Each type of maltreatment or violence exposure was coded as present or absent, and these indicators were summed to create a severity score.
Emotional reactivity and regulation
Attention bias to threat
A visual dot-probe task using affective faces was administered to assess attention bias to threat. This task has been widely used as a measure of attention bias to threat in children and adolescents (Briggs-Gowan et al., Reference Briggs-Gowan, Pollak, Grasso, Voss, Mian, Zobel and Pine2015; Pérez-Edgar et al., Reference Pérez-Edgar, Bar-Haim, McDermott, Chronis-Tuscano, Pine and Fox2010; Waters, Henry, Mogg, Bradley, & Pine, Reference Waters, Henry, Mogg, Bradley and Pine2010). Task stimuli consisted of face pairs with one angry face and one neutral face from the same actor, selected from the NimStim stimulus set (Tottenham, Borscheid, Ellertsen, Marcus, & Nelson, Reference Tottenham, Borscheid, Ellertsen, Marcus and Nelson2002). The task included 16 practice trials followed by two experimental blocks of 80 trials each. Participants were randomly assigned to one of three pseudorandom orders of stimulus presentation. Each trial began with a central fixation cross presented for 500 ms, followed by an angry–neutral face pair presented for 500 ms, followed immediately by a small white arrow, pointing either left or right, displayed for 500 ms. The arrow appeared in the space previously occupied by the center of one of the two face pictures. Angry faces were presented with equal frequency on either the right or the left side of the screen. Left and right arrows appeared with equal frequency in the location of the angry or neutral face. Participants were instructed to press the arrow key on the keyboard corresponding to the arrow on the screen, as quickly as possible, avoiding mistakes. Accuracy and response times were recorded. A measure of attention bias toward threat was obtained by subtracting the mean response time on correct trials when the arrow appeared behind the angry face, from mean response time on correct trials when the arrow appeared behind the neutral face. Positive scores indicate an attention bias toward threat; negative scores indicate attention away from threat.
Rumination
The Children's Response Styles Questionnaire (Abela, Brozina, & Haigh, Reference Abela, Brozina and Haigh2002) is a 25-item scale that assesses the extent to which children respond to sad feelings with rumination, defined as self-focused thought concerning the causes and consequences of depressed mood, distraction, or problem solving. The measure is modeled after the Response Styles Questionnaire (Nolen-Hoeksema & Morrow, Reference Nolen-Hoeksema and Morrow1991) that was developed for adults. For each item, youth are asked to rate how often they respond in that way when they feel sad on a 4-point Likert scale ranging from almost never (1) to almost always (4). The rumination subscale includes 13 items that are summed, with higher scores indicating greater habitual engagement of rumination. Sample items include: “Think about a recent situation wishing it had gone better” and “Think why can't I handle things better?” The Children's Response Styles Questionnaire has demonstrated good psychometric properties (Abela et al., Reference Abela, Brozina and Haigh2002) and had good internal consistency in this sample (α = 0.91).
Reappraisal and suppression
The Emotion Regulation Questionnaire (ERQ; Gross & John, Reference Gross and John2003) is a 10-item self-report questionnaire assessing the tendency to use cognitive reappraisal and expressive suppression. Six items pertain to cognitive reappraisal (e.g., “I control my emotions by changing the way I think about the situation I'm in”), and 4 pertain to expressive suppression (e.g., “I control my emotions by not expressing them”). Responses are provided on a 7-point Likert scale ranging from strongly disagree (1) to strongly agree (7). Separate sum scores are calculated for cognitive reappraisal and expressive suppression. Higher scores indicate a greater tendency to use that strategy. Both the reappraisal (α = 0.84) and the expressive suppression subscales (α = 0.75) demonstrated adequate internal consistency in this sample.
Emotional reactivity
The Emotion Reactivity Scale (ERS) is a 21-item scale that assesses stable patterns of emotional reactivity (Nock, Wedig, Holmberg, & Hooley, Reference Nock, Wedig, Holmberg and Hooley2008). The ERS asks participants to think about how they experience emotions on a regular basis, such as anger, sadness, excitement, or other emotions. The ERS items assess emotional sensitivity (8 items; e.g., “I tend to get emotional very easily”), arousal/intensity of emotional experiences (10 items; e.g., “When I experience emotions, I feel them very strongly/intensely”), and persistence of emotions (3 items; e.g., “When I am angry/upset, it takes me much longer than most people to calm down”), which are summed to create an overall emotion reactivity score. Participants rate each item on a 5-point Likert scale ranging from not at all like me (0) to completely like me (4), with a total possible score ranging from 0 to 84. The ERS has demonstrated excellent reliability and validity among adolescents (Nock et al., Reference Nock, Wedig, Holmberg and Hooley2008), and demonstrated excellent internal consistency in this study (α = 0.92).
Income-to-needs ratio
Income-to-needs ratio was calculated by dividing the parent-reported family income by the poverty threshold for a family of that size as indicated by the US Census Bureau (www.census.gov/hhes/www/poverty/data/threshld/). Family income was not reported for 17 participants (12 maltreated). Multiple imputation with 100 imputations was conducted using the mice package in R (Van Buuren & Groothuis-Oudshoorn, Reference Van Buuren and Groothuis-Oudshoorn2011) to estimate income in all regression analyses. For mediation analyses, the mean income of all other maltreated children was imputed for all maltreated children missing income data, and the mean income of all other nonmaltreated children was imputed for all nonmaltreated children with missing income data.
Symptoms of psychopathology
Depression symptoms were assessed with the Children's Depression Inventory—Second edition (CDI-2), a recently revised version of the widely used self-report measure of depressive symptoms in children and adolescents (Kovacs, Reference Kovacs1992, Reference Kovacs2011). The CDI has demonstrated good reliability and validity among children and adolescents (Craighead, Smucker, Craighead, & Ilardi, Reference Craighead, Smucker, Craighead and Ilardi1998). The CDI demonstrated excellent internal consistency in our sample (α = 0.89). Anxiety symptoms were assessed with the Screen for Child Anxiety Related Emotional Disorders (SCARED), which measures anxiety disorder symptoms across five domains: panic/somatic, generalized anxiety, separation anxiety, social phobia, and school phobia (Birmaher et al., Reference Birmaher, Khetarpal, Brent, Cully, Balach, Kaufman and Neer1997). The SCARED has sound psychometric properties (Birmaher et al., Reference Birmaher, Khetarpal, Brent, Cully, Balach, Kaufman and Neer1997, Reference Birmaher, Brent, Chiappetta, Bridge, Monga and Baugher1999) and excellent internal consistency in our sample (α = 0.94). Externalizing symptoms were assessed using both child and caregiver reports on the Youth Self-Report (YSR) and Child Behavior Checklist (CBCL; Achenbach, Reference Achenbach1991). The YSR/CBCL scales are among the most widely used measures of youth emotional and behavioral problems. The higher raw score between the CBCL and YSR was used from the attention problems, rule-breaking behaviors, and aggressive behavior subscales. Symptoms of PTSD were assessed using child- and parent-report versions of the PTSD-RI (Steinberg et al., Reference Steinberg, Brymer, Decker and Pynoos2004). The PTSD-RI assesses PTSD reexperiencing, avoidance/numbing, and hyperarousal symptoms according to DSM-IV criteria. A total symptom severity score is generated by summing all items. The PTSD-RI has sound psychometric properties (Steinberg et al., Reference Steinberg, Brymer, Kim, Briggs, Ippen, Ostrowski and Pynoos2013), and had excellent internal consistency in our sample (α = 0.92). The higher of the parent- and child-reported PTSD symptom severity score was used. Given that half our sample was recruited for exposure to maltreatment, these psychopathology indicators were positively skewed and kurtotic (skewness values above 1 ranged from 1.1 to 2.27; kurtosis values above 1 ranged from 1.1 to 6.94). We used each of these indicators to define “p.”
Defining p factor
Following Caspi et al. (Reference Caspi, Houts, Belsky, Goldman-Mellor, Harrington, Israel and Moffitt2014) and recent replications (Laceulle et al., Reference Laceulle, Vollebergh and Ormel2015; Schaefer et al., Reference Schaefer, Moffitt, Arseneault, Danese, Fisher, Houts and Caspi2018), we performed confirmatory factor analysis (CFA) to test two standard models: a correlated-factors model specifying internalizing and externalizing latent factors and a bifactor model specifying both a general psychopathology latent factor (“p”) and residual internalizing and externalizing factors (Figure 1). In order to ensure that our latent factors were not being driven by one or more indicators simply because of measurement differences across psychopathology instruments (i.e., different number of items, scoring, etc.), we binned scores on each indicator into deciles prior to CFA analyses. All CFA analyses were performed in MPlus version 8.1 (Muthén & Muthén, Reference Muthén and Muthén2012). Given that our observed indicator variables were slightly skewed and kurtotic, we used the robust maximum likelihood estimator, which employs a sandwich estimator to arrive at standard errors robust to nonnormality of observations. The robust maximum likelihood estimator performs well in modest sample sizes with skewed data, as in the present study (Li, Reference Li2016). We assessed the relative fit of each model using the Akaike information criterion (AIC), Bayesian information criterion (BIC), and the sample adjusted BIC. Fit indices for the correlated-factors model were AIC = 6056.31, BIC = 6249.00, sample adjusted BIC = 6077.79. Standardized factor loadings for the internalizing (CDI, SCARED, PTSD) latent factor ranged from 0.65 to 0.73, all ps < .001. Standardized factor loadings for the externalizing (aggressive behaviors, rule-breaking behaviors, and attention problem) latent factor ranged from 0.76 to 0.87, all ps < .001. Fit indices for the bifactor model were AIC = 6018.23, BIC = 6228.77, sample adjusted BIC = 6041.71. Standardized factor loadings for the latent p factor (CDI, SCARED, PTSD, aggressive behaviors, rule-breaking behaviors, and attention problems) ranged from 0.44 to 0.80, all ps < .001. Fit indices for the correlated factors model at follow-up were AIC = 4507.81, BIC = 4682.09, sample adjusted BIC = 4514.19. Standardized factor loadings for the internalizing factor ranged from 0.48 to 0.95, all ps < .001. Standardized factor loadings for the externalizing factor ranged from 0.76 to 0.84, all ps < .001. Fit indices for the bifactor model at the longitudinal follow-up were AIC = 4481.00, BIC = 4665.15, sample adjusted BIC = 4487.74. Standardized factor loadings for the latent p factor ranged from 0.46 to 0.81, all ps < .001. As assessed by relative fit indices and factor loadings, both models fit the data similarly well at the baseline assessment, with a relatively better fit for the bifactor model. In the present analyses, we used the bifactor model because it is the most commonly reported general factor model of psychopathology in the existing literature (Caspi et al., Reference Caspi, Houts, Belsky, Goldman-Mellor, Harrington, Israel and Moffitt2014; Greene & Eaton, Reference Greene and Eaton2017; Laceulle et al., Reference Laceulle, Vollebergh and Ormel2015; Lahey et al., Reference Lahey, Applegate, Hakes, Zald, Hariri and Rathouz2012; Martel et al., Reference Martel, Pan, Hoffmann, Gadelha, do Rosário, Mari and Salum2017; Murray et al., Reference Murray, Eisner and Ribeaud2016; Olino, Dougherty, Bufferd, Carlson, & Klein, Reference Olino, Dougherty, Bufferd, Carlson and Klein2014; Patalay et al., Reference Patalay, Fonagy, Deighton, Belsky, Vostanis and Wolpert2015; Schaefer et al., Reference Schaefer, Moffitt, Arseneault, Danese, Fisher, Houts and Caspi2018; Snyder et al., Reference Snyder, Young and Hankin2017), including in studies comparing the p factor in children with and without exposure to adversity.
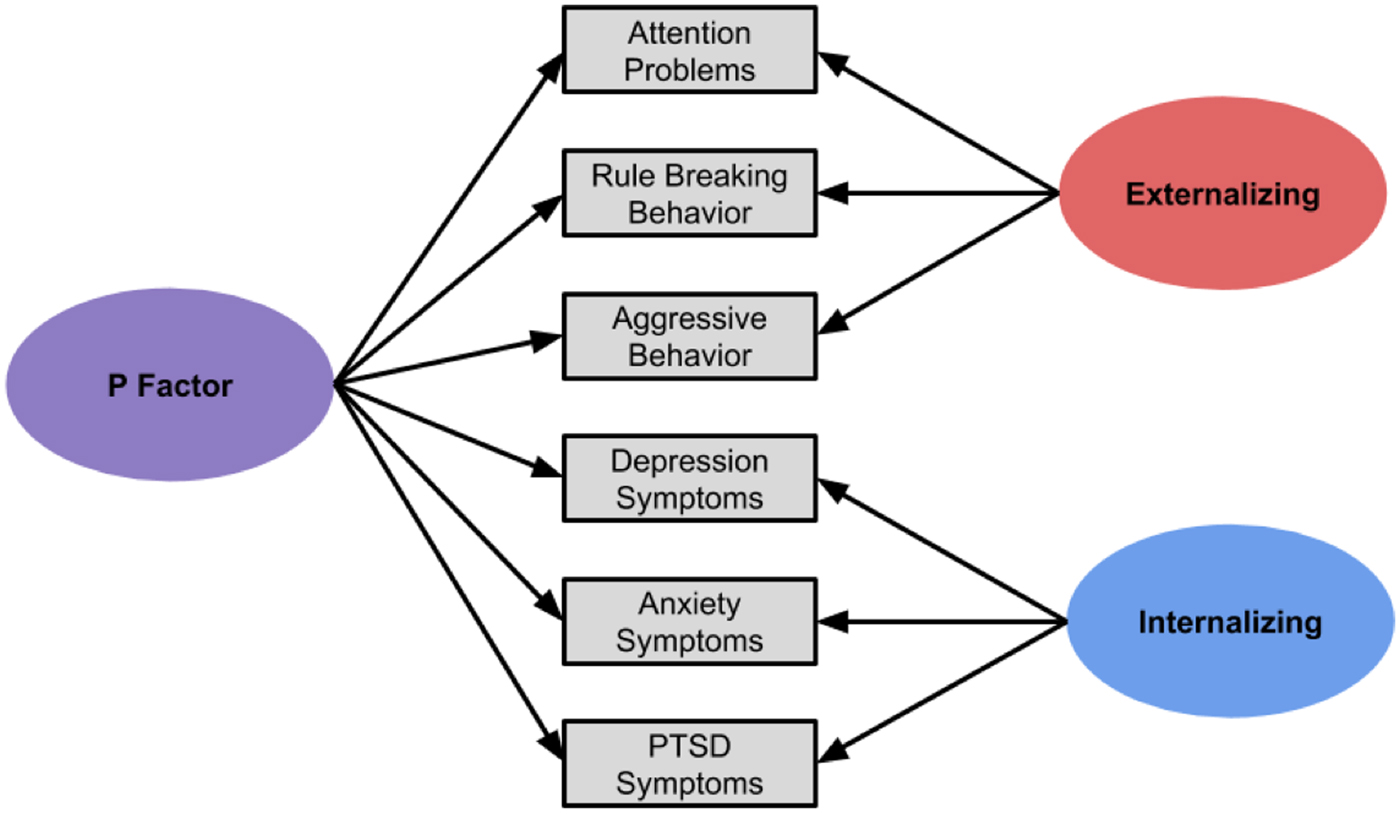
Figure 1. Factor structure of the bifactor model used to generate p factor scores from transdiagnostic symptom counts.
Our aim in estimating “p” in this sample was to condense an array of disparate psychiatric measures into a single transdiagnostic measure of psychopathology using a well-validated approach, not to characterize the latent structure of psychopathology in the general population. To ensure that our recruitment strategy did not unduly influence the latent structure of “p” in our sample, we fit the bifactor model separately in our maltreated participants and nonmaltreated controls. Because fit indices are sensitive to sample size and we had more maltreated cases than controls, we were not able to directly compare model fit indices. However, we examined standardized factor loadings to ensure that the models fit the data similarly in each group (see online-only Supplementary Materials for details). With the exception of rule-breaking behavior (.65 in maltreated youth, .37 in control youth) and PTSD (.73 in maltreated youth, .50 in control youth), factor loadings were very similar, and all standardized factor loadings were significant at p < .001 in both groups.
Analysis methods
Linear regression analyses were conducted in R (R Core Team, 2018) to examine each of our hypotheses. We examined the association of maltreatment exposure and maltreatment severity with threat bias, emotional reactivity, cognitive reappraisal, expressive suppression, and rumination. To evaluate whether these associations varied by age, we computed interactions of maltreatment exposure and severity with age and examined their association with threat bias, cognitive reappraisal, emotional reactivity, expressive suppression, and rumination. Significant interactions were visualized using the interActive data visualization tool (McCabe, Kim, & King, Reference McCabe, Kim and King2018). To determine how emotion regulation was related to psychopathology, we examined associations of threat bias, cognitive reappraisal, emotional reactivity, expressive suppression, and rumination with “p,” both at baseline and at the longitudinal follow-up controlling for “p” at baseline; these analyses controlled for maltreatment exposure. All analyses included covariates for racial/ethnic minority status and family income-to-needs ratio, as the maltreated and control groups differed on these variables. Regression analyses and mediation models predicting “p” at follow-up were conducted only among the 198 adolescents with follow-up data.
Mediation models with bootstrapped confidence intervals (10,000 iterations) were tested using version 2.13 of the process macro in SPSS (Hayes, Reference Hayes2013) for emotion regulation indices that were significantly related to both maltreatment exposure or severity and “p” at follow-up, controlling for “p” at baseline and maltreatment exposure or severity. We evaluated whether difficulties with emotion regulation mediated the association between maltreatment exposure and severity and “p” at the longitudinal follow-up, controlling for the effects of baseline “p,” racial/ethnic minority status, and income-to-needs ratio on “p.” Indices of maltreatment, emotional reactivity, and all control variables were collected concurrently. However, indices of maltreatment were retrospective. Data used to calculate “p” at follow-up was collected 2 years later.
Results
Descriptive statistics
Descriptive statistics for maltreated and control youth and intercorrelations of study variables are summarized in Table 1. Average reaction time during the dot-probe task was significantly faster for trials when the target was behind the neutral face than when it was behind the angry face, suggesting an attention bias away from threat in the total sample (M = –6.18, SD = 36.58, t = –2.71, p = .007). Cognitive reappraisal (M = 27.41, SD = 7.51) and expressive suppression (M = 14.88, SD = 5.70) were used at moderate levels in this sample, with mean totals over half of the maximum possible scores of 42 and 28, respectively. Rumination was somewhat less commonly used, with a mean score of 24.01 (SD = 8.64) out of a possible 52. Age was positively correlated with rumination (r = .35, p < .001) and emotional reactivity (r = .16, p = .009), but not threat bias (r = .11, p = .074), cognitive reappraisal (r = .04, p = .513), or expressive suppression (r = .11, p = .088). Indices of emotion regulation and emotional reactivity were mostly uncorrelated, with the exceptions that youth who reported greater rumination also reported greater expressive suppression (r = .21, p = .001) and emotional reactivity (r = .63, p < .001).
Maltreatment and antecedent-focused emotion regulation
Results of regression analyses relating maltreatment exposure and severity to emotion regulation are summarized in Tables 2 and 3. Neither maltreatment exposure (Table 2, Model 1) nor maltreatment severity (Table 2, Model 3) were associated with attention bias toward or away from threat. However, both maltreatment exposure (β = –.133, p = .038; Table 2, Model 2) and maltreatment severity (β = –.142, p = .030; Table 2, Model 4) interacted with age in predicting threat bias. In both cases, maltreatment exposure and greater maltreatment severity were associated with greater attention bias toward threat cues in children that disappeared during early adolescence and shifted to a significant attention bias away from threat in older adolescents (Figure 2). Neither maltreatment exposure nor severity was associated with cognitive reappraisal (Table 3). These associations did not vary with age.

Figure 2. Attention bias toward threat increases significantly with increasing maltreatment severity for younger (1.5 SD below the mean = 8.7 and 1 SD below the mean = 10.0 year old) participants and decreases significantly with increasing maltreatment for the oldest (1.5 SD above the mean = 16.5 year old) participants. Figure produced using the interActive data visualization tool (McCabe, Kim, & King, Reference McCabe, Kim and King2018).
Table 2. Regression table of effects of maltreatment, age, and their interaction on attention bias to threat

Note: Significant effects are in bold. B, unstandardized coefficient; β, standardized coefficient.
Table 3. Regression tables of main effects of maltreatment and maltreatment severity on emotion reactivity and regulation

Note: Significant effects are in bold. B, unstandardized coefficient. β, standardized coefficient.
Maltreatment and emotional reactivity
Maltreatment exposure and severity were both positively associated with emotional reactivity (β = .383, p < .001), such that participants who experienced maltreatment and greater maltreatment severity reported greater emotional reactivity (Table 3). Age did not interact with maltreatment exposure or severity in predicting emotional reactivity.
Maltreatment and response-focused emotion regulation
Maltreatment exposure was unrelated to expressive suppression. However, maltreatment severity was positively associated with expressive suppression (β = .194, p = .009), such that participants who experienced more severe maltreatment reported using expressive suppression more frequently (Table 3). Age did not interact with maltreatment exposure or severity in predicting expressive suppression.
Rumination was positively associated with both maltreatment exposure (β = .301, p < .001) and maltreatment severity (β = .447, p < .001). Children who experienced maltreatment were more likely to ruminate than those who had never been maltreated, and greater maltreatment severity was associated with greater engagement in rumination (Table 3). Age did not interact with maltreatment exposure or severity in predicting rumination.
Emotion regulation and psychopathology
Associations of emotion regulation strategies and emotional reactivity with “p” scores at baseline and at the longitudinal follow-up, controlling for baseline, are summarized in Table 4. Coefficients and test statistics of the full models are available in the online-only Supplementary Materials. First, we examined antecedent-focused emotion regulation strategies. Biased attention to threat was not associated with “p” at baseline, but did significantly predict higher “p” scores at the follow-up (β = .134, p = .021), indicating that youth with greater attention biases toward threat demonstrated greater increases in psychopathology over time. Cognitive reappraisal was not associated with “p” at either baseline or follow-up. Second, youth with higher emotional reactivity had higher “p” at baseline (β = .379, p < .001), and marginally greater increases in “p” at follow-up (β = .128, p = .072). Finally, we examined response-focused strategies. Youth who used expressive suppression more had higher “p” at baseline (β = .167, p < .001), but not at follow-up, (β = .063, p = .299). Youth who engaged in rumination more frequently had higher “p” at baseline (β = .301, p < .001), and greater increases in “p” at the follow-up (β = .175, p = .004).
Table 4. Associations of emotion regulation and reactivity with psychopathology

Note: Significant effects are in bold. B, unstandardized coefficient. β, standardized coefficient. All models controlled for race/ethnicity and income-to-needs ratio. Results of full models are in online-only Supplemental Materials.
Indirect effects of maltreatment on psychopathology through emotion dysregulation
Because the component paths were at least marginally significant, we examined whether emotional reactivity and rumination at baseline mediated the association between maltreatment exposure and severity and “p” at the longitudinal follow-up, controlling for “p” at baseline (Figure 3a). The total effect of maltreatment on “p” at follow-up when controlling for “p” at baseline was not significant (c = –.017, p = .901), but it is well established that a significant c path is not required to test for indirect effects (Hayes, Reference Hayes2013; MacKinnon, Fairchild, & Fritz, Reference MacKinnon, Fairchild and Fritz2007). We found a significant indirect effect of maltreatment exposure on “p” at follow-up through baseline emotional reactivity and rumination in parallel (95% confidence interval [.015, .210]). In contrast to maltreatment exposure, maltreatment severity was significantly associated with “p” at follow-up when controlling for “p” at baseline (c = .044, p = .016). The indirect effect of maltreatment severity on “p” at follow-up through baseline emotional reactivity and rumination in parallel was statistically significant (95% confidence interval [.002, .037]).

Figure 3. Models used to test the indirect effects of maltreatment and maltreatment severity on psychopathology (p factor) at follow-up, via emotional reactivity and rumination, controlling for baseline psychopathology. Income-to-needs ratio and racial minority status were also included as covariates in both models. Independent variables (maltreatment exposure and severity), mediators (emotional reactivity and rumination), and covariates (p factor at baseline, race/ethnicity, and income-to-needs) were collected concurrently, but independent variables were retrospective. Dependent variable (p factor at follow-up) was collected 2 years later. Standardized coefficients are shown. Solid lines indicate significant paths. Dotted lines indicate nonsignificant paths.
Discussion
We investigated the role of emotion regulation processes occurring at multiple stages of the emotion generation process as transdiagnostic mechanisms linking childhood maltreatment with psychopathology across childhood and adolescence. Maltreatment was associated with emotion dysregulation, as indicated by increased engagement in maladaptive response-focused emotion regulation strategies and heightened emotional reactivity, which in turn were associated with greater general psychopathology both concurrently and longitudinally. The associations between maltreatment and emotion regulation were largely age-invariant, with the exception of attention biases toward or away from threat. Specifically, maltreated children had greater attention biases toward threat that shifted to an attention bias away from threat in older adolescents. Further, youth with preferential attention to threat had increased psychopathology over time, conversely demonstrating that attention away from threat was associated with decreased psychopathology over time. Thus, the age-specific shift in bias direction found in the current study may reflect an adaptive strategy that buffers against risk for psychopathology among maltreated adolescents.
Childhood maltreatment is associated with multiple forms of emotion dysregulation. Specifically, children and adolescents who were maltreated and who experienced more severe maltreatment exhibited a greater tendency to engage in maladaptive, response-focused strategies like expressive suppression and rumination and also had increased emotional reactivity relative to children who had never been maltreated. These findings are consistent with a growing body of research using multiple methods and modalities demonstrating that childhood maltreatment, particularly forms of maltreatment that involve abuse and interpersonal violence, are associated with heightened emotional reactivity, as measured by self-report (Glaser et al., Reference Glaser, van Os, Portegijs and Myin-Germeys2006; Heleniak et al., Reference Heleniak, Jenness, Vander Stoep, McCauley and McLaughlin2016; McLaughlin et al., Reference McLaughlin, Kubzansky, Dunn, Waldinger, Vaillant and Koenen2010). The self-reported heightened emotional reactivity is corroborated by studies that find increased reactivity in neurobiological systems involved in emotional responding in maltreated youth, including the amygdala (Hein & Monk, Reference Hein and Monk2017; McCrory et al., Reference McCrory, De Brito, Sebastian, Mechelli, Bird, Kelly and Viding2011; McLaughlin et al., Reference McLaughlin, Peverill, Gold, Alves and Sheridan2015; Viding et al., Reference Viding, Sebastian, Dadds, Lockwood, Cecil, De Brito and McCrory2012). This suggests that maltreated children and adolescents may experience more intense emotions, perhaps contributing to, but also resulting from, emotion dysregulation.
To our knowledge, this is the first study to investigate the association between childhood maltreatment and engagement in expressive suppression. The positive association between expressive suppression and maltreatment severity is consistent with previous findings that harsh and inconsistent discipline is associated with increased use of this strategy in children (Balan et al., Reference Balan, Dobrean, Roman and Balazsi2017). When engagement in expressive suppression fails to prevent intrusive and intense negative thoughts and feelings, maltreated youth may dwell or ruminate on these distressing emotions. Consistent with past studies of maltreatment and other forms of early life stress (Conway et al., Reference Conway, Mendelson, Giannopoulos, Csank and Holm2004; Heleniak et al., Reference Heleniak, Jenness, Vander Stoep, McCauley and McLaughlin2016; LeMoult et al., Reference LeMoult, Humphreys, King, Colich, Price, Ordaz and Gotlib2018; McLaughlin & Hatzenbuehler, Reference McLaughlin and Hatzenbuehler2009), we found that maltreated children and adolescents engage in greater habitual use of rumination than children who have not experienced maltreatment. Building on control theory, (Carver & Scheier, Reference Carver and Scheier1982; Martin & Tesser, Reference Martin, Tesser and Wyer1996), we have previously argued that chronic and uncontrollable stressors might increase engagement in rumination because they either create or accentuate discrepancies between goals or desired states and one's actual situation (Michl et al., Reference Michl, McLaughlin, Shepherd and Nolen-Hoeksema2013). Experiences of maltreatment are inherently uncontrollable and often chronic, and thus may be particularly likely to generate discrepancies between one's current situation and desired states that cannot be resolved. Overall, our findings indicate that maltreatment can trigger a pattern of emotion dysregulation characterized by heightened emotional reactivity, which is unaided or exacerbated by greater engagement in maladaptive emotion regulation strategies, which may actually increase the intensity and duration of negative emotions.
Tendencies to engage in cognitive reappraisal were not associated with child maltreatment. This is consistent with the view that greater engagement in maladaptive emotion regulation is a more consistent mechanism conveying risk for psychopathology than decreased engagement in adaptive emotion regulation (Aldao & Nolen-Hoeksema, Reference Aldao and Nolen-Hoeksema2012a, Reference Aldao and Nolen-Hoeksema2012b; Aldao et al., Reference Aldao, Nolen-Hoeksema and Schweizer2010). It may be that while the tendency to engage in cognitive reappraisal is unrelated to childhood maltreatment, the capacity to utilize this strategy effectively may be nonetheless diminished in children and adolescents exposed to maltreatment. For example, maltreated adolescents have been found to engage prefrontal cortex more than nonmaltreated adolescents during a cognitive reappraisal task in which their self-reported change in negative affect did not differ (McLaughlin et al., Reference McLaughlin, Peverill, Gold, Alves and Sheridan2015), suggesting they may need to employ more regulatory effort to achieve the same emotional outcome.
Most of the associations between maltreatment and emotion regulation observed in this study were age invariant. However, age did interact with maltreatment exposure and maltreatment severity in relation to attention bias to threat. In children, maltreatment severity was associated with larger attention bias toward threat; in early adolescence, no association was observed between maltreatment severity and attention bias to threat, and among older adolescents, greater maltreatment severity was associated with attention bias away from threat. Attention bias away from threat was in turn associated with lower psychopathology at follow-up, consistent with past findings linking attention biases to threat-related cues with psychopathology, in particular anxiety (Hankin, Gibb, Abela, & Flory, Reference Hankin, Gibb, Abela and Flory2010; Lau & Waters, Reference Lau and Waters2017; Waters et al., Reference Waters, Henry, Mogg, Bradley and Pine2010). The association between abuse and attention bias toward threatening stimuli is consistent with prior work (Briggs-Gowan et al., Reference Briggs-Gowan, Pollak, Grasso, Voss, Mian, Zobel and Pine2015; Cicchetti & Curtis, Reference Cicchetti and Curtis2005; Pollak & Tolley-Schell, Reference Pollak and Tolley-Schell2003; Shackman et al., Reference Shackman, Shackman and Pollak2007). The variability of this association with age is consistent with the interpretation that with increasing age comes an increasing capacity to regulate attention away from distressing emotional stimuli, overriding prepotent tendencies to orient toward potential threats (Morales et al., Reference Morales, Fu and Pérez-Edgar2016) that may arise as a result of being raised in a dangerous environment (McLaughlin & Lambert, Reference McLaughlin and Lambert2017). The maturation of attentional control with age interacts with maltreatment experiences, which make potential threats in the environment both more salient, drawing attention (Pollak, Reference Pollak2003), and potentially more distressing, which might motivate attentional avoidance (Kelly et al., Reference Kelly, Viding, Puetz, Palmer, Mechelli, Pingault and McCrory2015).
A greater tendency to engage in maladaptive emotion regulation strategies is associated with a higher “p” both concurrently and prospectively, indicating greater transdiagnostic risk for psychopathology. Prior evidence suggesting that emotion dysregulation is a transdiagnostic factor in psychopathology comes largely from meta-analyses and reviews of many studies (Aldao & Nolen-Hoeksema, Reference Aldao and Nolen-Hoeksema2012a, Reference Aldao and Nolen-Hoeksema2012b; Aldao et al., Reference Aldao, Nolen-Hoeksema and Schweizer2010) or studies that have examined emotion regulation difficulties as mechanisms underlying comorbidity or transitions between different forms of psychopathology (McLaughlin et al., Reference McLaughlin, Aldao, Wisco and Hilt2014; McLaughlin & Nolen-Hoeksema, Reference McLaughlin and Nolen-Hoeksema2011; Messman-Moore & Bhuptani, Reference Messman-Moore and Bhuptani2017). Here, we demonstrate that emotion regulation strategies contribute directly to general psychopathology, as captured by the p factor (Caspi et al., Reference Caspi, Houts, Belsky, Goldman-Mellor, Harrington, Israel and Moffitt2014).
The association between maladaptive emotion regulation strategies and “p” is also consistent with evidence that greater engagement in maladaptive strategies like expressive suppression and rumination is more strongly associated with multiple psychiatric disorders than lesser engagement in adaptive strategies like cognitive reappraisal (Aldao et al., Reference Aldao, Nolen-Hoeksema and Schweizer2010). As conceptual models of emotion regulation consider it to be so intertwined with the emotion process itself that it is difficult to distinguish between emotions and their regulation (Cole et al., Reference Cole, Hall, Hajal, Beauchaine and Hinshaw2017; Gross, Reference Gross and Gross2014; Gross & Thompson, Reference Gross, Thompson and Gross2007; Thompson, Reference Thompson1994), it is perhaps unsurprising that emotion dysregulation would be associated with global disruptions to emotion functioning, increasing risk for psychopathology transdiagnostically. Moreover, greater tendencies to engage in expressive suppression and rumination and greater emotional reactivity were strongly interrelated, suggesting multiple interrelated manifestations of emotion dysregulation that together contribute to greater risk for psychopathology. It may be that because increased emotional reactivity, expressive suppression, and rumination tend to reinforce one another, that their impact and potential to spiral into psychopathology are more pronounced then adaptive strategies like cognitive reappraisal. Rumination and emotional reactivity also predict “p” longitudinally, as does attention bias to threat. As suggested by the age-related patterns in the relation between attention bias and childhood maltreatment, a greater attention bias away from threat may indicate a greater capacity to utilize attentional avoidance, an antecedent-focused strategy to direct attention away from negative or distressing emotional stimuli, which may be protective against developing psychopathology.
Childhood maltreatment was associated with a higher “p.” This is unsurprising and consistent with past findings that (a) childhood maltreatment explains a substantial proportion of all mental disorders in the population (Green et al., Reference Green, McLaughlin, Berglund, Gruber, Sampson, Zaslavsky and Kessler2010; Kessler, Mickelson, & Williams, Reference Kessler, Mickelson and Williams1999; McLaughlin et al., Reference McLaughlin, Green, Gruber, Sampson, Zaslavsky and Kessler2012) and (b) that maltreatment in childhood and adolescence predicts higher “p” in adulthood in longitudinal studies (Caspi et al., Reference Caspi, Houts, Belsky, Goldman-Mellor, Harrington, Israel and Moffitt2014; Schaefer et al., Reference Schaefer, Moffitt, Arseneault, Danese, Fisher, Houts and Caspi2018). In the present study, however, greater engagement in rumination and heightened emotional reactivity emerged as key mechanisms linking maltreatment with general psychopathology. Even though childhood maltreatment was not associated with changes in “p” over time, it indirectly influenced increases in “p” through the combined effect of increased emotional reactivity and rumination. A similar pattern was observed for maltreatment severity, which did predict increases in “p” over time. Thus, while maltreatment exposure was associated with increased psychopathology, this risk may be highly stable over time. Nonetheless, the maladaptive emotion regulation processes engendered by maltreatment exposure continue to maintain and worsen psychopathology across development.
This study had several strengths, including a large sample, which was recruited to ensure sufficient variability in both age and maltreatment exposure to evaluate their independent effects and interactions, integration of multiple measures of maltreatment from both youth and parents, and longitudinal measures of psychopathology from both youth and parents. However, some limitations constrain interpretation and suggest directions for future research. While maltreated and nonmaltreated youth were matched on both age and gender, maltreated youth had significantly lower income and a higher proportion of racial/ethnic minority youth. These factors frequently co-occur, and all analyses controlled for income-to-needs ratio and racial minority status. However, potential confounds from this collinearity cannot be entirely ruled out. Future work in samples recruited specifically to examine interactions among violence exposure, race/ethnicity, and socioeconomic status could help distinguish the unique and shared influence of these variables on emotion regulation and psychopathology. Next, this study relies on youth self-reported emotion regulation. While the use of multiple reporters for quantifying both maltreatment and psychopathology symptoms allays some concerns about associations being attributable to shared method variance, work utilizing behavioral and ecological measures of emotion regulation would provide necessary additional support to our findings. In addition, the meaning of “p” is still a subject of considerable debate, with hypotheses ranging from poor impulse control over emotions to deficits in intellectual functioning to a simple tendency to report on oneself in a negative way (Caspi & Moffitt, Reference Caspi and Moffitt2018). However, there is robust evidence supporting the utility of “p” as a correlate of both theoretically and practically important risk factors and outcomes, suggesting that identification of the specific emotion regulation mechanisms that contribute to “p” may significantly advance clinical science (Caspi & Moffitt, Reference Caspi and Moffitt2018; Snyder & Hankin, Reference Snyder and Hankin2017).
Although questionnaires were read out loud for younger children in the study (8- to 10-year-olds) and those who had difficulty reading, the ERS and ERQ have not been validated for children under 12 (Nock et al., Reference Nock, Wedig, Holmberg and Hooley2008), and at the time the study started, we were not aware of the child and adolescent version of the ERQ with slightly simplified language (Gullone & Taffe, Reference Gullone and Taffe2012). Finally, while associations between attention bias and psychopathology, especially anxiety, are quite consistent across studies (Bar-Haim, Lamy, Pergamin, Bakermans-Kranenburg, & Van IJzendoorn, Reference Bar-Haim, Lamy, Pergamin, Bakermans-Kranenburg and Van Ijzendoorn2007; Dudeney et al., Reference Dudeney, Sharpe and Hunt2015), attention biases as measured by the dot-probe task demonstrate low test–retest reliability (Brown et al., Reference Brown, Eley, Broeren, MacLeod, Rinck, Hadwin and Lester2014; Chapman, Devue, & Grimshaw, Reference Chapman, Devue and Grimshaw2017; Waechter, Nelson, Wright, Hyatt, & Oakman, Reference Waechter, Nelson, Wright, Hyatt and Oakman2014), calling into question its utility as a between-subjects measure of emotion regulation. Further validation by other indices of attention like eye tracking and event-related potentials would therefore provide necessary support to our findings related to attention biases and their implications.
Greater emotional reactivity and greater engagement in maladaptive emotion regulation strategies, in particular rumination, are transdiagnostic mechanisms linking childhood maltreatment with psychopathology in middle childhood and adolescence, and which maintain and exacerbate psychopathology symptoms over time. Attention biases away from threat predict decreased psychopathology over time. Maltreatment contributes to maladaptive patterns of emotion regulation in the form of attention biases toward threat in children and younger adolescents, but with more adaptive patterns in older adolescents, who may have a greater capacity to redirect their attention away from threatening and distressing emotional cues. These results suggest that therapies and interventions aimed at disrupting patterns of rumination in youth exposed to childhood maltreatment have the potential to reduce risk for multiple forms of psychopathology in adolescence, and that attention bias modification may also reduce risk for psychopathology, but its efficacy might be restricted to older adolescence and young adults who may have a greater capacity for regulating their attention.
Financial support
This research was funded by the National Institute of Mental Health Grant R01-MH103291 (awarded to K.A.M.) and Grant K01MH116325 (awarded to A.B.M.), an Early Career Research Fellowship from the Jacobs Foundation (to K.A.M.), and a OneMind Institute Rising Star Award (to K.A.M.).







