


The quality and organization of an infant's response to standardized episodes of separation from, and reunion with, their primary caregiver in socially stressful situations involving the presence of a stranger is recognized as an important index of the underlying quality of the early caregiver–child relationship (i.e., the Strange Situation Procedure; SSP; Ainsworth, Blehar, Waters, & Wall, Reference Ainsworth, Blehar, Waters and Wall1978). When an infant (or young child) shows normative patterns of distress following separation from his/her caregiver and is readily soothed by the caregiver on reunion and returns to play, we infer the existence of a secure selective attachment (Main & Solomon, Reference Main, Solomon, Brazelton, Berry and Yogman1986, Reference Main, Solomon, Greenberg, Cicchetti and Cummings1990). While the majority of infants conform to this pattern, deviations do occur. These encompass a number of distinctive patterns of insecurity and disorganization. Insecure-avoidant attachment is marked by apparent “independence” from the caregiver and diminished or lack of avoidance of contact with the caregiver on reunion. Children with Insecure ambivalent/resistant attachment patterns tend to exhibit a combination of dependent and resistant behaviors toward their caregiver. Disorganized attachment, which is often seen following significant disturbances of the early parent–child relationship, involves contradictory attachment behaviors, freezing/stilling, and/or fear of the caregiver (Main & Solomon, Reference Main, Solomon, Greenberg, Cicchetti and Cummings1990).
Attachment theorists consider that secure selective attachment promotes psychological health (Bowlby, Reference Bowlby1982/1969). This is because such attachments are thought to promote resilience by establishing a sense of personal agency (i.e., positive internal working model) and create a template for, and a network of, intimate social relationships that can buffer the negative effects of external threats (Boldt, Kochanska, & Jonas, Reference Boldt, Kochanska and Jonas2017), the benefits of which are thought to cascade across the life span (e.g., Fransson, Granqvist, Marciszko, Hagekull, & Bohlin, Reference Fransson, Granqvist, Marciszko, Hagekull and Bohlin2016). Consistent with this formulation, a recent meta-analysis suggests that early secure attachment in infancy is associated with lower levels of psychological problems later in childhood (Groh et al., Reference Groh, Fearon, Bakermans-Kranenburg, van IJzendoorn, Steele and Roisman2014). Negative effects of insecure attachment are small to moderate in size, larger for externalizing than for internalizing problems, and most likely to occur as a consequence of ambivalent/resistant and disorganized attachment patterns (Green & Goldwyn, Reference Green and Goldwyn2002; Groh et al., Reference Groh, Fearon, Bakermans-Kranenburg, van IJzendoorn, Steele and Roisman2014).
Attachments are hypothesized to be formed through the reciprocity that naturally develops during interactions within caregiver–child dyads in the first year, or so, of life (Belsky & Rovine, Reference Belsky and Rovine1988; Lamb, Reference Lamb1977) as carers respond to fulfill their infant's biopsychological needs (Wolff & van IJzendoorn, Reference Wolff and van IJzendoorn1997). Historically, it has been believed (a view perhaps particularly influenced by nonhuman primate research) that this period represents a biologically delimited, developmentally sensitive, period when both carer and infant are preprogrammed to develop selective attachments (Bretherton, Reference Bretherton2013). Contradicting this view, recent studies demonstrate that children adopted or fostered out of severely depriving institutional settings after this sensitive period has ended can still go on to form selective attachments with adoptive or foster parents (Carlson, Hostinar, Mliner, & Gunnar, Reference Carlson, Hostinar, Mliner and Gunnar2014; Oliveira, Fearon, Belsky, Fachada, & Soares, Reference Oliveira, Fearon, Belsky, Fachada and Soares2015; Smyke, Zeanah, Fox, Nelson, & Guthrie, Reference Smyke, Zeanah, Fox, Nelson and Guthrie2010). Although in many cases these attachments bear the hallmarks of security, for a substantial minority of previously institutionalized children, especially those exposed to prolonged periods of deprivation, attachment relations with adoptive parents appear to be disrupted and dysfunctional based on their response to separation and reunion whether assessed by the SSP (Kreppner, Rutter, Marvin, O'Connor, & Sonuga-Barke, Reference Kreppner, Rutter, Marvin, O'Connor and Sonuga-Barke2011; O'Connor et al., Reference O'Connor, Marvin, Rutter, Olrick and Britner2003) or semistructured interviews with parents (Smyke, Dumitrescu, & Zeanah, Reference Smyke, Dumitrescu and Zeanah2002).
As part of the English and Romanian Adoptees study (ERA) we used a home-based version of the SSP modified for preschoolers, the Modified Separation–Reunion Strange Situation Procedure (MSSP), to study the attachment status of adopted 4-year-old children previously exposed to extremely severe global institutional deprivation (O'Connor et al., Reference O'Connor, Marvin, Rutter, Olrick and Britner2003). Thirty-three percent of those children exposed to between 6 and 24 months of deprivation were coded as secure, somewhat lower than in a comparison group of UK adoptees (55%) placed in the first 6 months of life from nondepriving backgrounds. Of the remainder, a small number displayed classical patterns of attachment insecurity (ambivalent or avoidant 5%) or disorganization (8%). Strikingly, a far larger proportion of adoptees (54%) displayed a distinctive pattern of immature and attention-seeking behavior (emotionally dysregulated, chaotic, overly solicitous of the stranger, not looking for help from the parent, and showing excess of “on stage” or “goofy” behavior) across separation and reunion episodes (O'Connor et al., Reference O'Connor, Marvin, Rutter, Olrick and Britner2003). Because this affectively dysregulated pattern was not readily encompassed within the classical framework describing attachment insecurity and disorganization, it was coded as “insecure-other” (INS/OTH) to mark its distinctiveness from typical patterns of insecurity (O'Connor et al., Reference O'Connor, Marvin, Rutter, Olrick and Britner2003). This INS/OTH variant is usually rare in nondeprived samples but like the other INS/OTH categories (avoidant/dependent patterns, disengaged/depressive, and Inhibited/fearful), it is indicative of a disrupted parent–child relationship (Cassidy & Shaver, Reference Cassidy and Shaver2002).
The ERA sample has now entered young adulthood (Sonuga-Barke et al., Reference Sonuga-Barke, Kennedy, Kumsta, Knights, Golm, Rutter and Kreppner2017). Longitudinal analyses demonstrated a link between extended deprivation (i.e., over 6 months) and a distinctive, early onset and persistent pattern of impairment across a number of overlapping domains: disinhibited social engagement (Kennedy et al., Reference Kennedy, Kreppner, Knights, Kumsta, Maughan, Golm and Sonuga-Barke2017), autistic-like traits (referred to as quasi-autism; Kreppner et al., Reference Kreppner, Kumsta, Rutter, Beckett, Castle, Stevens and Sonuga-Barke2010), and symptoms of inattention/overactivity (Kennedy et al., Reference Kennedy, Kreppner, Knights, Kumsta, Maughan, Golm and Sonuga-Barke2016). It also had an initial devastating impact on cognition including impairments that were profound at entry but have recovered over time (Beckett, Castle, Rutter, & Sonuga-Barke, Reference Beckett, Castle, Rutter and Sonuga-Barke2010; Sonuga-Barke et al., Reference Sonuga-Barke, Kennedy, Kumsta, Knights, Golm, Rutter and Kreppner2017). In addition, while more general conduct and emotional problems were surprisingly absent in childhood, emotional problems displayed a striking increase between childhood and adulthood (Sonuga-Barke et al., Reference Sonuga-Barke, Kennedy, Kumsta, Knights, Golm, Rutter and Kreppner2017). A question remains, however, regarding whether the disrupted attachment relationship suggested by their pattern of separation and reunion responses displayed during the MSSP at age 4 years have impacted on the Romanian adoptees’ subsequent development.
To date, there have been few systematic longitudinal examinations of children's attachment behaviors displayed in relation to their adoptive parent and whether these are related to adoptees’ later development. Two analyses within the Leiden Longitudinal study found an effect of the security and disorganization of selective attachments on social development and cognition at age 7 years in a sample of children adopted before the age of 6 months (Stams, Juffer, van IJzendoorn, & Hoksbergen, Reference Stams, Juffer, van IJzendoorn and Hoksbergen2001). A follow-up into adolescence found only indirect effects of attachment security on social development (Jaffari-Bimmel, Juffer, van IJzendoorn, Bakermans-Kranenburg, & Mooijaart, Reference Jaffari-Bimmel, Juffer, van Ijzendoorn, Bakermans-Kranenburg and Mooijaart2006). McGoron et al. (Reference McGoron, Gleason, Smyke, Drury, Nelson, Gregas and Zeanah2012) provided a more direct test of the importance of attachment security in improving developmental outcomes in a high-risk sample of fostered children taking part in the Bucharest Early Intervention Project. They found that attachment insecurity assessed at 42 months was associated with attachment disorders and internalizing and externalizing problems 12 months later. In a follow-up analysis, the authors found that foster care improved attachment security and reduced internalizing problems in girls but not boys, with attachment security fully mediating this pathway (McLaughlin, Zeanah, Fox, & Nelson, Reference McLaughlin, Zeanah, Fox and Nelson2012). In their latest follow-up up to age 12 years, attachment security predicted a normative IQ trajectory (Almas, Degnan, Nelson, Zeanah, & Fox, Reference Almas, Degnan, Nelson, Zeanah and Fox2016). In these analyses preexisting externalizing and internalizing problems at age 42 months were not controlled statistically. As these may have already been elevated at that age, it leaves open the possibility that it was the child's preexisting behavior that determined attachment status rather than the other way around.
The main goal of the current paper, therefore, was to use longitudinal data to examine the extent to which INS/OTH status at age 4 years predicted deprivation-related developmental trajectories from childhood to adulthood in the ERA sample. To do this, we contrasted adoptees who at age 4 years were coded as displaying the INS/OTH pattern and had previously experienced prolonged deprivation with adoptees given any other classification (secure, insecure ambivalent, insecure avoidant, or disorganized). We predicted that in individuals exposed to extended deprivation, who we already know are at elevated risk for a range of mental health and neurodevelopmental conditions (Sonuga-Barke et al., Reference Sonuga-Barke, Kennedy, Kumsta, Knights, Golm, Rutter and Kreppner2017), this disturbed and distinctive pattern of MSSP behavior would be associated with more negative neurodevelopmental and mental health outcomes compared to those with more normative attachment patterns. This was based on the hypotheses that INS/OTH would reduce the chance for parents to effectively either (a) respond to preexisting deprivation-related impairment in their children such as attention-deficit/hyperactivity disorder or autism symptoms to aid recovery or (b) help buffer new stressors that may occur during life (e.g., between adolescence and adulthood) and so be linked to the emergence of emotional problems such as depression and anxiety. We therefore predicted that because of these effects, INS/OTH would also be linked to reduced quality of life and problems with daily functioning in adult life (i.e., impairment). Alternatively, INS/OTH may not be causally related to such negative developmental trajectories. Rather it, and its associated negative outcomes, may simply be two correlated characteristics of children with early emerging deprivation-related impairment. To examine this, our analysis controlled for characteristics at the time of entry to the United Kingdom and at age 4 years.
Method
Participants
Ninety-seven Romanian (53% females), and 49 UK adoptees (35% females, no deprivation history) and their adoptive families were included in the longitudinal analysis. The Romanian group was restricted to the 40% of the total sample who entered the United Kingdom before 24 months and were therefore young enough to be included in the age 4 assessment wave when we were confident the preschool version of the SSP was successfully implemented. Young adult outcome data were available for 65 Romanian adoptees and 38 UK adoptive controls. The average age at young adult assessment was 23.6 (UK adoptees) and 23.7 years (Romanian adoptees). A comparison of age 4 characteristics of those lost to follow-up before young adulthood (n = 37) and those who remained in the study (n = 121) provided no evidence of selective attrition in terms of sex of child, age, IQ, or levels of autism, inattention/overactivity, disinhibited social engagement, and emotional problems (data available from authors).
Measures
MSSP at age 4 years
This procedure was designed, as was the original SSP, to mildly stress the child's attachment system (see O'Connor et al., Reference O'Connor, Marvin, Rutter, Olrick and Britner2003). The sequence of episodes was as follows. There was a 10-min period of semistructured play between the child and parent using the Etch-a-Sketch toy. This involved parent and child co-operating, by taking turns, to produce a drawing. In a standardized manner, the experimenter/stranger then took the child to another room on their own and recorded the child's physical measurements (height and weight) during which time the experimenter/stranger was inevitably in close proximity to the child. The child was then taken back to the parent for a 3-min reunion. The parent then left the room and a standardized cognitive test, lasting 30 min, was administered by the experimenter (i.e., stranger). The adoptive parent then rejoined the child for 3 min. During each reunion episode, the experimenter/stranger remained in the room in order to operate the camera but remained quiet and noninteractive.
Participants were assigned an attachment classification on the basis of proximity or contact seeking, body orientation, speech patterns, gaze, affect, and the manner in which the parent and child negotiated separation using a modified version of the MacArthur system for coding attachment in preschool-aged children (Cassidy & Marvin, Reference Cassidy and Marvin1992). Coding was made from the video tapes “blind” to group status by researchers in the ERA team. Interrater reliability was acceptable (κ = .68, p < .001), exact agreement was 76%, and disagreements were resolved by conferencing (see O'Connor et al., Reference O'Connor, Marvin, Rutter, Olrick and Britner2003; the percentage of attachment classifications in each group is presented in Appendix A).
Neurodevelopmental and mental health outcomes measured at ages 4, 6, 11, and 15 years and in young adulthood
The current analysis included only those outcome domains shown previously to be associated with extended deprivation in the ERA study (Sonuga-Barke et al., Reference Sonuga-Barke, Kennedy, Kumsta, Knights, Golm, Rutter and Kreppner2017). Therefore, conduct problems were not included in the analysis. For the longitudinal analysis, we followed the same measurement strategy as in Sonuga-Barke et al. (Reference Sonuga-Barke, Kennedy, Kumsta, Knights, Golm, Rutter and Kreppner2017) using different developmentally appropriate assessment instruments at each assessment age (ages, 4, 6, 11, 15, and young adult [23–25] follow-ups) to provide equivalent ratings based on three core symptom domains reflecting the same clinical constructs. Inattention/overactivity combined parent-rated hyperactivity, sustained attention, and distractibility domains, measured using items from the Revised Rutter scale (Elander & Rutter, Reference Elander and Rutter1996) at ages 6 and 11 years, the Strengths and Difficulties Questionnaire (Goodman, Reference Goodman1997) at age 15 years, and an adaptation of the Comprehensive Behavior Rating Scale (CBRS; Conners, Pitkanen, & Rzepa, Reference Conners, Pitkanen and Rzepa2011) in young adulthood. The same questionnaires were used to measure emotional problems (depressed mood, worry, and social anxiety). For the Rutter scales and Strengths and Difficulties Questionnaire domains, a symptom was considered endorsed when a rating of 2 (certainly applies) was made (0–2 scale). For the CBRS, the equivalent rating was often/very often (2/3; 0–3 scale). Researcher ratings of parents’ responses to age-appropriate variants of three interview questions (“too friendly,” “showing inappropriate intrusiveness,” and “unaware of social boundaries”) were used to derive the measure of disinhibited social engagement. A rating of definite evidence of disinhibition (2 on a 0–2 scale) represented a positive endorsement (Kreppner et al., Reference Kreppner, Kumsta, Rutter, Beckett, Castle, Stevens and Sonuga-Barke2010). Autism symptom domains (social reciprocal interaction, communication and repetitive, and stereotyped behaviors) were assessed using 15 items from the parent-report Social Communication Questionnaire (SCQ; Rutter, Bailey, & Lord, Reference Rutter, Bailey and Lord2003; see Sonuga-Barke et al., Reference Sonuga-Barke, Kennedy, Kumsta, Knights, Golm, Rutter and Kreppner2017, for evidence of the validity of this approach) deemed to be developmentally relevant at all ages. Each symptom domain consisted of five items rated as either absent (0) or present (1). Scores were log-transformed to reduce skew in the current analysis. IQ was based on age-appropriate standardized IQ assessments: the McCarthy Scales of Children's Abilities General Cognitive Index (McCarthy, Reference McCarthy1972) at age 6, the short form of the Wechsler Intelligence Scale for Children (block design, object assembly, vocabulary, and similarities) at ages 11 and 15 (Wechsler, Reference Wechsler1992), and block design and vocabulary subscales from the short form of the Wechsler Abbreviated Scale of Intelligence in adulthood (Wechsler, Reference Wechsler1999). General Cognitive Index values were adjusted to account for apparent inflation of scores since the norms were established in 1970 (Beckett et al., Reference Beckett, Maughan, Rutter, Castle, Colvert, Groothues and Sonuga-Barke2006).
Measures taken in young adulthood only
Young adult depression and generalized anxiety disorder symptoms were assessed using the Young Adult Psychiatric Assessment (Angold et al., Reference Angold, Cox, Prendergast, Rutter, Simonoff, Costello and Ascher1999) conducted via face-to-face assessments with the young adults themselves. Trained coders rated the presence of symptoms within the last 3 months, based on DSM-IV criteria. Following this, we calculated symptom count scores. Quality of life was measured using the self-completed Satisfaction with Life Scale (Diener, Emmons, Larsen, & Griffin, Reference Diener, Emmons, Larsen and Griffin1985). This scale is rated from 1 to 5, with higher scores indicating greater satisfaction with life. This scale demonstrated high internal consistency (α = .90). General daily functioning was measured using the parent-rated impairment scale on the CBRS (Conners et al., Reference Conners, Pitkanen and Rzepa2011). This was a sum score of three impairment items (social, work, and at home), each scored between 0 and 4, with higher scores indicating a greater degree of impairment.
Child characteristics at the time of entry to the United Kingdom
Measures of the child's developmental status at entry to the adoptive home were based on parents’ retrospective accounts made at the age 4 assessment (O'Connor, Bredenkamp, & Rutter, Reference O'Connor, Bredenkamp and Rutter1999). Individual items included levels of inappropriate rocking behaviors, difficulties eating solids, and self-injurious behaviors. There was also an assessment of the child's attempts to imitate at least two words. All items were coded 0 for absent or 1 for present. A developmental quotient for the child at entry was also calculated using the Denver scale (Frankenburg, van Doornick, Liddell, & Dick, Reference Frankenburg, van Doornick, Liddell and Dick1986; see Rutter & English and Romanian Adoption Adoptees Study Team, Reference Rutter1998, for evidence of the validity of this report). The presence of subnutrition, defined as weighing 1.5 SD below UK norms, was also recorded. Socioeconomic status (SES) was based on parents’ occupation at the age 15 follow-up (Rutter, Sonuga-Barke, & Castle, Reference Rutter, Sonuga-Barke and Castle2010). Families were assigned to high (skilled, managerial/technical, or professional) and low (manual or unskilled) SES groups in line with the Registrar General's classification (General Register Office, 1971). Data for the UK group were not collected on subnourishment, developmental status, or language at entry.
Procedure
Ethical approval was received from the King´s College London and the University of Southampton Research Ethics Committees. At each wave, all participants and/or their parents/carers gave written informed consent or verbal assent (where developmentally appropriate). Assessments took place in participants’ homes. Some questionnaires were completed online or returned by mail at the young adult follow-up.
Statistical analysis
All assessed children were assigned to attachment status groupings (INS/OTH(+) or INS/OTH(–), including all other standard A, B, C, and D codings) based on the MSSP. As in previous analyses, we also divided the Romanian adoptees into two deprivation status groups based on whether they had experienced more (Rom>6) or less than 6 months of time in the institutions; this latter group was combined with the UK adoptees to form a low deprivation group (LoDep). The LoDep group consisted of 107 individuals at age 4 (UK n = 49; Rom<6 n = 58) and 86 in young adulthood (UK n = 42, Rom<6 n = 4). The Rom>6 group had 39 members at age 4 and 29 at young adult follow-up. These groupings (Rom>6 and LoDep) have been repeatedly validated (see Kreppner et al., Reference Kreppner, Rutter, Beckett, Castle, Colvert, Groothues and Sonuga-Barke2007; Sonuga-Barke et al., Reference Sonuga-Barke, Kennedy, Kumsta, Knights, Golm, Rutter and Kreppner2017), based on (a) a step increase in risk for those with more than 6 months of deprivation across multiple outcomes and (b) similarly low rates of problems seen in the UK adoptees and the Rom<6 groups.
First, we conducted analyses to look at differences between groups that existed at or before the age 4 MSSP assessment. Chi square (χ2) analyses were used to examine differences due to attachment and deprivation status at the time the Romanian adoptees entered the United Kingdom. These analyses were restricted to Rom<6 and Rom>6 groups as no data for the UK adoptees was available. To investigate age 4 differences in deprivation specific problems (see Appendix B), we derived Sidak-corrected planned follow-up analyses from mixed-effects models, with age at assessment fixed at 4 years.
Second, we employed mixed-effects regression models to conduct longitudinal analyses. Assessment age wave (4, 6, 11, 15, and young adulthood) was a within-subject random effect. Deprivation (LoDep vs. Rom>6) and attachment status (INS/OTH(+) vs. INS/OTH(–)) were between-subject variables. The dependent variables were disinhibited social engagement, autism symptoms, IQ, inattention/overactivity, and emotional symptoms. Where a significant interaction between Assessment Age × Deprivation Status × Attachment Status was found, planned supplementary analyses were conducted to isolate the source of this effect. In particular, we tested whether there was an effect of attachment status on trajectories in the Rom>6 group using a two-way mixed model with Assessment Age × Attachment Status as independent variables. This was followed up by an analysis of simple main effects of attachment status at each age in the Rom>6 group.
Third, we tested whether any effects of attachment status on developmental trajectories found in the Rom>6 could be explained by differences between the groups already apparent at the time the Romanian adoptees entered the United Kingdom or at age 4 when the MSSP was completed. To do this, models were adjusted for any age at entry or age 4 outcomes found to differentiate the INS/OTH(+) from INS/OTH(–) groups.
Fourth, we also conducted a series of cross-sectional two-way analyses of variance on data collected only at the young adult assessment with deprivation status and attachment status as the independent variable and measures of depression and generalized anxiety disorder symptoms, quality of life, and impairment as the dependent variables.
All analyses were performed using SPSS v25 (IBM Corp., 2017). To limit the risk of interpreting false-positive findings, α was set at .01.
Results
Group differences at entry to United Kingdom and 4 years of age
Twenty-four (22%) of the LoDep (UK: 8 [16%], Rom<6: 16 [27.6%]; p = .16) and 21 (54%) of the Rom>6 months group were classified as INS/OTH at age 4, χ2 (1) = 13.23; p < .001. Table 1 presents characteristics at age of entry as a function of attachment status in the Rom<6 and Rom>6 groups. Rom>6 groups in general were rated as having lower developmental status than the Rom<6. INS/OTH(+) was associated with higher SES (Table 1). Turning to the age 4 data, there was a tendency for the Rom>6 INS/OTH(+) group to have more problems across domains (cf. Figure 1); however, these differences were consistently nonsignificant (ps > .057; see Appendix B). The exception being in relation to more general cognitive impairment (Rom>6 INS/OTH(+) vs. Rom>6 INS/OTH(–); p = .003, Cohen's d = 1.02).
Table 1. Background differences and characteristics at the time of adoption

Note: LoDep, UK adoptees and Romanian adoptees who experienced less than 6 months deprivation. Rom>6, Romanian adoptees who experienced more than 6 months deprivation. INS/OTH(+), adoptees with insecure other attachment classification at age 4. INS/OTH(–), adoptees with other attachment classifications. Dep, deprivation. Attach status, whether INS/OTH(+) or INS/OTH(–). All degrees of freedom rounded to full digit. Adjustments have been made for violations of equal variance assumptions. Subnourished, proportion with weight 1.5 SD below UK norms. Rocking, self-injury, difficulty eating based on adoptive parent retrospective accounts taken at age 4 interview. Developmental status based on parent ratings. Language, parent report of child attempting to imitate language. Effect size estimates, d = Cohen's d. ϕ = phi coefficient.

Figure 1. Estimated marginal mean symptom domain scores over time for IQ, autism, disinhibited social engagement, inattention/overactivity, and emotional symptoms as a function of deprivation and attachment status. Estimated marginal means were derived for each outcome separately via mixed models using the EMMEANS command in SPSS version 25.
Developmental trajectories
Figure 1 charts the developmental trajectories for symptoms of autism, disinhibited social engagement, inattention/overactivity, emotional problems, and IQ as a function of the presence INS/OTH in the LoDep and Rom>6 groups. Table 2 shows results of tests for main effects and the three-way interaction of the mixed models. There was a main effect of deprivation status on disinhibited social engagement and IQ and a main effect of attachment status on IQ (ps < .008). There were also significant three-way interactions (Assessment Age × Deprivation Status × Attachment Status) for autism symptoms and emotional problems, suggesting differences between the developmental trajectories of the four groups. Planned follow-up analyses for these revealed a significant interaction of Assessment Age × Attachment Status in the Rom>6 group for autism spectrum disorder (ASD; F = 4.22; p < .05) but not for emotional problems (F = 0.001; p = .99). The significant interaction for ASD was due to an increasingly significant difference between INS/OTH(+) and INS/OTH(–) in the Rom>6 group (age 4 mean diff = –0.07; p = .57, d = 0.18; age 6 mean diff = –0.12; p = .32, d = 0.32; age 11 mean diff = –0.22; p = .043, d = 0.67; age 15 mean diff = –0.31; p = .013, d = 0.85; young adult mean diff = –0.48; p = .009, d = 0.90). In order to examine whether this differential pattern of persistence was specific to one or more autism subdomains, we conducted a supplementary analysis using the scores for the social reciprocal interaction, communication, and repetitive and stereotyped behaviors subscales as the dependent variables (Figure 2). The interaction between attachment status and assessment age was significant only for the communication score (F = 8.40; p = .008; other ps >.29). Although, the relevant three-way interaction was not significant at α < .01 there was a striking pattern of IQ catch up in the INS/OTH(+) Rom>6 group from a very low base (age 4 mean diff = 15.53; p = .003, d = 1.02; age 6 mean diff = 13.47; p = .004, d = 0.98; age 11 mean diff = 8.30; p = .022, d = 0.77; age 15 mean diff = 4.17; p = .20, d = 0.42; young adult mean diff = –4.10; p = .32, d = 0.32).
Table 2. The interaction between age, deprivation, and attachment status (mixed-effect models)

Note: Rom>6, Romanian adoptees who experienced more than 6 months deprivation. Dep status, deprivation status (whether LoDep or Rom>6). Attach, attachment status (whether INS/OTH(+) or INS/OTH(–)). Three-way interaction, Deprivation Status × Attachment Status × Age. Autism symptoms based on parent-rated Social Communication Questionnaire. Disinhibited social engagement symptoms based on parent-rated three-item interview. Inattention/overactivity symptoms and emotional problems based on parent-rated Rutter scale, Strengths and Difficulties Questionnaire, or Comprehensive Behavior Rating Scale depending on age of assessment. IQ based on McCarthy or Wechsler scales. aTwo-way interactions were included in the model, but results are not shown here to reduce complexity.

Figure 2. Estimated marginal means for comparing Rom>6 INS/OTH(–) and INS/OTH(+) for the three subscales of the Social Communication Questionnaire. *p < .05.
In the planned follow-up analyses to see if the persistence of ASD symptoms in the INS/OTH+ Rom>6 group could be accounted for by differences seen prior to or at age 4, we added age 4 IQ into the model. The Assessment Age × Attachment Status interaction dropped to nonsignificant levels (F = 4.05, p = .053), with differences between INS/OTH(+) and INS/OTH(–) at each age also dropping to nonsignificant levels (p age4 = .64; p age6 = .89; p age11 = .40; p age15 = .14; p young adult = .053).
Young adulthood (cross-sectional comparisons)
Table 3 reports data for the cross-sectional comparison of the outcomes in young adulthood. There was a main effect of both deprivation status and attachment status on impairment. There was also a nominal difference in impairment between INS/OTH(+) and INS/OTH(–) in the Rom>6 group (p = .018). There was a similar trend for depression (p = .050).
Table 3. Young adulthood outcomes
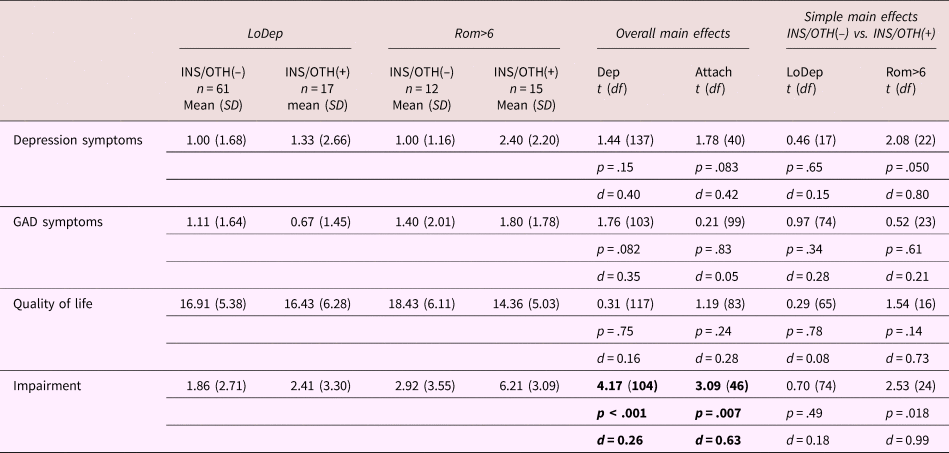
Note: LoDep, UK adoptees and Romanian adoptees who experienced less than 6 months deprivation. Rom>6, Romanian adoptees who experienced more than 6 months deprivation. INS/OTH(–) adoptees with other attachment classifications. INS/OTH(+), adoptees with insecure other attachment classification at age 4. Dep, deprivation status. Attach, attachment status (whether INS/OTH(+) or INS/OTH(–)). Depression based on self-report Young Adult Psychiatric Assessment depression symptom score. Generalized anxiety disorder based on self-report Young Adult Psychiatric Assessment generalized anxiety disorder symptom score. Quality of life based on self-report Satisfaction with Life Scale. Impairment based on Comprehensive Behavior Rating Scale impairment scale sum score. d = Cohen's d.
Discussion
Extended early severe institutional deprivation is associated with negative young adult outcomes across a range of neurodevelopmental domains (Sonuga-Barke et al., Reference Sonuga-Barke, Kennedy, Kumsta, Knights, Golm, Rutter and Kreppner2017). We addressed the question of whether the dysfunctional adoptee–adopter relationship signified by the INS/OTH classification of behaviors observed in the MSSP at age 4 was associated with adoptees’ developmental trajectories based on the hypothesis that they may hinder recovery of existing problems or contribute to the onset of new ones. We used observational data from the MSSP gathered when the children were 4 years old. In the MSSP, a substantial minority of Romanian adoptees displayed the dysfunctional INS/OTH(+) pattern marked by chaotic approach and avoidance of the parent, over solicitousness of the stranger, and an excess of immature attention seeking, “on stage,” or “goofy” behavior. This was especially common in those individuals who spent over 6 months in the institutions. Although significantly lower than in the Rom>6 group, there was evidence of INS/OTH in both the Rom<6 and the UK groups. This provides some of the first evidence of the relevance of INS/OTH in nondeprived samples; however, in contrast to the Rom>6 group, INS/OTH in these groups was not associated with worse developmental outcomes in the LoDep group.
With regard to developmental trajectories in the Rom>6 group, the most striking finding involved the remission of ASD symptoms in the Rom>6 INS/OTH(–) group compared to the strongly persistent pattern in the Rom>6 INS/OTH(+) group. Initial reports from the ERA study highlighted quasi-autism as a core distinctive deprivation-specific sign of early extreme institutional deprivation (Rutter et al., Reference Rutter1998, Reference Rutter, Sonuga-Barke and Castle2010). After breaking down the analysis by the autism symptom domain as measured by the SCQ, we found that this effect was driven most by an offset in problems in the communication domain (i.e., “odd speech,” ”lack of to-and-fro conversation,” “socially inappropriate speech,” “difficulty with pronouns,” and “made up words or phrases”). It is interesting that the pattern of remission in the Rom>6 INS/OTH(–) group did not extend to the social reciprocal interaction domain in the current sample of institutionally deprived children. These two elements, previously separated in DSM-IV, are now combined in DSM-5 in recognition of their highly overlapping nature in clinically typical children with autism (McPartland, Reichow, & Volkmar, Reference McPartland, Reichow and Volkmar2012). In this regard, the current results suggest that autistic patterns of behavior arising as a result of extreme early adversity may have a distinctive underlying structure with the previous tripartite structure still being relevant. The prefix quasi– was originally added to definitions in the ERA study partly to distinguish deprivation-related autism from more putative genetically based autism variants. The results of the current study highlight another potentially distinctive feature of ASD symptoms following deprivation, a developmental relationship between INS/OTH and symptom persistence. Previous research has established no evidence for attachment disturbances in idiopathic autism once intellectual disability is controlled for (Rutgers, Bakermans-Kranenburg, & van IJzendoorn, Reference Rutgers, Bakermans-Kranenburg, van Ijzendoorn and van Berckelaer-Onnes2004; Teague, Gray, Tonge, & Newman, Reference Teague, Gray, Tonge and Newman2017). There is also no prior evidence that a secure attachment is related to developmental trajectories of autism symptoms in typical clinical cases across time (Mayes, Calhoun, Waschbuscch, & Baweja, Reference Mayes, Calhoun, Waschbusch and Baweja2017).
While the lack of impact of dysfunctional attachment relations in more “typical” groups with clinical autism diagnoses is noteworthy, it is crucial that we establish their relevance to autism symptoms following institutional deprivation. There are two possible ways to think about the different developmental trajectories for ASD symptoms in the Rom>6 INS/OTH(+) and Rom>6 INS/OTH(–) groups. First, it is possible that the dysfunctional relationship suggested by the INS/OTH designation undermines the parents’ ability to work effectively with their child with preexisting autistic problems to improve outcomes. From this perspective, the specific lack of remission of problems of social communicative intent, seen when the SCQ was broken down by subscale, might be interpreted as a domain of impairment particularly open to parental influence in the context of well-functioning attachment relations, but not where such relations are not established as in the Rom>6 INS/OTH(+) group. However, for this to be plausible, a similar pattern in the other “social” autism domain would be expected (i.e., social reciprocal interaction), unless these effects are specifically tied to the linguistically sophisticated nature of the adoptive families. However, the significantly lower SES in the INS/OTH(–) group does not seem consistent with such an interpretation.
The second possibility is that there are two types of deprivation-related ASD symptoms established in early childhood (here measured at age 4 years), one which is developmentally more benign and remitting than the other, especially with regard to communication problems. In this case, the pattern of dysregulated behavior coded as INS/OTH in the MSSP could be considered an early marker of a poor outcome rather than its cause. It is interesting to reflect on what distinctive features of the Rom>6 INS/OTH(+) compared to the Rom>6 INS/OTH(–) might predict these different trajectories. Most striking, in this regard, was the much higher levels of cognitive impairment at age 4 in the Rom INS/OTH(+) group. This leads us to consider the notion that preexisting cognitive deficits might have inhibited the formation of normative adoptee–adopter attachments. However, this interpretation is complicated by two things. First, that the severe intellectual impairment seen at age 4 in the Rom>6 INS/OTH(+) group remitted over time (as IQ improved in the deprived group generally), an effect not mirrored for ASD symptoms. Second, that adding age 4 IQ as a factor to the mixed models in the planned follow-up analysis, although reducing it to nonsignificant levels, did not completely remove the effect of attachment status on ASD symptoms in the Rom>6 group.
Some elements of the behavior displayed by children designated as INS/OTH in the MSSP, such as the tendency to be oversolicitous of reactions from stranger and undifferentiated in response to the parent, overlapped with the concept of disinhibited social engagement disorder in DSM-5 (American Psychiatric Association, 2013). While previously disinhibited social engagement was regarded as a disinhibited form of reactive attachment disorder, indicating a disturbed relationship to the adoptive parent (O'Connor et al., Reference O'Connor, Marvin, Rutter, Olrick and Britner1999), the definition now primarily focuses on indiscriminate social approach and intimacy with strangers (which itself is very common in the ERA sample). The current analyses revealed a significant overlap between MSSP INS/OTH and disinhibited social engagement assessed from parental report across developmental stages. Disinhibited social engagement was significantly elevated at age 4 in the Rom>6 INS/OTH(+) group compared to the Rom>6 INS/OTH(–) group, a difference that became somewhat more marked over time through to young adulthood. The question is then whether, while sharing some elements, INS/OTH and disinhibited social engagement essentially measure the same thing or are similar constructs measured using different methods. In order to compare the developmental significance of INS/OTH and disinhibited social engagement, we conducted a series of supplementary analyses where we compared the developmental trajectories of children with and without disinhibited social engagement at age 4. If the disinhibited social engagement and INS/OTH concepts were equivalent (i.e., captured the same or highly overlapping phenotypes), then we would expect similar developmental trajectories for both. However, the results were very different. In particular, there was no differential persistence of autism symptoms in those with disinhibited social engagement as seen for those in the INS/OTH group (Appendix C).
We also assessed whether dysfunctional attachment relations indicated by INS/OTH placed deprived children at risk for the development of emotional problems in adolescence and adulthood. The current findings provided little evidence for this hypothesis, with no significant differences between the two Rom>6 groups in terms of emotional problems at either the age 15 or the young adult assessment waves. Although there was a trend for more impairment and depression in the Rom>6 INS/OTH(+) group in young adulthood based on clinical assessment, this was not statistically significant when α was set at .01.
This is the first study to examine the relationship between attachment at age 4 years and long-term outcome trajectories through to young adulthood in children who suffered extreme adversity in early life. It had many strengths, including a comprehensive assessment of attachment security at age 4 and neurodevelopmental and mental health outcomes and its prospective natural experimental longitudinal design (with relatively low attrition). However, there were a number of limitations that need to be considered when interpreting the findings.
First, the sample only included a proportion of the children who eventually entered the ERA study (those for whom data was available at age 4) when the MSSP was first employed and we had confidence in its validity. This meant that we are unable to report conclusively about the impact of extended deprivation on attachment status or the effect of INS/OTH on development in the very deprived group who experienced between 24 and 43 months of deprivation.
Second, focusing only on those with age 4 MSSP data also reduced our sample size. This raises the possibility that the ERA sample, although perhaps the largest study of adopted children exposed to extreme deprivation to have been conducted to date, has limited power to detect interactions between variables, as required in the current analysis, especially when those with over 24 months of exposure are excluded. Our power calculation found that we had 93% power to detect medium-sized within or between two-way interaction effects (f = 0.25) with a sample size of n = 35, α = .05, 2 groups, 5 assessment waves, an intraclass correlation of .63 between repeated measures, and a nonsphericity correction of ε = .5.
Third, our limited sample size and the fact that few individuals displayed classical patterns of attachment insecurity and disorganization meant that our analysis was limited to a contrast of INS/OTH(+) and INS/OTH(–). We were unable to contrast INS/OTH with the other more normative insecure codes. We were also unable to breakdown the INS/OTH classification by its four subcodes to identify the extent to which it was the dysregulated affect that appeared characteristic of a number of late-placed adoptees that was important.
Fourth, our longitudinal analyses were necessarily limited to a carefully selected small number of items from different scales because of the need for equivalence across assessment waves. It may be that different patterns might emerge with more comprehensive assessments of the different phenotypes of interest. There was some support for this from the trend seen for depression in young adulthood.
In summary, INS/OTH was associated with persistence of ASD symptoms in adoptees who had previously experienced extended severe deprivation in the Romanian institutions. While we are unable to rule out the possibility that the dysfunctional attachment relations signified by this pattern of MSSP behaviors itself drove this negative developmental trajectory, the data are more consistent with the notion that it was an early marker of prior deprivation-related effects on social and cognitive development.







