



Introduction
Obsessive–compulsive disorder (OCD) is a psychiatric disorder characterized by the presence of obsessions and/or compulsions impairing everyday activities and provoking significant distress in a variety of quality of life domains.1-5
Cognitive behavioral models emphasize the role of obsessive beliefs in the development and maintenance of OCD. These models assert that obsessions may originate from catastrophic misinterpretations of normal intrusive thoughts, accompanied by the perception that the occurrence of a negative event is highly probableReference Rachman6 and by an inflated sense of responsibility, giving rise to distress and compulsions.Reference Salkovskis7 Following and elaborating on these early theories, the Obsessive Compulsive Cognitions Working Group8, 9 identified three main categories of dysfunctional obsessive beliefs: (1) Overestimation of Threat/Inflated Sense of Responsibility (erroneous beliefs regarding the probability of occurrence of a feared event/one’s vulnerability to and critical responsibility for preventing or avoiding negative outcomes); (2) Importance/Control of Thoughts (beliefs that a thought has the same potential as the actual action imagined, that leads the individuals to perceive their thoughts as extremely important, consequently determining thought control strategies to prevent negative events); (3) Perfectionism/Intolerance for Uncertainty (the need to succeed and avoid failure brings OCD patients to set exceedingly high personal standards that are inevitably impossible to meet. The desire and need to have everything in just the right place make OCD patients intolerant toward all that is uncertain).
Several studies demonstrated the specific role of obsessive beliefs in the development, maintenance and treatment response of OCD. Results have confirmed that stronger obsessive beliefs prospectively predict subsequent OCD onset in the general population, that OCD patients hold stronger obsessive beliefs than healthy control subjects, and that obsessive belief changes are associated with better treatment response.10-20 All three obsessive belief domains were also found to be individual predictors of psychological quality of life in OCD patients.Reference Kumar, Sharma, Kandavel and Reddy21
Sexuality is one of the key ingredients of human quality of life and wellbeing.Reference Davison, Bell, LaChina, Holden and Davis22, Reference Stephenson and Meston23 Sexual functioning is a neglected quality of life outcome in OCD research and is very rarely assessed during clinical practice with this type of patientsReference Pozza, Veale and Marazziti24 since psychotherapeutic and pharmacological treatment often exclusively focus on symptom reduction.Reference Norberg, Calamari, Cohen and Riemann25 Only a few studies investigated sexual functioning in OCD by focusing on the prevalence of specific sexual dysfunctions. In particular, increased sexual dissatisfaction and avoidance, less desire and arousal, or orgasm problems were more frequent in this condition than in the general population (53%-80% vs 10%-40%).26-29 Even sexual dysfunctions are more frequent in OCD patients than in other clinical groups such as patients with anxiety disorders.Reference Fontenelle, de Souza and de Menezes30
On the basis of studies performed in OCD patients showing an association between obsessive beliefs and different quality of life domains,Reference Kumar, Sharma, Kandavel and Reddy21 it may be hypothesized that obsessive beliefs are associated with poorer sexual functioning in the OCD population. Overestimation of Threat/Inflated Sense of Responsibility may create a state of self-criticism about sexual performance and focus the individual on failure. Importance/Control of Thoughts may lead the individual to try to suppress/control negative thoughts and thus focus on nonsexual stimuli, thereby compromising the possibility of sexual desire, arousal, and orgasm.Reference Basson and Gilks31, Reference Pahwa, Foley and Ishak32 Perfectionism/Intolerance for Uncertainty can impose unrelenting standards on the individual and contribute to problems in sexual satisfaction, pleasure, arousal, and overall performance.33-35
The Dual Control Model is a theoretical proposal introduced in sex research to explain impaired sexual functioning.Reference Janssen, Vorst, Finn and Bancroft36 According to it, satisfactory sexual response is based upon a balance between the neurophysiological systems of the sexual excitation and sexual inhibition that in turn are influenced by the psychological characteristics of the individual. The model introduced three processes related to sexual response: (1) Sexual Excitation, (2) Inhibition Due to Threat of Performance Failure (eg, fear of a performance failure during sexual act), (3) Inhibition Due to Threat of Performance Consequences (eg, fear of being seen by others during sexual encounters, fear of contagion with sexually transmitted diseases, fear of an undesired pregnancy). A strength of this model is that it considers the psychological processes associated with sexual response, such as the fear of performance failure. This aspect may assist researchers and clinicians in the exploration of the psychological dimensions related to impaired sexuality in clinical populations and distinguish these dimensions from the effects of pharmacological treatments that psychiatric patients often undergo.
Sexual response in OCD is overlooked and no study has investigated it according to the Dual Control Model nor explored the role of obsessive beliefs in this quality of life outcome of this population. The assessment of sexual response in OCD may have important implications in clinical practice such as the integration of sex/couple therapy in psychotherapeutic intervention. In addition, investigating whether obsessive beliefs are associated with sexual response may suggest that the psychotherapist should address these cognitive domains with the aim of improving sexual functioning. Therefore, the aims of the present study were to compare sexual excitation and inhibition according to the Dual Control Model between OCD patients and matched control subjects from the general population, and to investigate whether obsessive beliefs may predict sexual excitation and inhibition.
Methods
Participants
Inclusion criteria in the clinical group with OCD were (a) primary diagnosis of OCD according to the criteria of the DSM-5,2 (b) age higher than 17 years, and (c) provision of signed informed consent. Exclusion criteria were (a) psychotic disorders, (b) bipolar disorders and current major depression, (c) mental retardation, (d) neurological disorders, (e) OCD induced by drugs or medical diseases, and (f) drug dependence/abuse. All participants in the clinical group were outpatients recruited by mental health specialists in public or private centres. The control group, composed by individuals from the general population, was created matching each control participant to a clinical participant by gender and age. The presence of anti-obsessive drugs, specifically serotonin reuptake inhibitors, was not chosen as an exclusion criterion, as the majority of our OCD patients was taking these drugs, as it is common in specialized clinical settings.Reference Brakoulias, Starcevic and Belloch37
Participation was voluntary and uncompensated in both groups. All the participants included were asked to provide written informed consent to their participation after receiving a description of the aims and could withdraw consent at any time without consequence for their treatment. Materials containing personal information about participants were kept on electronic supports protected by passwords. The research, in accordance with the Helsinki Declaration, was approved by the Institutional Ethics Committee. The diagnosis of OCD was made through the Structured Clinical Interview for Axis I DisordersReference Mazzi, Morosini, De Girolamo, Lussetti and Guaraldi38) and confirmed through the Yale-Brown Obsessive Compulsive ScaleReference Goodman, Price and Rasmussen39 both administered by a mental health professional (psychiatrist or clinical psychologist).
Measures
Obsessive Compulsive Inventory—Revised (OCI-R)
The OCI-R is a revised version of the OCI developed by Foa et al.Reference Foa, Kozak, Salkovskis, Coles and Amir40 The OCI-R measures the distress caused by obsessive–compulsive symptoms using 18 items divided into 6 subscales (Washing, Obsessing, Hoarding, Ordering, Checking, and Mental Neutralising), evaluated using a 5-point Likert scale (0 = Not at all and 4 = Extremely).Reference Foa, Huppert and Leiberg41 The Italian version of the OCI-R presented good internal consistency (Cronbach’s α > 0.70), and excellent test–retest reliability (Pearson’s r > 0.70).Reference Sica, Ghisi and Altoe42 In the present study, internal consistency was good for all the scales (range of Cronbach’s α = 0.83-0.88).
Obsessive Beliefs Questionnaire-46 (OBQ-46)
The OBQ-46 is the Italian version of the OBQ developed by the OCCWG. It includes 46 items measuring 5 obsessive beliefs: Perfectionism, Responsibility for Harm, Control of Thoughts, Responsibility for Omissions, and Importance of Thoughts. Reference Dorz, Novara, Pastore, Sica and Sanavio43 Each item is evaluated on a 7-point Likert scale (1 = Strongly Disagree and 7 = Strongly Agree). The OBQ-46 presented good internal consistency (0.65 > Cronbach’s α > 0.86) and test–retest reliability (0.67 > Pearson’s r > 0.84).Reference Novara, Dorz, Pastore, Sica and Sanavio44 In the present study, internal consistency was good for all the scales (range of Cronbach’s α = 0.80-0.84).
Sexual Inhibition/Sexual Excitation Scales (SIS/SES)
Developed by Janssen et al,Reference Janssen, Vorst, Finn and Bancroft36 the SIS/SES measure individual differences in sexual response. They consist of 45 items divided according to three factors: SES (example item: “When I think of a very attractive person, I easily become sexually aroused”); Inhibition Due to Threat of Performance Failure (SIS1; example item: “When I have a distracting thought, I easily lose my erection/my arousal”); Inhibition Due to Threat of Performance Consequences (SIS2; example item: “If a realize there is a risk of catching a sexually transmitted disease, I am unlikely to stay sexually aroused”). Each item is evaluated on a 4-point Likert scale (1 = Strongly Agree and 4 = Strongly Disagree). For all three scales, higher scores indicate lower sexual excitation, lower inhibition due to threat of performance failure, and lower inhibition due to threat of performance consequences, respectively. The Italian version of the SIS/SES presented acceptable internal consistency (0.69 > Cronbach’s α > 0.89) and good test–retest reliability (Pearson’s r > 0.60).Reference Panzeri, Dèttore, Altoe, Zanella, Baldetti and Janssen45 In the present study, internal consistency was acceptable to good for all the scales (range of Cronbach’s α = 0.76-0.82).
Statistical analyses
Independent-group Student’s t tests were computed to investigate the between-group differences regarding frequency and intensity of OCD symptoms and beliefs and levels of sexual excitation/inhibition (SIS/SES). Effect sizes were calculated as Cohen’s d indices and were interpreted according to the following criteria: values equal to 0.80 or higher were interpreted as large, values up to 0.50 as medium, and values up to 0.20 as small.Reference Cohen46 Finally, we conducted ANCOVAs of SIS/SES scores to examine the interaction effects between groups (clinical group versus control group), OBQ-46 and OCI-R Total scores and group main effects. Statistical analyses were conducted using SPSS 24.00.47 Statistical significance was at a .05 P-value.
Results
Socio-demographic and clinical characteristics of the groups
Seventy-two OCD patients (mean age ± standard deviation [SD]: 34.50 ± 10.39 years) and 72 matched control participants (mean age ± SD: 34.25 ± 10.18 years) were included. In both groups, there were 55 men (62.5 %) and 27 women (37.5 %). The socio-demographic and clinical characteristics are shown in Table 1.
Table 1. Socio-Demographic and Clinical Characteristics.

Abbreviations: OCD, obsessive–compulsive disorder; SD, standard deviation.
Between-group comparisons
The OCD group reported significantly higher OCI-R Total, SES, SIS1, and SIS2 scores than the control group with medium to large effect sizes (Table 2). These results suggest that the OCD group experienced significantly higher levels of sexual excitation, inhibition due to threat of performance failure, and inhibition due to threat of performance consequences.
Table 2. Comparison Between the OCD and the Control Groups on the Clinical Scales.

Abbreviations: OBQ-46, Obsessive Beliefs Questionnaire-46; OCD, obsessive–compulsive disorder; OCI-R, Obsessive Compulsive Inventory—Revised; SD, standard deviation; SES, Sexual Excitation; SIS1, Inhibition Due to Threat of Performance Failure; SIS2, Inhibition Due to Threat of Performance Consequences.
No significant differences in SIS/SES scores were found between OCD patients who were on serotonergic antidepressants and those who were not. The scores between the two groups were not significantly different on the SES (t (70) = −0.77, P = .44), on the SIS1 (t (70) = −1.13, P = 0.26), and on the SIS2 (t (70) = −1.03, P = .30).
The comparisons between men and women showed no significant differences across gender on all the SIS/SES scores in the clinical group (range of t (70) = −1.87-1.40, P = 0.16-0.94) and in the control group (range of t (70) = −0.35-2.00, P = 0.05-0.72).
Obsessive beliefs and sexual response
The results of the ANCOVA showed an interaction effect between the group, OBQ-46 responsibility for harm scores and SES scores: for the control group, higher OBQ-46 responsibility for harm scores predicted higher SES scores, suggesting that control subjects with stronger responsibility for harm beliefs had lower sexual excitation (β = 0.018, t = 2.12, P < .05). There was an interaction effect also between the group and OBQ-46 control of thoughts scores: control subjects with stronger control of thoughts beliefs had higher sexual excitation (β = −0.015, t = 2.01, P < .05). An interaction effect also was found between the group and OCI-R total scores: OCD patients with more severe symptoms had lower excitation (β = 0.014, t = 3.03, P < .01).
The results showed an interaction effect between the group, OBQ-46 perfectionism scores and SIS1 scores: OCD patients with more severe perfectionism had significantly higher inhibition due to threat of performance failure than those with less severe perfectionism (β = −0.013, t = −2.41, P < .05).
Finally, an interaction effect was observed between the group, SIS1 scores and SIS2 scores: both OCD patients (β = 0.475, t = 4.25, P < .001) and control subjects (β = 0.371, t = 3.16, P < .01) with higher inhibition due to threat of performance failure had significantly higher inhibition due to threat of performance consequences than those with lower inhibition due to threat of performance failure.
The results of the ANCOVAs are provided in Tables 3 to 5.
Table 3. ANCOVA of SES scores on OBQ-46 and OCI-R scores in the total group (n= 144).

Abbreviations: CI, confidence interval; OBQ-46, Obsessive Beliefs Questionnaire-46; OCD, obsessive–compulsive disorder; OCI-R, Obsessive Compulsive Inventory—Revised; SE, standard error; SES, sexual excitation.
Table 4. ANCOVA of SIS1 Scores on OBQ-46 and OCI-R Scores in the Total Group (n = 144).

Abbreviations: CI, confidence interval; OBQ-46, Obsessive Beliefs Questionnaire-46; OCD, obsessive–compulsive disorder; OCI-R, Obsessive Compulsive Inventory-Revised; SE, standard error, SES, sexual excitation, SIS1, Inhibition Due to Threat of Performance Failure; SIS2, Inhibition Due to Threat of Performance Consequences.
Table 5. ANCOVA of SIS2 Scores on OBQ-46 and OCI-R Scores in the Total Group (n = 144).
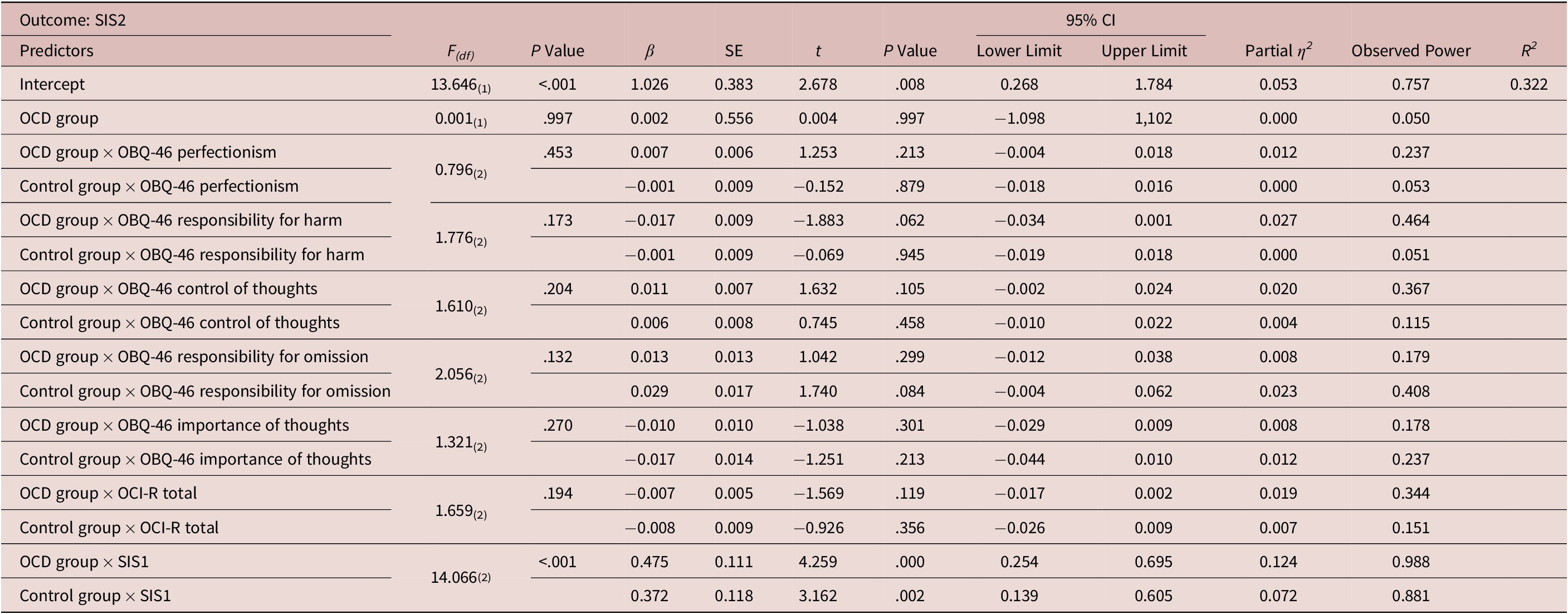
Abbreviations: CI, confidence interval; OBQ-46, Obsessive Beliefs Questionnaire-46; OCD, obsessive–compulsive disorder; OCI-R, Obsessive Compulsive Inventory-Revised; SE, standard error, SES, sexual excitation, SIS1, Inhibition Due to Threat of Performance Failure; SIS2, Inhibition Due to Threat of Performance Consequences.
Discussion
Sexual response is an overlooked quality of life outcome in OCD research and clinical practice; therefore, the present study aimed to fill this lack of information. According to our knowledge, it can be considered as the first one to explore sexual response according to the Dual Control Model in a group of OCD patients and matched healthy individuals of both sexes.Reference Bancroft and Janssen48
The ensuing findings showed that the OCD patients had higher levels of sexual excitation, inhibition due to threat of performance failure, and inhibition due to threat of performance consequences than controls. These results seem to be consistent with the Dual Control Model implying that healthy sexual response is associated with a balance between excitation and inhibition responses.Reference Bancroft and Janssen48 According to this model, a satisfactory sexual response implies that the levels of sexual excitation and inhibition are not excessively elevated. Sexual excitation, which influences how easily the individual becomes aroused by internal/external stimuli, is assimilated to a gas pedal, while sexual inhibition is conceptualized as a brake pedal, since it reduces sexual arousal and discourages sexual behavior when the context is inappropriate or the pursuit of sexual activities poses a threat to the person. Despite we found no difference in the levels of sexual excitation and inhibition between OCD patients who were on serotonergic antidepressants and those who were not, the inclusion of individuals who were taking SSRIs, which are known to impair sexual function, should be regarded as a major limitation of the study. Indeed, the lack of difference we found may be attributed to the relatively low statistical power of the analysis. In addition, we did not control for the effects of potentially confounding variables related to medications such as the duration of medication intake, dosages, and the types of antidepressants.
Some explanations may be put forward to explain evidence that OCD patients show a higher sexual excitation than control subjects. This phenomenon may be due to a rebound effect of sexual fantasies/thoughts provoked by mental suppression strategies that are frequent among OCD patients; such a process may lower the threshold of sexual excitation.Reference Purdon49 Again, OCD patients who often present alexithymic traits may misinterpret arousal-related body signals, or are unable to distinguish their subjective feelings of different emotions.Reference Pozza, Ferretti and Coluccia50, Reference Bankier, Aigner and Bach51 As such, OCD patients might confuse anxiety and excitation and vice versa. In addition, arousal nonconcordance phenomena may play a role in this difference (automatically occurring physical-reaction excitation to what is sexually relevant, not to what the individual actually wants and values).Reference Pulverman52
Moreover, increased sexual excitation levels in OCD patients may be explained by a nonspecific effect of interpersonal isolation, social avoidance, and depressive symptoms often associated with OCD.Reference McNally, Mair, Mugno and Riemann53 Indeed, in the field of sex research, evidence about sexual excitation is somewhat paradoxical, and controversies even exist on the notion that depression and anxiety are associated with a poorer sexual response, as one study reported that 20% of depressed/anxious patients showed an increased sexual excitation.Reference Janssen, Vorst, Finn and Bancroft36, Reference Bancroft and Janssen48 Some researchers proposed that increased sexual interest when depressed can be a strategy to cope with negative mood/loneliness feelings and indicate the need for personal contact or validation by another person.Reference Bancroft and Vukadinovic54 Alternatively, an increased sexual interest would represent a mean to achieve at least a transient reduction of anxiety and obsessions. The paradoxical effect of increased excitation in the clinical group might be an example of the so-called excitation transfer that occurs when arousal induced in association with anxiety becomes incorporated into response to sexual stimuli.Reference Zillman, Cacioppo and Petty55
Finally, the evidence of increased excitation in OCD may be in line with case reports describing patients whose OCD-related intrusions were accompanied by penis erection.Reference Warwick and Salkovskis56 The present findings related to higher excitation in OCD patients may suggest that sexuality should be used as a motivational element in the psychotherapeutic process with these patients with the aim of encouraging them to expose themselves to OCD-related situations and stop avoiding them. In addition, mindfulness-based interventionsReference Kabat-Zinn57 and metacognitive therapy modulesReference Wells58 may be useful in helping the patient to leave the need to control sexual fantasies/thoughts and stay in the present moment.
OCD patients with more intense symptoms had lower sexual excitation, while suggesting that the presence of more severe OCD characteristics is associated with impaired sexual response. It may be that the severity of obsessions can distract the individual from the present moment during sexual activity. In addition, the fact that OCD patients with more severe symptoms had lower excitation would suggest the need for the introduction of sex therapy modules for more severely affected patients.
OCD patients with more severe perfectionism showed a stronger sexual inhibition due to threat of performance failure than those with less severe perfectionism. Perfectionist beliefs may trigger performance anxiety and negative thoughts about the individual’s ability to perform well during sexual activity in combination with high standards about the necessity of pleasing the partner. Thus, it may be useful to introduce Acceptance and Commitment Therapy modules to increase the individual’s tolerance of failure or even to use group cognitive behavioral therapy to reduce the unrelenting standards of OCD patients by confronting with other people.Reference Pozza and Dettore59, Reference Strosahl, Hayes, Wilson, Gifford, Hayes and Strosahl60
Finally, both OCD patients and control subjects with stronger inhibition due to threat of performance failure had stronger inhibition due to threat of performance consequences than those with less strong inhibition due to threat of performance failure. This result suggests that the two inhibition processes are interrelated. This result may be in line with literature data showing that the Dual Control Model of sexuality may be applied to both clinical and community individuals.Reference Velten61 An implication of this may be that targeting one of them can lead to an improvement in the other.
Some limitations of the present study should be acknowledged. A major shortcoming is that 62% of both the groups was represented by males. In addition, the integration of self-report measures with clinician-administered interviews may improve the assessment of the sexual response. Future research should assess whether obsessive beliefs also predict categorical diagnoses of sexual dysfunctions. The use of a longitudinal design may allow a causal link between OCD (and obsessive beliefs) and sexual response to be demonstrated. An interpretation of these results may be that targeting beliefs can lead to an improvement in sexual response; however, it may be that targeting sexual response can lead to an improvement in beliefs and also in OCD. In addition, an assessment of depressive symptoms should be introduced. Finally, comparison with another clinical group (eg, a clinical group with mixed anxiety disorders) may help to establish the specificity of the role of beliefs in OCD sexual response. Another clinical group might also help in understanding whether the differences found between OCD patients and control subjects should be attributed to OCD or to a more general effect of living with a psychologically impairing condition.
Conclusions
Sexual response seems to be a quality of life outcome worth assessing in OCD patients. The Dual Control Model allows the psychological processes associated with sexuality to be assessed. The present study is the first to compare OCD patients and controls regarding levels of sexual excitation and inhibition and to investigate the role of obsessive beliefs in these sexual domains. Some specific obsessive beliefs may predict impaired sexual response. In the present study, OCD patients had higher sexual excitation, inhibition due to threat of performance failure, and inhibition due to threat of performance consequences than the controls. OCD patients with more severe symptoms had lower excitation and those with higher perfectionism had higher inhibition due to threat of performance failure. Both OCD patients and controls with higher inhibition due to threat of performance failure had stronger inhibition due to threat of performance consequences.
Overall, these findings support the importance of assessing sexuality in OCD and addressing perfectionism beliefs with the aim of improving sexual life. A key clinical implication of the present findings is the use of cognitive behavioral therapy and Acceptance and Commitment Therapy techniques as strategies aimed to reduce the patient’s perfectionistic intolerance of failure and unrelenting standards on sexual performance which might amplify fear of failure during sexual encounters.
Acknowledgements
Dr. Pozza, Prof. Dèttore and Dr. Marazziti planned and implemented the study and selected the subjects to be included. Dr. Pozza, Dr. Angelo and Dr. Prestia assessed all the subjects. Dr. Pozza carried out the statistical analysis. Dr. Marazziti, Dr. Pozza, Dr. Mucci, Dr. Prestia, Dr. Angelo and Prof. Dèttore revised all the available literature on OCD and sexuality. Dr. Pozza, Prof. Dèttore, Dr. Marazziti and Dr. Mucci wrote the paper, subsequently revised and approved by all authors.
Financial Support
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosures
Andrea Pozza, Donatella Marazziti, Federico Mucci, Nicole L. Angelo, Davide Prestia, and Davide Dèttore do not have anything to disclose.





