



Introduction
The most frequently used outcome measures in the treatment of major depressive disorder (MDD) are disorder-specific observer-rating scales like the Hamilton Depression Rating Scale (HAMD) or the Montgomery–Åsberg Depression Rating Scale (MADRS).Reference Hamilton 1 , Reference Montgomery and Åsberg 2
The HAMD was published in 1960 and comprises many sleep and anxiety items which mirror the clinical effects of the tricyclics frequently used in those days.Reference Hamilton 1 The MADRS was published in 1979 and comprises those 10 items of the larger Comprehensive Psychopathological Rating Scale (CPRS) that improved most during treatment with a variety of antidepressants including mianserin, amitriptyline, maprotiline, and clomipramine.Reference Montgomery and Åsberg 2 , Reference Åsberg, Montgomery, Perris, Schalling and Sedvall 3 Hence, both can be considered “antidepressant-friendly” scales, that is, they focus mainly on those symptoms that antidepressants are able to modify. It is remarkable that much less attention is paid to the development of self-rating scales that accurately focus on patient expectations.
Discrepancies have been described between the levels of change assessed with observer-rating scales and levels of change assessed with self-rating scales. It has been suggested that in very severe depression, the discrepancy between observer-rating and self-rating scales is due to the fact that the observer takes also nonverbal impressions into account resulting in relatively higher scores, while in dysthymia or so-called neurotic depression, self-rating scores tend to be inflated relative to observer ratings.Reference Möller 4 Effect sizes in psychological and pharmacological treatment studies are generally larger when considering observer ratings. A meta-analysis of psychological treatment studies found a 0.20 higher effect size with observer-rating scales vs self-rating scales.Reference Cuijpers, Li, Hofmann and Andersson 5 This difference can be due to different item content, to a different weighting of symptoms, or to observer or patient bias. Even in an antidepressant study using an observer-rating and a self-rating versions of the same scale (eg, MADRS and MADRS-S), outcome was better on the observer-rating than on the self-rating scale: 76.1% and 66.4%, respectively for response rates, and 56.1% and 49.6%, respectively for remission rates.Reference Fantino and Moore 6
Discrepancies have also been found between the content of standard assessment scales on one hand and what patients expect from treatment on the other hand. Indeed, patients who meet criteria for a Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV) MDD rather aim for “recovery” (ie, getting back the strength and the positive) than for “remission” (ie, fading away of the weakness and the negative). In fact, the highest ranking in patient treatment expectation is the return of a positive mental health state (optimism, vigor, and self-confidence), and the items considered to be most important are “my life is meaningful,” “I enjoy life,” “I am satisfied with myself,” and “I am able to concentrate.”Reference Zimmerman, McGlinchey, Posternak, Friedman, Attiullah and Boerescu 7 , Reference Demyttenaere, Donneau, Albert, Ansseau, Constant and van Heeringen 8 It is therefore remarkable that the standard definitions of response, remission, and recovery in MDD treatment studies often do not sufficiently take into account the specificity of patient expectations. This is clearly reflected in the fact that the assessment with standard scales (HAMD or MADRS) mainly focuses on the decrease of negative affect (ie, depressive or anxiety symptoms) and not on the increase of positive affect or of hedonic tone despite the fact that “loss of interest or pleasure” is a core criterion in the DSM-5 definition of MDD. 9 An elegant study investigating the association between the positive and negative mood items of the Center for Epidemiological Studies Depression Scale and a variety of psychopathological dimensions suggested that “(lack of) positive mood” is more specifically related to mood disorders while “(excess of) negative mood” is also related to a variety of other psychopathological dimensions.Reference Olson, Presniak and MacGregor 10 Recently, the Leuven Affect and Pleasure Scale (LAPS) was developed as a self-rating scale with the aim of better representing patient expectations: the 16-item scale comprises three subscales (negative affect, positive affect, and hedonic tone) and four independent items (cognitive functioning, overall functioning, my life is meaningful, and I feel happy).Reference Demyttenaere, Mortier, Kiekens and Bruffaerts 11 The scale was shown to differentiate well between three populations: healthy subjects, a student population subjects meeting diagnostic criteria for major depression but not being in treatment, and a group of inpatients with severe major depression.Reference Demyttenaere, Mortier, Kiekens and Bruffaerts 11 The changes in LAPS scores during antidepressant treatment have not yet been reported.
The aim of the present study was to investigate the changes in depressed outpatients during pharmacological treatment, assessing these changes with standard outcome scales as well as with the LAPS. A further aim was to investigate whether patients in remission reach comparable levels of negative affect, positive affect, hedonic tone, (cognitive) functioning, meaningfulness of life, and happiness as healthy controls.
Materials and Methods
Subjects
A total of 109 depressed outpatients were enrolled in the study (Belgium, N = 38; France, N = 10; Ireland, N = 10; and Italy, N = 51). Patients between 18 and 70 years were included when they fulfilled DSM-5 criteria for a major depressive episode and received treatment with an antidepressant. Exclusion criteria were meeting criteria for lifetime psychotic depression, bipolar disorder, alcohol or substance abuse, or clinical suspicion of dementia. The choice of the treatment was left to the discretion of the treating psychiatrist: pharmacotherapy as usual and combination with psychological treatment were allowed (resulting in a wide range of prescribed antidepressants sometimes combined with benzodiazepines or antipsychotics). Study duration was 8 weeks with visits and assessments at baseline and after 2, 4, and 8 weeks. At endpoint, 21 patients had dropped leaving 88 patients with data at all visits. Average age was 44.7 ± 13.1 years, 64% of included patients were female, 59% were married or living together, and 23% were on sick leave. A history of suicide attempt was reported in 21% of the patients. It was a recurrent episode for 71% of the included patients.
We also included two control groups of healthy volunteers. A first control group comprised 38 healthy controls from Italy (nursing and administrative staff). A second control group (for the LAPS scores) was taken from 111 healthy KU Leuven University students for whom we had LAPS scores, published in a previous paper.Reference Demyttenaere, Mortier, Kiekens and Bruffaerts 11The latter were a random sample of freshmen in their first year of university (University of Leuven) with a median age 18 years and a mean Composite International Diagnostic Interview depression score 7.88 ± 4.22.
The protocol was approved by the French “Comité consultative sur le traitement de l’information en matière de recherché dans le domaine de la santé” (CCTIRS; No. 15-885, 5/19/2016), by the “Ethisch Comité UPC KU Leuven” (EC 2016-290, 3/1/2016), and by the “Commissie Medische Ethiek UZ-KU Leuven” (S58943, 3/16/2016). All patients provided informed consent.
Instruments
In the depressed patient group, the following instruments were administered at each visit: the HAMD 17-item version, the Sheehan Disability Scale (SDS), the Positive and Negative Affect Scale (PANAS) with its two subscales for positive affect and negative affect, respectively, the Snaith–Hamilton Pleasure Scale (SHAPS), and the LAPS.Reference Hamilton 1 , 11-14 The 16-item LAPS has a subscore for negative affect (means of items 1-4), positive affect (means of items 5-8), hedonic tone (means of items 9-12), cognitive functioning, overall functioning, feeling that life is meaningful, and happiness.Reference Demyttenaere, Mortier, Kiekens and Bruffaerts 11 The scoring of the SHAPS was (in contrast to the original paper) reversed so that higher scores refer to higher pleasure scores (higher “hedonic tone”), which makes the interpretation in comparison with the LAPS hedonic tone easier. At baseline, the Clinical Global Impression of Severity (CGI-s) was assessed; after 2, 4, and 8 weeks of treatment, the overall improvement was assessed with the observer-rated Clinical Global Impression of Improvement (CGI-i) and the self-rated Patient Global Impression of Improvement (PGI-i).Reference Guy 15
Statistics
Descriptive statistics are provided using proportions and means (±standard deviations [SDs]). The correlation coefficient was used to assess associations between scales in MDD patients at baseline. Evolutions of scores during 8 weeks of antidepressant treatment were plotted using the SGPLOT procedure in SAS. Statistical differences in means between the control groups and HAMD remitters were examined using the independent samples t test with α set at 0.05. All analyses were performed using SAS 9.4 and SPSS 23.0.
Results
Baseline sociodemographic and clinical characteristics of the MDD population and of the healthy controls are given in Table 1. Correlations were calculated within the MDD population.
Table 1. Sociodemographic and Baseline Clinical Characteristics for Patients and for Italian Healthy Controls (Means ± SD, Percentages)

Abbreviations: CGI-s, Clinical Global Impression of Severity; HAMD, Hamilton Depression Rating Scale; LAPS, Leuven Affect and Pleasure Scale; MDD, major depressive disorder; PANAS, Positive and Negative Affect Scale; SD, standard deviation; SDS, Sheehan Disability Scale; SHAPS, Snaith–Hamilton Pleasure Scale.
Baseline negative and positive affect are negatively correlated, but the correlation coefficients are only modest: R = −0.41 between LAPS negative affect and LAPS positive affect and R = −0.20 between PANAS negative affect and positive affect.
The baseline HAMD is consistently correlated stronger with negative affect than with positive affect or with hedonic tone: the correlation coefficient is 0.51 with the PANAS negative affect score, 0.59 with the LAPS negative affect score, 0.41 with the PANAS positive affect score, −0.21 with the SHAPS hedonic tone score, −0.30 with the LAPS positive affect score, and −0.28 with the LAPS hedonic tone score (Table 2).
Table 2. Baseline Correlations Between LAPS Scores and Standard Scales (in MDD Patients)
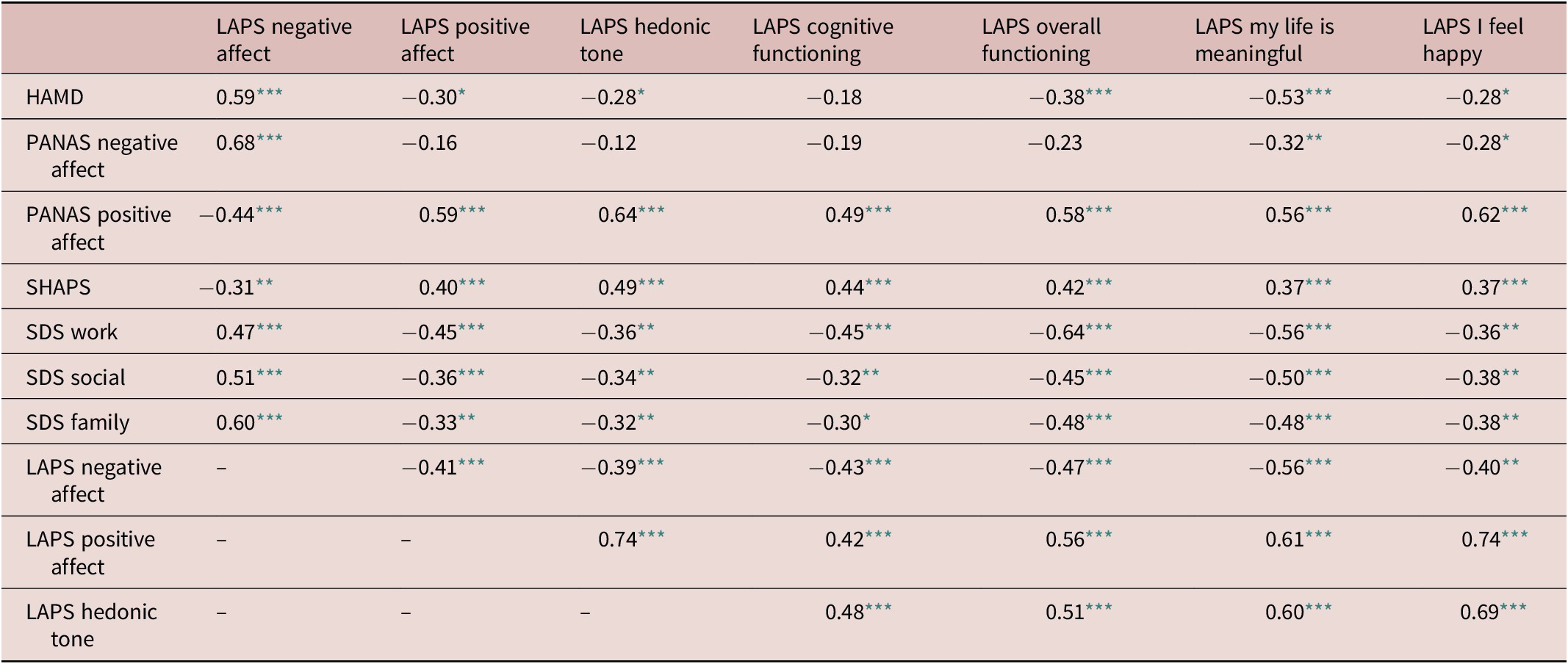
Abbreviations: HAMD, Hamilton Depression Rating Scale; LAPS, Leuven Affect and Pleasure Scale; MDD, major depressive disorder; PANAS, Positive and Negative Affect Scale; SDS, Sheehan Disability Scale; SHAPS, Snaith–Hamilton Pleasure Scale.
* P ˂ .05.
** P ˂ .01.
*** P ˂ .001.
The four single LAPS items (cognitive functioning, overall functioning, my life is meaningful, and I feel happy) have stronger correlations with positive mood than with negative mood (higher with PANAS positive affect and SHAPS hedonic tone than with the HAMD or the PANAS negative affect, and higher with LAPS positive affect or LAPS hedonic tone than with LAPS negative affect) (Table 2).
Figure 1 shows the evolution of the scores on different scales during the 8 weeks of antidepressant treatment. The decrease in HAMD and in LAPS negative affect is larger than the increase in LAPS positive affect, or the increase in LAPS hedonic tone, the increase in cognitive functioning, the increase in overall functioning, the increase in “my life is meaningful,” or the increase in “I feel happy.”

Figure 1. Evolution of Hamilton Depression Rating Scale (HAMD) and Leuven Affect and Pleasure Scale (LAPS) scores during 8 weeks of antidepressant treatment.
After 2 weeks of treatment, HAMD response and remission rates were 13% and 8% respectively; after 4 weeks, these rates were 34% and 21% respectively, and at 8 weeks rates were 86% and 38% respectively.
In HAMD remitted patients, negative affect is higher than in healthy Italian controls but lower than in healthy Belgian students when assessed with the LAPS and is not significantly different from healthy Italian controls when assessed with the PANAS. In HAMD remitters, positive affect is not significantly different from healthy Italian controls but is lower than in healthy Belgian students when assessed with the LAPS and is significantly lower than in healthy Italian controls when assessed with the PANAS (Table 3). Hedonic tone remains significantly lower when assessed with the LAPS or with the SHAPS. Cognitive functioning, overall functioning, “my life is meaningful,” and “I feel happy” also remain significantly lower than in healthy Italian controls or than in healthy Belgian students.
Table 3. Comparing HAMD Remitters to Healthy Italian Controls/Healthy Belgian Students at 8-Week Follow-Up

Abbreviations: HAMD, Hamilton Depression Rating Scale; LAPS, Leuven Affect and Pleasure Scale; PANAS, Positive and Negative Affect Scale; SD, standard deviation; SDS, Sheehan Disability Scale; SHAPS, Snaith–Hamilton Pleasure Scale.
Since patients considered to be in remission with the standard definition (ie, HAMD ≤ 7) were not yet comparable to healthy control populations (for all variables assessing positive mental health), we divided the remitters in four subgroups (HAMD 7 or 6, 5 or 4, 3 or 2, and 1 or 0) (Figure 2). As can be seen, there is a clear trend that LAPS scores only become comparable to healthy controls when the HAMD approaches 1 or 0: this is apparent for LAPS positive affect, LAPS hedonic tone, LAPS cognitive functioning, LAPS overall functioning, LAPS “my life is meaningful,” and LAPS “I feel happy” (scores or LAPS negative affect are reached earlier). The same trend is found with the PANAS: healthy control levels of negative affect are reached at a HAMD of 7, but healthy control levels of positive affect are only reached when the HAMD approaches 1 or 0.

Figure 2. LAPS scores for remitted patients (four subgroups: HAMD 7 or 6, 5 or 4, 3 or 2, and 1 or 0) and in healthy controls. Abbreviations: HAMD, Hamilton Depression Rating Scale; LAPS, Leuven Affect and Pleasure Scale; PANAS, Positive and Negative Affect Scale; SDS, Sheehan Disability Scale; SHAPS, Snaith–Hamilton Pleasure Scale.
Discussion
The present data provide empirical evidence for the fact that positive affect and negative affect are mainly independent clinical dimensions in depressed patients, as postulated in the original Watson and Clark paper more than 30 years ago.Reference Watson, Clark and Tellegen 13 Specifically, we found that the HAMD, which focuses mainly on negative affect (ie, depression and anxiety), has numerically stronger associations with negative affect (as measured with the PANAS negative affect score as well as with the LAPS negative affect score) than with positive affect or hedonic tone (the former assessed with the PANAS positive affect score or with the LAPS positive affect score, the latter assessed with the SHAPS hedonic tone or with the LAPS hedonic tone). Indeed, the HAMD does not cover positive affect and only poorly covers hedonic tone despite the fact that “lack of interest or pleasure” is a core criterion in the DSM-5 definition of major depression: only 1 score on one out of the 17 items refers to hedonic tone—“loss of interest in activity, hobbies or work” (score 2 on item 7—work and interests).Reference Hamilton 1 Our findings subsequently highlight a remarkable weakness of the HAMD, since anhedonia and lack of positive affect have been shown to be strong predictors of life expectancy as well in healthy as in medically ill people (even after correcting for negative affect).Reference Chida and Steptoe 16 Moreover, anhedonia and lack of positive affect/positive thinking have been shown to be strong protective predictors of persistent suicidal ideation after discharge as well in adolescents as in adults, even stronger than “hopelessness” as a well-known risk factor.Reference Yen, Weinstock, Andover, Sheets, Selby and Spirito 17 , Reference O’Connor, Fraser, Whyte, MacHale and Masterton 18 This was confirmed in a study with 1529 psychiatric inpatients where anhedonia was correlated with suicidality at baseline as well as at termination, and where anhedonia remained a robust protective predictor of persistent suicidal ideation independent of cognitive or (negative) affective symptoms of depression.Reference Winer, Nadorff, Ellis, Allen, Herrera and Salem 19 Moreover, positive affect has been shown to be a very important treatment expectations in patients suffering from depression.Reference Zimmerman, McGlinchey, Posternak, Friedman, Attiullah and Boerescu 7 , Reference Demyttenaere, Donneau, Albert, Ansseau, Constant and van Heeringen 8
It is worthwhile noticing that the four individual items of the LAPS (cognitive functioning, overall functioning, my life is meaningful, and I feel happy) are numerically more strongly correlated with positive affect and hedonic tone than with negative affect (as well when measured with the recent LAPS as when measured with the more standard SHAPS or PANAS). The intimate relationship between positive affect and cognitive functioning has been shown earlier in a factor analysis on the GENDEP and STAR*D database where cognitive functioning and positive affect clustered together in one dimension (the authors called it interest-activity but the items cover cognition and positive affect): it is remarkable that this factor was the strongest predictor of outcome with treatment.Reference Uher, Perlis and Henigsberg 20 From a clinical perspective, motivation (“what makes me move”) precedes cognitive functioning and overall functioning and is related to both reward anticipation and reward expectation. It has been shown earlier that anhedonia is a strong predictor of psychosocial dysfunctioning in depressed patients and that persistence of psychosocial dysfunctioning despite symptomatic response (measured with the MADRS) is strongly predicted by persistence of anhedonia.Reference Vinckier, Gourion and Mouchabac 21 A recent study in depressed patients treated with vortioxetine reported on a mediational analysis showing that improvement in anhedonia is a strong predictor of the association between improvement in depressive symptoms and reduced impairment in social functioning (as assessed with the SDS) explaining 39.9% of the variance (while no significant prediction was found for impairment in occupational or family functioning).Reference Cao, Park and Subramaniapillai 22 In addition, in the latter paper, one of the anhedonia measures was the so-called MADRS anhedonia factor comprising “apparent sadness, reported sadness, concentration difficulties, lassitude, and inability to feel” again mixing up affect, hedonic tone, motivation, and cognition. More strictly defined, anhedonia in the MADRS is represented only by two scores on item 8 (inability to feel): score 2 = reduced ability to enjoy usual interest and score 4 = loss of interest in surroundings, and loss of feelings for friends and acquaintances.Reference Montgomery and Åsberg 2 This strong relation between positive affect/hedonic tone and cognitive or overall functioning is a further illustration of the broaden-and-build theory of positive emotions.Reference Fredrickson 23 This theory showed how positive emotions appear to broaden peoples’ momentary thought–action repertoires (which are important in cognitive functioning) and build their enduring (inter)personal resources (which are important in social and overall functioning).Reference Fredrickson 23
When looking at the evolution of positive affect/hedonic tone and negative affect during treatment, important new findings are observed. First, the rates of response and remission rates (based on the standard 50% decrease on the HAMD or on a HAMD ≤ 7) are in the expected range.
Second, the decrease of negative affect (HAMD, PANAS negative affect, and LAPS negative affect) is greater than the increase in positive affect (PANAS positive affect and LAPS positive affect) or the increase in hedonic tone (SHAPS hedonic tone and LAPS hedonic tone). The LAPS positive affect and LAPS hedonic tone seem to better differentiate better between responders and nonresponders than the PANAS positive affect and the SHAPS hedonic tone. The LAPS has a broader range of positive affect items (activated and deactivated positive affect as well as affiliative positive affect, the latter being absent in PANAS positive affect) and a broader range of hedonic tone (anticipatory and consummatory, both for sensory and for social hedonic tone, all of them less well differentiated in the SHAPS where the items moreover have a somewhat confusing phrasing: “I would enjoy”).Reference Demyttenaere, Mortier, Kiekens and Bruffaerts 11 , Reference Snaith, Hamilton, Morley, Humayan, Hargreaves and Trigwell 14
But, probably the most important finding of the study is that the standard threshold for remission from depression on the HAMD 17-item scale (cutoff of 7) could well be too high for defining a return to “being back to normal.”Reference Frank, Prien and Jarrett 24 While the present data show that the standard definition of remission is associated with a more or less normal range of negative affect, all other measures consistently do not reach the normal range. An additional exploratory analysis looking at subgroups (HAMD 7 or 6, 5 or 4, 3 or 2, and 1 or 0) suggests that all the latter measures only reach the normal range when the HAMD approaches a score 1 or 0. Remitters therefore seem to reach more or less normal negative mood, but do not seem to reach normal positive mood. It has already been suggested that the standard cutoff for remission (HAMD score of 7) should be lowered and that patients with a scoring 0 to 2 could be considered “highly likely” to be in remission, while patients with a scoring 3 to 7 could be considered “possibly” in remission.Reference Zimmerman, Martinez and Attiullah 25 In that paper, there were significant differences between the latter two subcategories in work performance, marital relations, family relations, mental health, leisure, global rating of life satisfaction, and global rating of quality of life.Reference Zimmerman, Martinez and Attiullah 25 The question remains why these patients do not reach normal levels of positive affect, hedonic tone, (cognitive) functioning, “my life is meaningful,” or “I feel happy.” One reason could be that the treatment did not (yet) reach maximum efficacy (lack of positive affect could then be considered as a “residual symptom”), or it could be that a depressive episode leaves the patient with a scar, or it could be that even in their premorbid state they had overall lower levels of positive affect/hedonic tone/functioning. Only a long-term prospective study of a large population cohort could differentiate between these options.
A limitation is that the choice of the antidepressant, the concurrent use of other psychotropic medication, or changes during the study duration were tolerated: a larger study comparing two antidepressants (with different mechanism of action) with limitations on drug changes or drug combinations would be an interesting next study. Another limitation is that the subgroups of remitted patients (with HAMD scores of 6 or 7, 4 or 5, 2 or 3, and 0 or 1) are too small to perform statistical analyses: larger patient samples should hence confirm these findings.
In conclusion, the present study illustrates that positive and negative affect are mainly independent clinical dimensions and that (cognitive) functioning, meaningfulness of life, and happiness are more closely related to positive affect and hedonic tone than to negative affect. The most important finding, however, is that the standard definition of remission (with the HAMD) should be lowered if the treatment goal is not only bringing back negative affect to normal levels, but also bringing back positive affect, hedonic tone, (cognitive) functioning, and meaningfulness of life/happiness to normal levels. The standard definition of remission (HAMD cutoff of 7) is therefore probably adequate for remitting the negative mood, but not good enough in recovering positive mood, hedonic tone, functioning, or meaningfulness of life.
Disclosures
G.K., P.M., and R.B. have nothing to disclose. K.D. has the following disclosures: LivaNova: personal fees, consultant, and speaker’s bureau; Servier: personal fees, consultant, advisory board, and speaker’s bureau; and Johnson & Johnson: advisory board. L.M. received honoraria from Servier in relation to this study. P.G. received during the last 5 years fees for presentations at congresses or participation in scientific boards from Alcediag-Alcen, Angelini, GSK, Janssen, Lundbeck, Otsuka, SAGE, and Servier. M.D.G. received fees as a consultant/advisor from Servier, Lundbeck, and Otsuka.





