Introduction
Although non-heterosexual populations are known to be at greater risk for a variety of mental health disorders than their heterosexual counterparts,1 few studies have examined how mental health varies across the continuum of sexual orientation. In public health research, sexual orientation is typically described in terms of three discrete categories (heterosexual, gay/lesbian, bisexual). Even so, most evidence indicates that sexuality exists along a continuum, ranging from exclusively opposite sex (“0”) to exclusively same-sex (“6”) orientation on a Kinsey-like scale.Reference Savin-Williams2 Men with a small amount of same-sex attraction (Kinsey 1s), for example, report more mental health problems—including depression, suicidality, anxiety, self-harm, body dissatisfaction, disordered eating, and substance use—compared to heterosexual men.Reference Vrangalova and Savin-Williams3 Other studies suggest that bisexuals (Kinsey 2 to 4) and “mostly” gay or lesbian participants (Kinsey 5s) are at greater risk for non-suicidal self-injury,Reference Whitlock, Muehlenkamp, Purington, Eckenrode, Barreira and Abrams4 mood/anxiety disorders,Reference Bostwick, Boyd, Hughes and McCabe5 and substance useReference Hughes, Szalacha and McNair6–Reference McCabe, Hughes, Bostwick and Boyd8 than heterosexual and (in some cases) exclusively same-sex attracted individuals. However, the current literature on sexuality and mental health has 2 major gaps. First, it has focused mostly on substance addictions without examining whether same-sex sexuality is also correlated with rates of non-substance (“behavioral”) addictions.Reference Grant, Potenza, Weinstein and Gorelick9 Second, studies have not yet explored whether the health disparities between heterosexual and non-heterosexual populations could be partly explained by trait differences in impulsivity and compulsivity.
To address these conceptual and empirical limitations, we examined the association between mental health issues and sexual attraction—a key indicator of sexual orientation—in a large, non-clinical sample of university students. Sexual attraction was assessed using the Klein Sexual Orientation Grid (KSOG), a Kinsey-like scale.Reference Klein, Sepekoff and Wolf10 We hypothesized that a greater degree of same-sex attraction would be associated with higher rates of behavioral addictions (gambling disorder, compulsive sexual behavior, binge eating disorder) and personality (trait) measures of impulsivity.
Methods
Survey design
The Department of Psychiatry and Behavioral Neuroscience at the University of Chicago and Boynton Health at the University of Minnesota jointly developed the Health and Addictive Behaviors Survey to assess health and well-being in a large sample of university students. The survey included basic demographics and questions from several validated screening tools examining mental health and psychological well-being. All study procedures were carried out in accordance with the principles of the Declaration of Helsinki and were approved by the University of Minnesota’s Institutional Review Board (IRB).
Participants
A total of 10,000 college and graduate students at a large, nondenominational and coeducational university in the midwestern United States were chosen by random, computer-generated selection. Over a 3-week period during the fall 2016 semester, students were invited by email to complete the Health and Addictive Behaviors Survey online. Of the 10,000 email invitations, 9449 were successfully received by the recipients (ie, did not bounce back). Recipients of the email were first required to view the IRB-approved online informed consent page, at which point students could choose to participate in the survey or opt out. The survey asserted that all information was both anonymous and confidential. Compensation was offered at the conclusion of the survey by randomly selecting respondents to receive tablet computers (n = 3) or gift certificates to an online retailer in the amounts of $250 (n = 4), $500 (n = 2), or $1000 (n = 1). Participants were required to review all survey questions to be eligible for prize drawings but were not required to answer any question they did not wish to answer. Of the 9449 students who received the invitation to participate, 3659 (38.7%) completed the survey.
Assessments
The self-report survey consisted of 156 questions and took participants approximately 30 minutes to complete. The survey collected information on demographics, self-reported sexual behavior, and academic achievement (ie, grade point average [GPA]). As described below, survey questions also assessed participants’ sexuality and clinical characteristics, including current mental health and substance use problems.
Multiple dimensions of sexual orientation were assessed using a modified version of the Klein Sexual Orientation Grid (KSOG).Reference Klein, Sepekoff and Wolf10 The KSOG was derived from the Kinsey scale and measures actual sexual experiences as well as sexual attractions, sexual fantasies, emotional preferences, and social preferences in the past and present. The KSOG uses a 7-point Likert-type scale from 1 (other sex only) to 7 (same sex only) to describe the continuum from exclusively opposite-sex to exclusively same-sex orientation. The KSOG is a valid and reliable measure of sexual orientation.Reference Weinrich and Klein11, Reference Weinrich, Klein, McCutchan and Grant12 Of the major domains of sexual orientation, we focused on sexual attraction given that sexual identity and sexual behavior are considerably fluid.Reference Savin-Williams13, Reference Savin-Williams, Joyner and Rieger14 The KSOG includes a self-identification measure (“How do you label or identify yourself?”) that was not used in our survey instrument.
In order to assess mental health functioning and aspects of self-regulation, participants were asked to complete the following measures:
The Alcohol Use Disorders Identification Test (AUDIT) is a well-validated, 10-item questionnaire used to assess alcohol use behaviors and related problems.Reference Saunders, Aasland, Babor, de la Fuente and Grant15 Each item is scored 0–4, with a maximum of 40 points possible. A score of 8 or greater indicates hazardous or harmful alcohol use.
The Drug Abuse Screening Test (DAST-10) is a valid and reliable, 10-item, yes/no measure of problematic substance use.Reference Skinner16, Reference Yudko, Lozhkina and Fouts17 A score of 3 is used to screen for a drug use disorder.
The Patient Health Questionnaire (PHQ-9) assessed depressive symptoms. This valid 9-item measure is based directly on Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR) criteria for major depressive disorder.Reference Kroenke, Spitzer and Williams18
The Primary Care PTSD Screen (PC-PTSD) was used to screen for posttraumatic stress disorder (PTSD) based on DSM-IV PTSD criteria.Reference Prins, Ouimette and Kimerling19 A score of ≥3 indicates probable PTSD.
The Generalized Anxiety Disorder-7 (GAD-7) screened for generalized anxiety disorder.Reference Spitzer, Kroenke, Williams and Löwe20 Total scores of 10 or greater indicate clinically significant anxiety.
The Body Dysmorphic Disorder Questionnaire (BDDQ) screened for body dysmorphic disorder.Reference Phillips21
The Minnesota Impulsive Disorders Interview (MIDI) assessed for a range of putative disorders of impulse control, including gambling disorder and compulsive sexual behavior.Reference Grant22
The Adult ADHD Self-Report Scale (ASRS-v1.1) was used to screen for attention-deficit/hyperactivity disorder (ADHD). The ASRS contains 6 items and has demonstrated strong psychometric properties.Reference Kessler, Adler and Ames23
The Rosenberg Self-Esteem Scale (RSES) measured global feelings of self-worth or self-regard.Reference Rosenberg24 Scores below 15 suggest low self-esteem.
The Barratt Impulsiveness Scale, Version 11 (BIS-11) examined impulsivity across 3 dimensions: attentional (inability to concentrate), motor (acting without thinking), and non-planning (lack of future orientation).Reference Patton, Stanford and Barratt25, Reference Stanford, Mathias, Dougherty, Lake, Anderson and Patton26
The Cambridge–Chicago Compulsivity Trait Scale (CHI-T) provided a valid and reliable 15-item measure of compulsive traits (eg, being comfortable when things are done “just right”).Reference Chamberlain and Grant27
Data analysis
All respondents with complete data on the sexual attraction domain of the KSOG were included in the analyses (N = 2743; 74.96%). Relationships between attraction and clinical measures were investigated using Kendall’s tau-b. Statistical significance was defined as p ≤ 0.01 to account for multiple comparisons. SPSS (version 25) was used for all statistical analyses.
Results
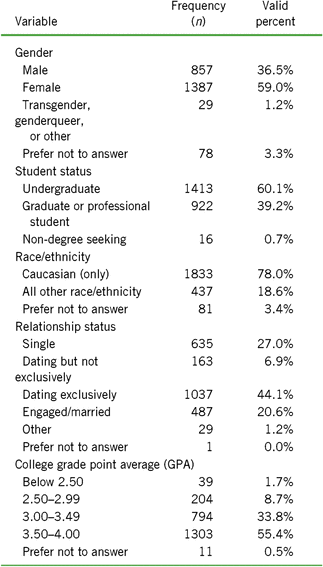
The demographics of the sample are presented in Table 1. The typical participant reported a small degree of same-sex attraction in the past (over one year ago; mean KSOG score = 1.51 [SD = 1.33]) and in the present (within past year; mean KSOG score = 1.55 [1.39]). Survey respondents showed a slight female predominance (59.0%) and were more likely to be white/Caucasian (78.0%) than students at the university as a whole. There was no correlation between sexual attraction and college GPA (τb = .027, p = .118).
TABLE 1. Characteristics of university students (N = 2743) who completed questions concerning sexual attractiona
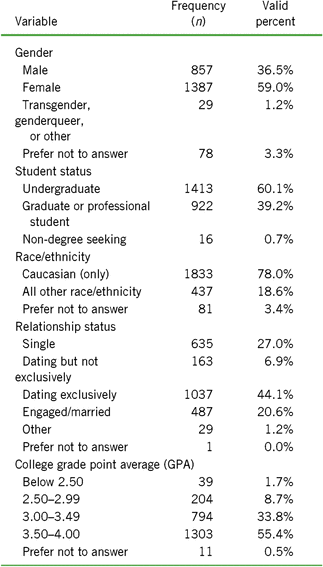
a Assessed by the Klein Sexual Orientation Grid (KSOG).
In terms of sexual behavior, students reporting a greater degree of same-sex attraction were significantly more likely to be sexually active at a younger age (τb = .118), to be sexually active without using some form of barrier protection (τb = .069), to have a higher number of sexual partners (τb = .136), and to report a past sexually transmitted infection (τb = .107; p < .001 for all). As expected, same-sex attraction showed a strong correlation with same-sex behavior (as measured by the KSOG) both in the past (τb = .614, p < .001) and present (τb = .553, p < .001).
Drug and alcohol use by the participants is presented in Table 2. Same-sex attraction was significantly associated with problematic substance use and the use of a wide range of illicit drugs (cocaine, hallucinogens, prescription pain medication, sedatives).
TABLE 2. Association between drug and alcohol use and sexual attractiona in university students (N = 2743)

Note. A positive correlation coefficient indicates that the variable is associated with a greater degree of same-sex attraction (ie, score of 7 on the KSOG). AUDIT, Alcohol Use Disorders Identification Test; DAST-10, Drug Abuse Screening Test.
a Assessed by the Klein Sexual Orientation Grid (KSOG).
b Responses rated on a 5-point scale of 1 (never used), 2 (used in past; have not used in past 12 months), 3 (use rarely), 4 (use occasionally), 5 (use daily).
c Including both prescription medications (eg, d,l-methylphenidate [Concerta, Ritalin], d,l-amphetamine [Adderall]), and drugs of abuse (eg, methamphetamine).
d Including barbiturates, methaqualone (Quaalude), sleeping aids, tranquilizers/benzodiazepines (eg, alprazolam [Xanax]), and ketamine.
* p < .01.
Aspects of mental health are presented in Table 3. Same-sex attraction was associated with higher rates of most mental health disorders (including compulsive sexual behavior, binge eating disorder, and ADHD), but not gambling disorder or body dysmorphic disorder.
TABLE 3. Association between mental health problems and sexual attractiona in university students (N = 2743)

Note. A positive correlation coefficient indicates that the variable is associated with a greater degree of same-sex attraction (ie, score of 7 on the KSOG). GAD-7, Generalized Anxiety Disorder-7; PC-PTSD, Primary Care PTSD Screen; PHQ-9, Patient Health Questionnaire; RSES, Rosenberg Self-Esteem Scale.
a Assessed by the Klein Sexual Orientation Grid (KSOG).
* p < .01.
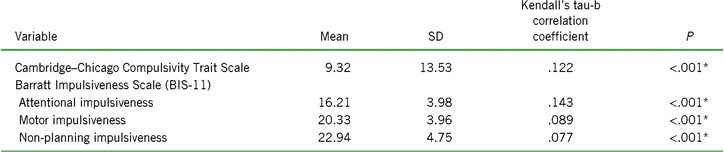
Same-sex attraction was significantly associated with higher traits of impulsivity (BIS-11) and compulsivity (CHI-T) (p < .001; Table 4).
TABLE 4. Association between impulsivity/compulsivity and sexual attractiona in university students (N = 2743)

Note. A positive correlation coefficient indicates that the variable is associated with a greater degree of same-sex attraction (ie, score of 7 on the KSOG).
a Assessed by the Klein Sexual Orientation Grid (KSOG).
* p < .01.
Discussion
Sexual orientation is a complex, multidimensional construct that has presented challenges for public health researchers.Reference Wolff and Wells28 In this study, we explored the association between sexual attraction and a wide range of mental health variables in a university sample. Our use of a continuum to describe sexual orientation reflects considerable evidence that many people show non-exclusivity in their sexual attractions, behavior, or both.Reference Savin-Williams2 We found that same-sex attraction was strongly correlated with riskier sexual practices, multiple types of substance use, and a wide range of mental health problems. Although these findings are largely consistent with previous studies of LGBQ students,Reference Oswalt and Wyatt29, Reference Grant, Odlaug, Derbyshire, Schreiber, Lust and Christenson30 this study expands our understanding of sexual-minority health in 2 ways. First, we found that sexual attraction was associated with multiple addictive problems, including non-substance or “behavioral” addictions.Reference Grant, Potenza, Weinstein and Gorelick9 In a second, related finding, same-sex attraction was correlated with personality measures of impulsivity and compulsivity, suggesting a possible cognitive/physiological mechanism that may contribute to LGBQ health disparities. These findings have implications for the health and well-being of the many young adults who experience some degree of same-sex attraction.
Health disparities in sexual orientation are typically explained in terms of minority stress—that is, chronic stress related to stigma and discrimination.Reference Meyer31, Reference Meyer, Meyer and Northridge32 A wealth of research has examined the relationship between adverse health outcomes and identity development, the state of being “out,” and internalized biases (ie, internalized homonegativity) in the LGBQ community. Internalized homonegativity, for example, refers to the process by which LGBQ people internalize negative social attitudes and assumptions about sexual orientation, resulting in feelings of shame, low self-esteem, and other emotional problems. Although a psychological framework may explain some of the findings in this study, it is unlikely to explain all of them, particularly the strong associations between same-sex attraction and disorders thought to have an underlying biological component: compulsive sexual behavior, binge eating disorder, and ADHD. Nor is there a clear connection between minority stress and personality traits of impulsivity and compulsivity, which describe deeply rooted patterns of behavior. These discrepancies invite a broader understanding of how diverse cognitive and socio-emotional processes may contribute to human sexuality.
Students with high levels of same-sex attraction in our sample showed high rates of substance use, ADHD, and other problematic behaviors such as risky sexual behavior and binge eating. Same-sex attraction was also significantly associated with personality traits of both impulsivity and compulsivity, as seen on the BIS-11 and CHI-T. When viewed together, these findings suggest that self-regulatory problems may play a global (rather than context-dependent) role in the lives of LGBQ young adults.
The taxonomy of self-control includes 2 distinct but related concepts: impulsivity and compulsivity. Impulsivity—broadly defined as a tendency to act without regard to negative consequences—is a core feature of a sweeping number of public health problems, including ADHD and substance use and eating disorders.Reference Congdon and Canli33, Reference Sharma, Markon and Clark34 Impulsivity is also associated with risky sexual practices,Reference Charnigo, Noar, Garnett, Crosby, Palmgreen and Zimmerman35, Reference Deckman and DeWall36 such as low rates of barrier protection use and higher numbers of sexual partners, both of which were correlated with same-sex attraction in this study. By contrast, compulsivity—a tendency toward repetitive or habitual behaviors—may make a separate or overlapping contribution to these and other health problems. The extent to which deficits in self-regulation contribute to sexual orientation–related health disparities, and how, requires further investigation.
Interestingly, same-sex attraction was not associated with body dysmorphic disorder or gambling disorder, 2 conditions that also have impulsive or compulsive features. Given the low prevalence of these disorders in our sample, it is possible that our study was underpowered to detect relationships between these variables and sexuality. Our negative findings therefore require replication in a larger sample before firm conclusions can be drawn.
These findings may have implications for the health and well-being of sexual minorities. Alongside minority stress, our data suggest that the relatively poor health of non-heterosexual young adults could be partly explained by biological factors unrelated to social experiences. In other settings, similar statements have engendered considerable controversy. A biological understanding of sexuality has been welcomed by some, who hope that it will lead to greater acceptance and inclusion, and condemned by others, who fear that such knowledge could be abused. Nevertheless, scientific approaches have shed growing light on the biology of sexual orientation. One provocative genome-wide linkage study has identified genes on chromosome 8 and chromosome Xq28 that may influence how sexual orientation develops in males.Reference Sanders, Martin and Beecham37 Other studies suggest that sexual orientation in males may be influenced by prenatal hormones and a maternal immune response during fetal development.Reference Balthazart38 Whether a shared biological mechanism links these factors with impulsivity and compulsivity—themselves constructs with partially overlapping neurobiology—is unknown.
Limitations
Our study has the advantage of being relatively large. Even so, several limitations should be noted. First, our study was cross-sectional and therefore cannot determine the direction of causality for any effects. Second, diagnostic assessment via an online survey may be less accurate (more “noisy”) compared with an in-person clinical evaluation due to response bias and underreporting. Our large sample size, however, provided the ability to detect even relatively small effects. Third, using a self-report questionnaire to assess sexual orientation poses methodological challenges. The KSOG (like the Kinsey scale) has been criticized for requiring participants to make a tradeoff between same- and opposite-sex orientationReference Sell39 and by sexual minorities themselves for not capturing certain aspects of their sexuality.Reference Galupo, Mitchell, Grynkiewicz and Davis40 We believe that this study nevertheless provides robust measures of association between sexuality and mental health outcomes. Finally, we did not identify factors associated with sexual attraction by gender. Gender may have affected the results of our study given that men are relatively more impulsive than women. However, the instrument that we used to measure trait impulsivity (the BIS-11) has shown no significant gender differences in previous studies.Reference Patton, Stanford and Barratt25, Reference Stanford, Mathias, Dougherty, Lake, Anderson and Patton26
Conclusion
Same-sex sexuality is associated with numerous public health concerns including substance and behavioral addictions, affective problems, and high-risk sexual behavior (earlier age at first sexual experience and lower use of barrier protection). These findings may be partly explained by personality traits of impulsivity. Further research is needed to understand the potential cognitive and developmental processes that contribute to health disparities among sexual minorities.
Disclosures
Dr. Grant has received research grant support from the American Foundation for Suicide Prevention, Takeda Pharmaceuticals, and the TLC Foundation for Body-Focused Repetitive Behaviors; he receives yearly compensation from Springer Publishing for acting as Editor-in-Chief of the Journal of Gambling Studies; and he has received royalties from American Psychiatric Publishing, McGraw Hill, Norton Press, Johns Hopkins University Press, and Oxford University Press. Dr. Lust and Dr. Christenson report employment with Boynton Health. Dr. Blum has nothing to disclose.