



The aortic valve comprises three semilunar cusps and functions to allow unidirectional blood flow from the left ventricle into the systemic circulation. These cusps are right coronary, left coronary, and non-coronary cusps, named based on their relationship to the coronary arteries.Reference Angelini, Ho and Anderson1 Anatomical variations of the aortic valve have been documented notably the unicuspid, bicuspid, and quadricuspid valves. Of these variants, the bicuspid aortic valve is the most common congenital aortic valve abnormality with a prevalence of approximately 1–2% in the general population.Reference Krepp, Roman and Devereux2 On the other hand, unicuspid aortic valve (estimated prevalence of 0.02% in the general population and 4–6% in patients presenting for isolated aortic valve replacement)Reference Krepp, Roman and Devereux2 and quadricuspid aortic valve (estimated prevalence of general population ranges from 0.013 to 0.043%, and 1% intraoperatively during aortic valve surgery)Reference Robicsek, Sanger, Daugherty and Montgomery3 follow, respectively. Unicuspid and quadricuspid aortic valves share many characteristics with the bicuspid aortic valve, such as aortic valve stenosis and/or regurgitation and aortic dilatation.
There are two case reports in this study. A 16-year-old male with moderate aortic valve stenosis, mild aortic valve regurgitation, and ascending aorta dilatation secondary to a unicommissural unicuspid aortic valve and a 13-year-old female with mild aortic valve regurgitation secondary to a quadricuspid aortic valve.
Case 1
A 16-year-old male patient was admitted to our outpatient clinic with the diagnosis of congenital aortic valve stenosis. In the neonatal period, a diagnosis of the bicuspid aortic valve was made and he was followed up regularly due to aortic valve stenosis.
His pulse rate was 75/min, with a blood pressure of 130/90 mmHg. A 3/6 systolic murmur was auscultated over the whole precordium, with the murmur radiating to the neck. Electrocardiogram showed sinus rhythm and there was no left ventricular hypertrophy findings by voltage criteria. His chest X-ray was normal with cardiac index within referral range. The patient did not describe effort dyspnoea or syncope in both resting and during the exercise test.
Transthoracic echocardiography demonstrated unicommissural type unicuspid aortic valve with a commissure between the left and right coronary cusps, which is at 6 o’clock, normal left ventricle systolic function, mild left ventricle hypertrophy, moderate aortic stenosis (peak/mean gradient of 55/31 mmHg with an aortic valve area of 2.2 cm2 (1.67 cm2/m2)), and eccentric mild aortic valve regurgitation with a vena contracta of 6 mm. Coronary arteries were normal. The transthoracic echocardiography also showed prolapsed mitral valve, mild mitral valve regurgitation, and ascending aorta dilatation (37 mm, z score: +5.75) (Fig1a–d).
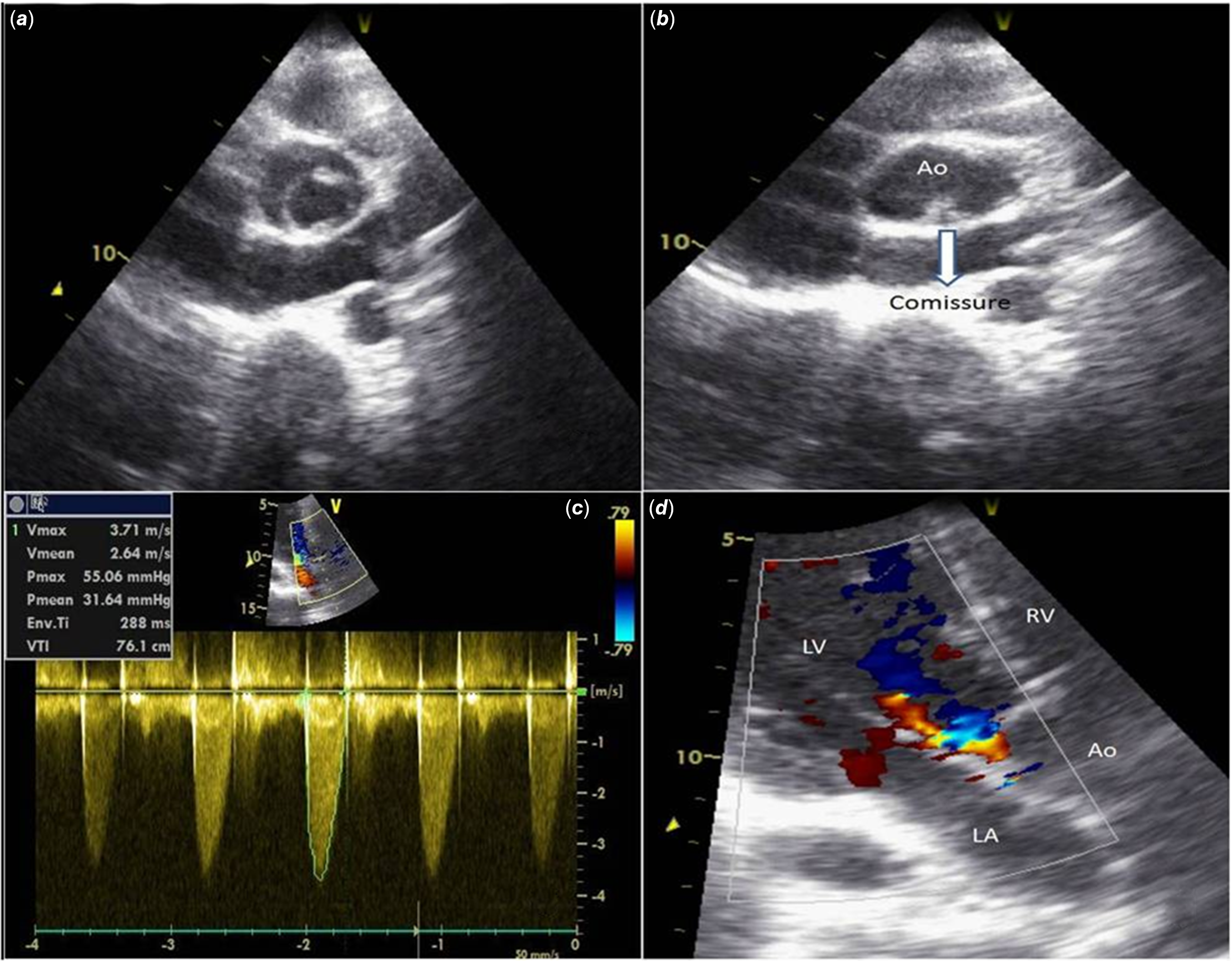
Figure 1. (a, b, c and d) Transthoracic echocardiogram in parasternal short-axis view demonstrating (a) a unicuspid aortic valve with an eccentric orifice in systole, (b) in diastole with one commissure at 6 o’clock, (c) moderate aortic valve stenosis by continuous-wave Doppler, (d) eccentric mild aortic valve regurgitation.
His aortic valve stenosis was defined as moderate, according to the 2017 ESC/EACTS valvular heart guideline.Reference Falk, Baumgartner and Bax4 This guideline recommends aortic valve replacement in moderate aortic valve stenosis, only in cases requiring cardiac surgery for other indications. Since he had no additional cardiac pathology requiring surgery, and he did not have exertional dyspnoea or syncope in both resting and during the exercise test, he was not intervened, and close follow-up was performed every 3 months. Consent was obtained from the patient’s parent for this case study.
Case 2
A 13-year-old girl was seen in the cardiac outpatient clinic. She was previously followed for rheumatic fever. Her blood pressure was 120/60 mmHg, pulse rate was 79/min, and a grade 1-2/6 diastolic murmur was heard at the third left intercostal space. Electrocardiogram was normal. His chest X-ray was normal with cardiac index within referral range. The patient did not describe effort dyspnoea or syncope.
Transthoracic echocardiography finding in the short-axis view was an X-shaped commissure pattern during diastole and a rectangular appearance during systole. The cusps appeared of equal size (Type A, Hurwitz and Robert’s classification), and the leaflets were thin and mobile. Central mild aortic valve regurgitation was detected with a vena contracta of 4 mm. Left ventricular dimension and systolic function were normal. There was no additional intracardiac pathology. Echocardiographic examination of ascending aorta were normal (24 mm, z score: +1.21) (Fig 2a–c). Coronary arteries were normal. The patient’s history, clinic, and laboratory findings were insufficient for the diagnosis of rheumatic fever. The patient recognised an isolated quadricuspid aortic valve with mild aortic valve regurgitation. She was advised to follow-up at intervals of 6 months at the outpatient cardiology clinic for an aortic valve regurgitation. Consent was obtained from the patient’s parent for this case study.
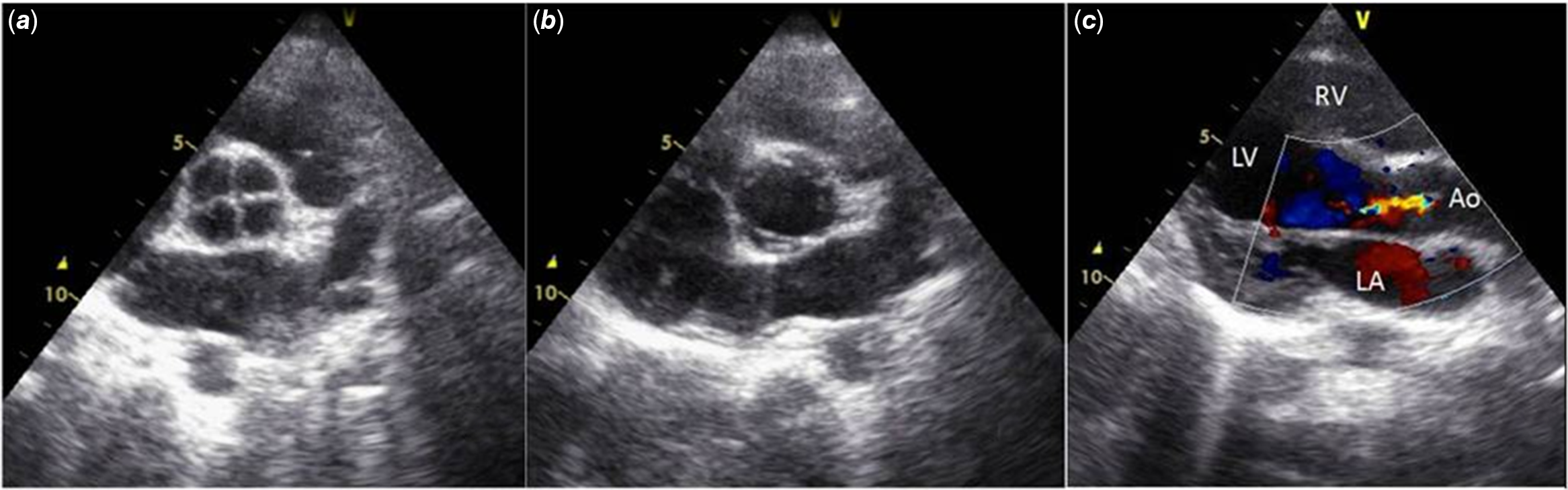
Figure 2. (a, b, and c) Transthoracic echocardiogram in parasternal short-axis view demonstrating (a) quadricuspid aortic valve with four equally cusps in diastole, (b) rectangular shaped opening in systole, (c) central mild aortic valve regurgitation.
Discussion
Aortic valve development begins at approximately days 31–35 from the endocardial cushions in the outflow tract and atrioventricular canal of the primitive heart tube. Cavitation of the cushions results in a central lumen of each cushion that separates the three-valve leaflets.Reference Spicer, Bridgeman, Brown, Mohun and Anderson5
The bicuspid aortic valve develops when the excessive fusion of ridges results in conjoined leaflets with two commissures. When more leaflets have fused, this situation results in a unicuspid aortic valve. Two forms of unicuspid aortic valve have been described, the unicommissural variant which is characterised by one commissure, the presence of a lateral attachment to the aorta with an eccentric orifice and the acommissural form in case of the absence of such attachment and presence of a central orifice.Reference Essandoh, Castellon-Larios, Zuleta-Alarcon, Portillo and Crestanello6 In their recently published article, Slostad et alReference Slostad, Witt and O’Leary7 reported that they detected unicommissural type unicuspid aortic valve in 100% of 75 patients after surgery and autopsy. In some patients, it is difficult to make a differential diagnosis on echocardiography from the bicuspid aortic valve. However, Ewen et alReference Ewen, Karliova and Weber8 defined major and minor criteria for the echocardiographic diagnosis of the unicuspid aortic valve. Criteria are as follows: (I) single commissural attachment zone, (II) rounded, leaflet-free edge on the opposite side of the commissural attachment zone, (III) eccentric valvular orifice during systole, and (IV) patient age <20 years and mean transvalvular gradient >15 mmHg. The minor criteria were defined as an associated thoracic aortopathy and age <40 years. They claimed that three of the four main criteria or two of the four main criteria and one minor criterion distinguish unicuspid aortic valve patients from the bicuspid aortic valve or tricuspid aortic valve with high sensitivity and specifcity.Reference Ewen, Karliova and Weber8 The present case is of the unicommissural type unicuspid aortic valve with a single commissural attachment zone, a rounded, leaflet-free edge, and an eccentric orifice causing a slight narrowing of the aortic valve area. There may be a phenotypic continuum of similar disease between bicuspid and unicuspid aortic valves; however, in the unicuspid aortic valve, there is more smaller indexed aortic valve area that correlates with the lower number of cusps than bicuspid aortic valve.Reference Krepp, Roman and Devereux2 In addition, acommissural valves have a smaller effective orifice area than unicommissural valves and often presents at a younger age due to severe stenosis.Reference Armstrong, Crawford and Arnautovic9
Trileaflet aortic valve is formed by the excavation of the mesenchymal ridge in three areas. Quadricuspid aortic valve may develop when one of these three mesenchymal ridges divides to form an additional leaflet.Reference Fernández, Durán, Martire, López and Sans-Coma10 Two classifications are usually used to describe quadricuspid aortic valves. In the first classification, Hurwitz and Roberts introduced the classification system in which seven subtypes, named A to G by the relative size of the four cusps. The most common types consist of four equal cusps (type A) and three equally sized cusps and one smaller cusp (type B) (both, 73% of all cases).Reference Hurwitz and Roberts11 In the second classification, Nakamura et al provided a simplified classification into four types based on the position of the supernumerary cusp.Reference Nakamura, Taniguchi, Saiki, Morimoto and Yamaga12 It is important to note that the position of the accessory cusp has no effect on the severity of the valvular regurgitation.Reference Tsang, Abudiab and Ammash13 The characteristic echocardiographic finding in the short-axis view is an X-shaped commissure pattern during diastole and a rectangular appearance during systole. The present case was showed a quadricuspid aortic valve classified as type A (four relatively equal cusps) in accordance with the Hurwitz and Roberts’ classification. No thickness and calcification were found.
Unicuspid and quadricuspid aortic valves have similar clinical presentations (aortic stenosis or regurgitation) with the bicuspid aortic valve.Reference Krepp, Roman and Devereux2 Because unicuspid aortic valve had a smaller indexed aortic valve area, most often present with aortic stenosis, with or without aortic valve regurgitation (93% mixed with aortic valve regurgitation, 7% isolated).Reference Slostad, Witt and O’Leary7 Aortic valve stenosis tends to start earlier and progress more rapidly in patients with the unicuspid aortic valve. Slostad et alReference Slostad, Witt and O’Leary7 reported that 71 of the 75 patients with the unicuspid aortic valve needed aortic valve surgery during a median clinical follow-up of 13.2 years. Additionally, unicuspid aortic valve patients had greater mean and peak aortic valve gradients than the bicuspid aortic valve.Reference Krepp, Roman and Devereux2 In the present case, there is moderate aortic valve stenosis with mildly narrowed aortic valve area and mild aortic valve regurgitation, which requires close clinical follow-up. The quadricuspid aortic valve tends to present with aortic valve regurgitation due to incomplete coaptation of the valve leaflets. Aortic valve stenosis has been described more rarely (90% versus 8%, respectively).Reference Tsang, Abudiab and Ammash13 The present case of the quadricuspid aortic valve has mild aortic valve regurgitation due to incomplete coaptation of four cusps with thin and mobile leaflets.
Both unicuspid and quadricuspid aortic valves usually appear as an isolated congenital anomaly, but may also be associated with other abnormalities. Slostad et alReference Slostad, Witt and O’Leary7 reported that, 27% of the patients with the unicuspid aortic valve, had additional structural cardiac comorbidities, including patent foramen ovale, coarctation of the aorta, hypertrophic cardiomyopathy, aortic dissection. Additionally, interatrialReference Saito, Yoshimura, Miyatsu and Ikeda14,Reference Ermis, Bilgi, Altay and Erol15 and/or interventricular septal defect,Reference Demirkol, Balta, Arslan, Unlu, Kucuk and Iyisoy16,Reference Ishigami, Iwase and Hyoudo17 Fallot tetralogy,Reference Maheshwari, Tanwar and Mittal18 truncus arteriosus,Reference Franco, Gabriel and Ruehm19 coarctation of the aorta,Reference Agrawal, Kalavakunta and Gupta20 Turner syndrome,Reference Essandoh, Castellon-Larios, Zuleta-Alarcon, Portillo and Crestanello6 and Williams syndromeReference Gouveia, Martins and Costa21 have been reported in the literature. However, unicuspid and quadricuspid aortic valves are most frequently associated with coronary abnormalities, such as a single coronary artery, origin and/or course abnormalities of coronary arteries.Reference Saito, Takaoka and Funabashi22 In addition, infective endocarditis has been reported in both unicuspid and quadricuspid aortic valves.Reference Yuzawa-Tsukada, Tanaka and Morimoto23,Reference Jackson, Sarwar, Hwang, Joglekar and Alsafwah24 While aortic valve disease was the only complication in the patient with quadricuspid aortic valve; aortic valve disease was accompanied by mitral valve prolapse and mild mitral valve regurgitation in the patient with the unicuspid aortic valve.
Aortic stenosis changes the jet of fluid emerging from the aortic valve leading to an increased risk for aortic dilatations, and aortic dissection. Because of the earlier presentation and increased likelihood of more severe stenosis, unicuspid aortic valves manifest with an increased incidence of ascending aorta dilatation,Reference Slostad, Witt and O’Leary7 and aortic complications than the bicuspid and quadricuspid aortic valves.Reference Krepp, Roman and Devereux2,Reference Naito, Sequeira-Gross, Petersen, Holst, Reichenspurner and Girdauskas25 In accordance with the literature, aortic dilatation was present in the patient with the unicuspid aortic valve, while aortic measurements were normal in the patient with the quadricuspid aortic valve.
Conclusion
Although unicuspid, bicuspid, and quadricuspid aortic valves have distinctly different morphologies, they cause similar pathological and clinical findings. However, aortic stenosis and aortic complications tend to occur earlier and more aggressive phenotype in those patients with the unicuspid aortic valve. Adopting the current recommendations of the bicuspid aortic valve guideline for these patients would be appropriate in the close management and monitoring of both aortic valve and aortic complications.Reference Naito, Sequeira-Gross, Petersen, Holst, Reichenspurner and Girdauskas25 While evaluating these patients, it is necessary to clearly demonstrate the coronary arteries, especially for patients who will undergo surgery, as well as other possible intracardiac pathologies.
Acknowledgements
None.
Financial support
This research received no specific grant from any funding agency, commercial, or not-for-profit sectors.
Conflicts of interest
None.
Ethical standards
The study was approved by our hospital’s ethics committee.


