



Case
Transcatheter closure of patent ductus arteriosus in very low birth weight infants is exclusively performed through the transfemoral venous approach. Transjugular venous approach for transcatheter patent ductus arteriosus closure has previously been described in older paediatric patients but not in a very low birth weight infant. Reference Fernandes1 The presented case is a 1.4 kg premature female who underwent transcatheter patent ductus arteriosus closure at 4 weeks of life. Upon obtaining femoral vein access, interruption of the inferior vena cava with azygous continuation was discovered. The decision was made to use a transjugular venous approach. Right internal jugular venous access was obtained, and a 4-Fr prelude sheath (Merit Medical, South Jordan, Utah) was placed. Retrospectively, we think that flipping the baby 180° may have provided an easier device deployment. A large patent ductus arteriosus was confirmed by echocardiogram and angiography (Figs 1a and 2a). A 4-2 mm Amplatzer Piccolo patent ductus arteriosus occluder (Abbott, North Chicago, IL) was successfully implanted within the PDA. Delicate and coordinated manoeuvring between two interventional cardiologists was necessary for the device deployment because of the difficulty associated with the transjugular approach. Final imaging showed satisfactory device position without impingement on the left pulmonary artery or the descending aorta (Figs 1b and 2b). Significant tricuspid valve regurgitation caused by the delivery catheter may cause hemodynamic instability using the transjugular approach. However, the patient tolerated the procedure very well in our case and she was able to be extubated the next day.
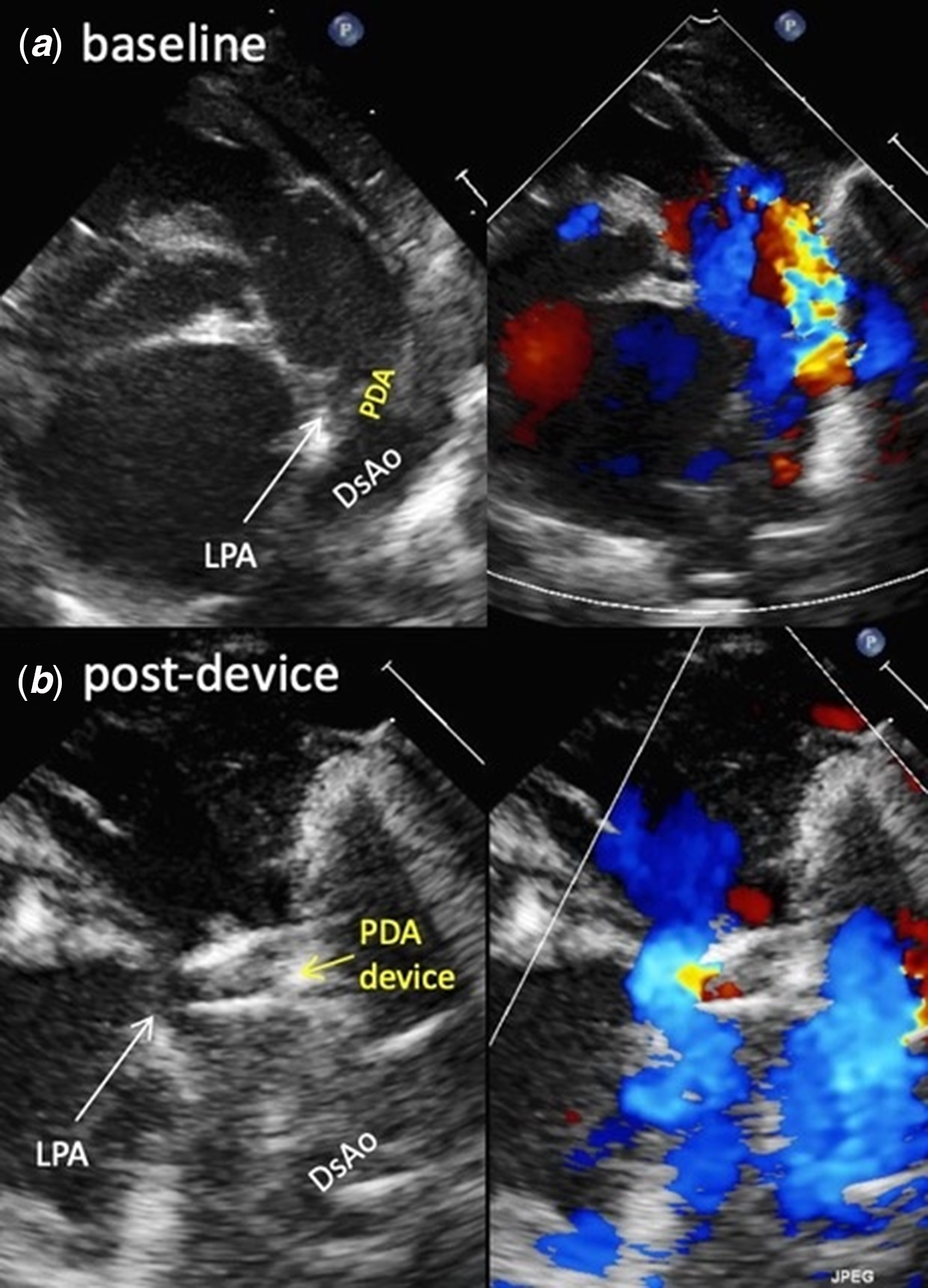
Figure 1. Transthoracic echocardiography. ( a ) Patent ductus arteriosus (PDA) with a large left to right shunt. ( b ) The PDA device is in a satisfactory position with no residual shunt. DsAo, descending aorta; LPA, left pulmonary artery.
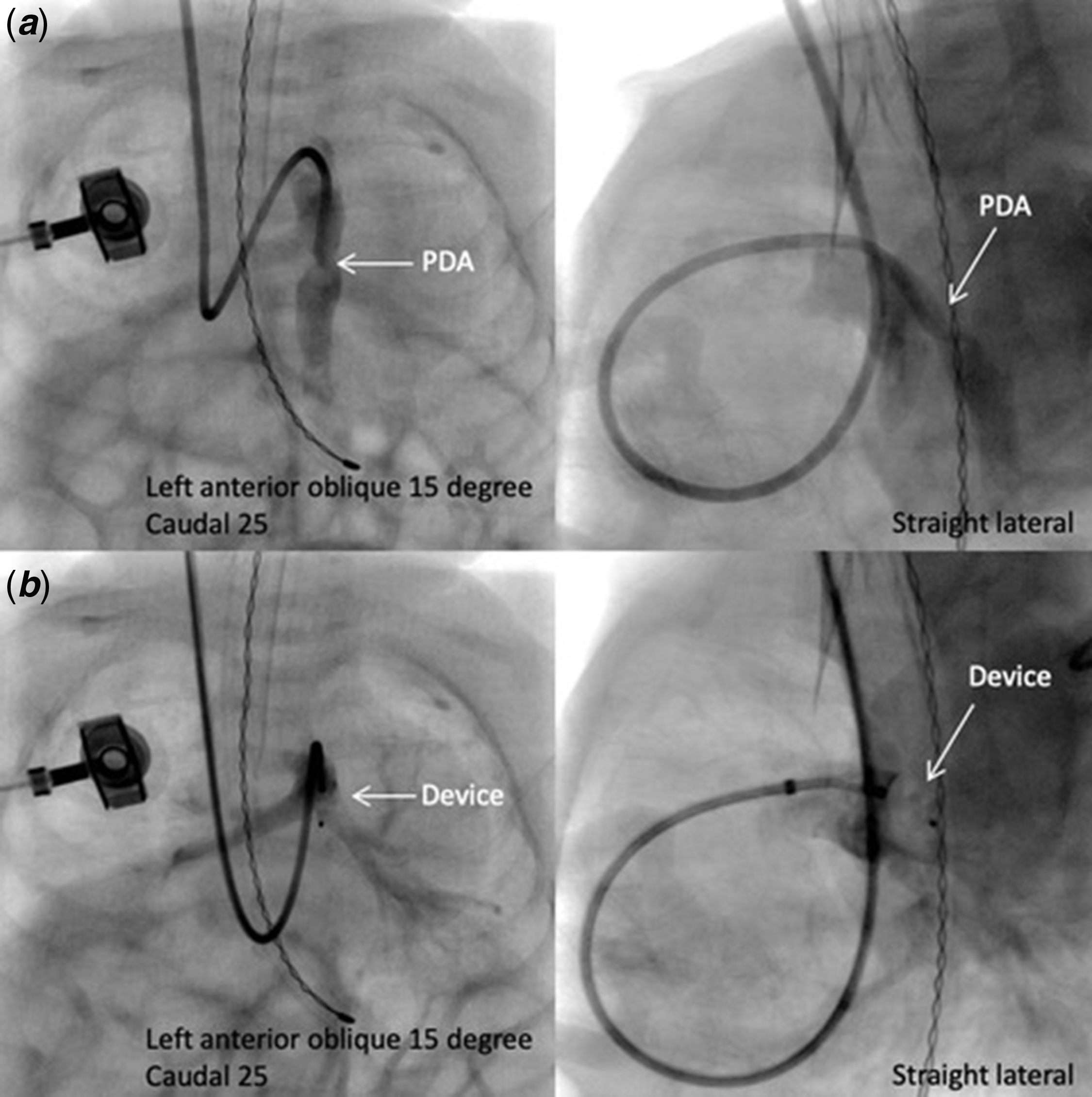
Figure 2. Cardiac catheterisation. ( a ): A 4-Fr Glide catheter courses from the right internal jugular vein to superior vena cava, right atrium and ventricle, main pulmonary artery, and descending aorta through the patent ductus arteriosus (PDA). Baseline descending aortography shows the PDA. ( b ): A 4-2 mm Amplatzer Piccolo PDA occluder is positioned at the PDA. Pulmonary artery angiography shows a satisfactory device position with unobstructed flow to both branch pulmonary arteries.
Acknowledgements
None.
Financial support
This research received no specific grant from any funding agency, commercial, or not-for-profit sectors.
Conflicts of interest
None.
Ethical standards
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in this case report.


