


Case
A 25-year-old with a Fontan circulation presented at 11 weeks gestation with an unplanned pregnancy. Underlying anatomy was dextrocardia, atrioventricular and ventriculoarterial discordance, pulmonary atresia, ventricular septal defect, and bilateral patent arterial ducts. She underwent stent implantation to the ducts, a central shunt, and pulmonary artery augmentation in infancy. Aged 5, an extracardiac fenestrated Fontan was performed. The fenestration was subsequently closed percutaneously.
Two years before conception she underwent cardiac MRI showing patent Fontan pathways (Fig 1a). Left ventricular ejection fraction was 63% and the right 66% (Fig 1b). There was no valve regurgitation. A small collateral was noted from the internal mammary and a leash of collaterals behind the superior vena cava contributing 8–10% of pulmonary venous return.
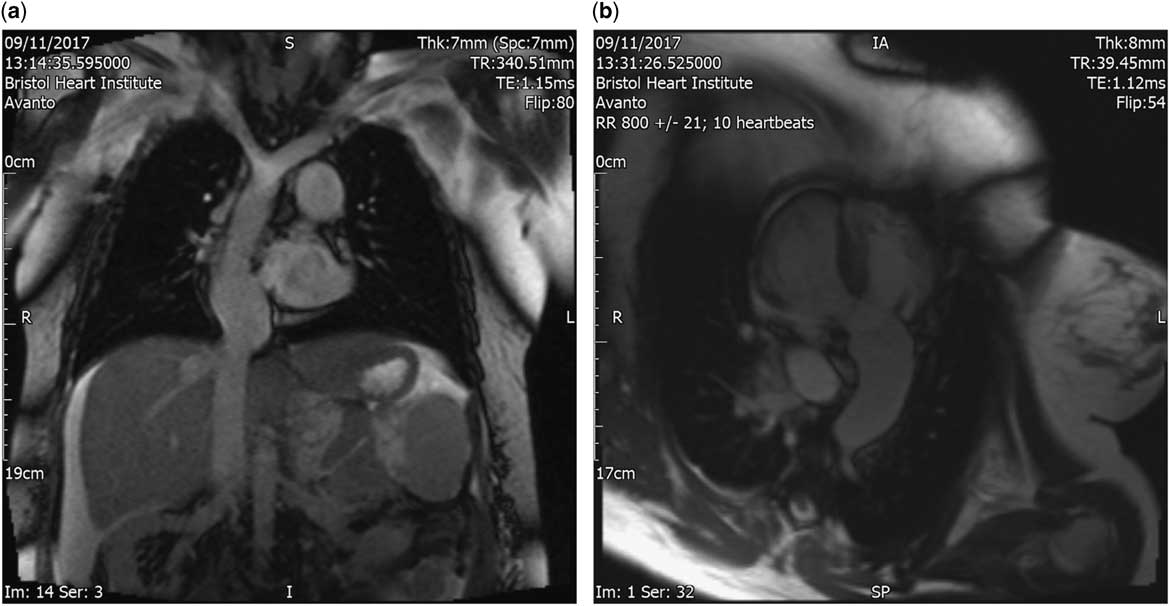
Figure 1 ( a ) Cine MRI image showing total cavopulmonary connection. ( b ) Cine MRI image showing single-ventricle physiology.
VO2 max was 53% predicted on cardiopulmonary exercise testing. Baseline oxygen saturations were 94 and 93% at peak exercise. Bloodwork revealed normal renal and liver function and brain natriuretic peptide. Haemoglobin was 143 g/L. Liver ultrasonography and elastography was normal. Contraception was advised, and planned pregnancy recommended.
On presentation she was mildly breathless on exertion, though had gained 8 kg over the previous year. She was taking aspirin 75 mg a day. She was normotensive with no murmurs. There was no fluid retention or hepatomegaly. Oxygen saturations were 94%. Blood pressure was 128/64. ECG showed sinus rhythm, right-axis deviation, and T-wave inversion in V1-V4. Echocardiography showed good ventricular function, no valvar regurgitation, no outflow tract obstruction, and low velocity phasic flow in the Fontan.
She and her partner were keen to continue the pregnancy and accepted the risks of prematurity, possible fetal loss, intrauterine growth restriction, post-partum haemorrhage, deterioration of cardiac function, and arrhythmias. The aspirin was changed to low molecular weight heparin 1 mg/kg twice a day.
At 15 weeks gestation, owing to abnormal quad testing the fetus was scanned and was found to be severely growth restricted with a large abnormal placenta with placental lakes. The patient described new peripheral oedema, orthopnoea, fever, and rigors. On examination she had oedema to the mid abdomen. Pulse was 88 beats per minute and regular; blood pressure was 142/74. Auscultation of heart and lungs was normal. ECG showed sinus rhythm and echocardiography was unchanged. Oxygen saturations were 94%.
Differential diagnosis included pre-eclampsia, Mirror Syndrome, Fontan failure, or sepsis. Blood tests showed a normal urea, creatinine and electrolytes, liver function, clotting, full blood count, and C-reactive protein. Amniocentesis showed a normal fetal karyotype. MRI showed patent Fontan pathways with small bilateral pleural effusions. Liver ultrasound showed dilated hepatic veins. The urine grew Escherichia coli, and the diagnosis of a urinary tract infection on the background of a struggling Fontan was made. She improved with antibiotics and bed rest and was discharged a week later on methyldopa 250 mg twice a day.
One week later, she re-attended with persistent peripheral oedema. Blood pressure was 140/90, oxygen saturations 93%, and echocardiography unchanged. Fetal sonography showed a large, grossly abnormal placenta, reduced liquor, and severe intrauterine growth restriction. She was told that it was unlikely that the fetus would survive to a viable gestation, but declined termination. She was prescribed sildenafil 25 mg three times a day, furosemide 40 mg a day, and methyldopa was doubled in an attempt to improve cardiac output.
Two weeks later, at 18 weeks gestation, she presented with spontaneous rupture of membranes and worsening peripheral oedema and sadly miscarried.
Discussion
Many women with CHD have successful pregnanciesReference Greutmann and Pieper 1 and risk factors are well-described,Reference Thorne, MacGregor and Nelson-Piercy 2 , Reference Drenthen, Boersma and Balci 3 but the risk in complex hearts is not well understood.
The Fontan operation is used to palliate congenital heart lesions that cannot support a biventricular circulation in order to decrease volume overload on the ventricle and eliminate cyanosis.Reference Gewillig and Brown 4 Despite its success, the Fontan physiology has its drawbacks as a low and fixed cardiac output driven by the pulmonary vascular resistance, leading to an inherent limitation in the heart’s ability to augment cardiac output.Reference Gewillig and Brown 4
Existing literature suggests that fetal outcomes are poor in the pregnant Fontan but that maternal risk is comparatively low. Maternal risks include bleeding, arrhythmia, and heart failure but fetal loss is disproportionally high with reported rates of miscarriage from 27 to 69%, and small for gestation age infants and prematurity rates of up to 92%.Reference Canobbio, Mair, van der Velde and Koos 5 – Reference Cauldwell, Steer and Bonner 10
Poor fetal outcomes are thought to be due to a combination of cyanosis, anticoagulation, and suboptimal haemodynamics.Reference Canobbio, Mair, van der Velde and Koos 5 – Reference Cauldwell, Steer and Bonner 10 A recent risk stratification model divided patients into three risk groups: lower, intermediate, and very high, based on the functional class, ventricular function, exercise tolerance, oxygen saturations, and the presence or absence of atrioventricular valve regurgitation.Reference Arif, Chaudhary and Paul 9 Lower risk women had a trend towards a higher percentage of live births, but this was not significant. Clearly fetal outcome is more complex and not just dependent on the mother’s functional state. Our patient was lower risk, according to this model, yet her outcome was poor.
Deep cyanosis results in almost certain miscarriage in Fontan pregnancies,Reference Cauldwell, Steer and Bonner 10 but the bigger risk may lie with the fundamental low cardiac output state. Gewillig has written eloquently about the limitation of using contractility as a measure of good Fontan function. The ventricle can only pump the blood that is delivered to it by the Fontan; when this is limited it reacts by increasing end-diastolic pressure. The haemodynamic demands of pregnancy are profound: a 20% increase in myocardial oxygen consumption, 30–40% increase in blood volume, and 15–20% increase in heart rate. It is feasible that a Fontan circulation faced with these demands enters a vicious cycle: the relative reduction in cardiac output results in further vasoconstriction and an increase in systemic vascular resistance, which causes increased afterload and further poor Fontan forward flow.
We suggest that good systolic ventricular function in Fontan patients is not necessarily predictive of a good outcome in pregnancy. It is essential to measure the Fontan pressure and end-diastolic pressure as well as comprehensively assessing the pulmonary vasculature pre-pregnancy. No Fontan pregnancy can be considered low risk and women need to be aware that miscarriage and fetal death are possible, even if they are deemed “lower risk”. Egg harvest for surrogacy is also not without risk. Appropriate advice around assisted reproduction and effective contraception is essential in these patients.
Financial Support
This research received no specific grant from any funding agency, or from commercial or not-for-profit sectors.
Conflicts of Interest
None.

