Retroaortic innominate veins are a rare finding most often associated with congenital cardiac defects. They are most commonly seen in patients with tetralogy of fallot and in those with a right aortic arch. They may lead to compression of the superior caval vein if left in its original aberrant position at the time of surgical repair.
Case report
We present the case of a male patient with an antenatal diagnosis of transposition of the great vessels with intact ventricular septum. Fetal echocardiography confirmed the diagnosis at 25 weeks gestational age. He was born by spontaneous vaginal delivery at 36 weeks gestation with a birth weight of 3.3 kg. His Apgar score was 7 at 1 minute and 9 at 5 minutes of age. No resuscitation was required and his oxygen saturations increased to 80% at 10 minutes of age on both pre- and post-ductal monitoring.
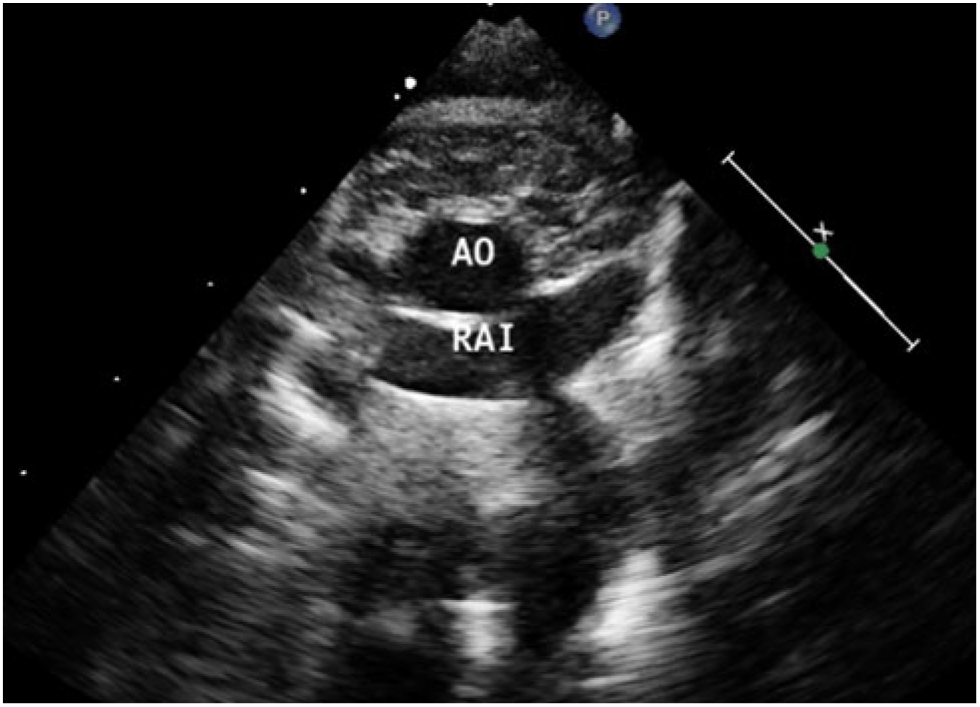
He was subsequently transferred to a tertiary cardiology care centre on prostin 5 ng/kg/minute and was clinically stable on arrival. His echocardiogram revealed a restrictive atrial septal communication (3 mm) with a left to right shunt angled superiorly through the patent foramen ovale. Of note, a retroaortic innominate vein was also identified (Fig. 1). The patient remained clinically stable overnight, with oxygen saturations remaining above 80% and serum lactate levels below 2.5. As a result, balloon atrial septostomy was not performed, and the patient was taken to theatre the following morning.
Cardiopulmonary bypass was initiated following cannulation of the superior and inferior caval vein and ascending aorta. The atrial septal defect was closed. An arterial switch operation with a Lecompte manoeuvre was then performed. The aberrant course of the retroaortic innominate vein was identified. The vein was mobilised along its length in both directions and the innominate vein was incorporated into the Lecompte manoeuvre with translocation anterior to the aorta (Fig. 2). The patient had a bypass time of 133 minutes and a cross clamp time of 77 minutes.
The patient had a slow post-operative recovery with an isolated rise in serum creatinine. Serial renal ultrasound scans demonstrated normal appearing kidneys. He had a prolonged inotrope wean and was discharged from the intensive care unit on day 8 following surgery. He remained clinically stable on the ward and was discharged home on post-operative day 18. Post-operatively and on subsequent out-patient review, no evidence of superior caval vein obstruction has been identified.
Discussion
Retroaortic innominate veins are a rare entity where the left innominate vein courses horizontally behind the ascending aorta before joining the superior caval vein below the azygous vein insertion. This finding was first reported by Kershner in 1888. They are typically associated with other cardiac lesions although isolated findings of retroaortic innominate veins without other cardiac pathology have been noted.Reference Srinivasan, Kannivelu, Ali and See 1 Its incidence has been reported at 0.5% in patients with congenital cardiac defectsReference Curtil, Tronc, Champsaur, Bozio, Sassolas and Carret 2 and it is most commonly seen in patients with tetralogy of fallot, especially when associated with a right aortic arch.Reference Changela, John and Maheshwari 3 , Reference Kulkarni, Jain, Kasar, Garekar and Joshi 4 We believe that this is the first case to describe a retroaortic innominate vein in a patient with transposition of the great arteries.
The presence of a retroaortic innominate vein usually has no clinical implications. However, in certain circumstances cardiothoracic surgical repair may be complicated by their presence. The abnormal connection of the retroaortic innominate vein to the superior caval vein may hinder mobilisation of the superior caval vein in patients undertaking cavopulmonary anastomosis.Reference Koutlas, Wernovsky, Slack, Weinberg and Spray 5 Rarely, the risk of compression to the innominate vein must be considered at the time of surgery. A case report by Konstantinov et al describes a newborn infant with coarctation of the aorta and a retroaortic innominate vein. At surgery, following transection of the aorta, they opted to relocate the innominate vein anterior to the aorta to avoid venous compression.Reference Konstantinov, Van Arsdell, O’Blenes, Roy and Campbell 6 We undertook a similar strategy in our patient, incorporating the innominate vein into the Lecompte manoeuvre, removing the risk of venous compression and superior caval vein syndrome if this was ignored. Mobilisation of the retroaortic innominate vein is not technically challenging in this context as the great vessels are transected during the switch procedure.
Superior caval vein compression has been described in a case report by Kalra et al.Reference Kalra, Joshi, Joshi and Aggarwal 7 Their patient presented with tetralogy of fallot with absent pulmonary valve and a retroaortic innominate vein. They performed a Lecompte procedure to alleviate airway compression of the left main bronchus. The patient developed superior caval vein syndrome in the post-operative period secondary to compression of the retroaortic innominate vein. They subsequently advocated for anterior re-location of the anomalous vein during the Lecompte manoeuvre. Our group would support this approach.
Conclusion
Retroaortic innominate veins may occur in patients with transposition of the great vessels. We recommend incorporation of the retroaortic innominate vein into the Lecompte manoeuvre to avoid the risk of venous compression and the development of superior caval vein syndrome.

Figure 1. The retroaortic innominate vein (RAI) is displayed coursing behind the aortic arch (Ao).

Figure 2. The right image demonstrates the pre-operative anatomy with the retroaortic innominate vein posterior to the aorta. The left image demonstrates the post-operative result with the innominate vein and pulmonary artery moved anterior to the neo-aorta.
Financial Support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Conflicts of Interest
None.