CHD is present in 0.5–1% of newborns and infants; 7–10% of patients are born with congenital pulmonary valve stenosis.Reference Hoffman and Kaplan 1 , Reference Kan, White, Mitchell and Gardner 2 The right ventricle usually adapts well to pulmonary valve stenosis, even when severe, with symptoms being unusual in children and adolescents. Eventually, longstanding untreatable severe obstruction may lead to right ventricular failure and tricuspid regurgitation. 3 In the case of chronic pressure overload, the wall thickness greatly increases as new sarcomeres are added parallel to the existing sarcomeres. This type of ventricle is capable of generating greater forces and higher pressures, whereas the increased wall thickness maintains normal wall stress. The ventricle becomes “stiff” – that is, its compliance is reduced – which can impair filling and lead to diastolic dysfunction. 3 The fundamental abnormality of restrictive right ventricular physiology – that is, the presence of antegrade pulmonary arterial flow in late diastole throughout the respiratory cycle – is reduced right ventricular compliance as a result of longstanding pressure overload.Reference Redington, Penny, Rigby and Hayes 4 Data are scanty to address the impact of chronic increase in right ventricular outflow resistance on right ventricular diastolic performance.Reference Redington, Penny, Rigby and Hayes 4 The right ventricular filling indices measured by pulsed-wave Doppler – peak E-wave and A-wave velocities, E-wave deceleration time, and isovolumic relaxation time – have the drawbacks of heart rate and load dependency as well as the lack of generally acceptable reference values, particularly for different age groups,Reference Horton, Meece and Hill 5 whereas tissue Doppler imaging velocities and right ventricular long-axis systolic amplitudes have been validated as surrogate markers of right ventricular function.Reference Horton, Meece and Hill 5 The right ventricular restrictive filling pattern – antegrade pulmonary arterial flow in late diastole –Reference Redington, Penny, Rigby and Hayes 4 predicted post-operative outcomesReference Cullen, Shore and Redington 6 and long-term right ventricular restriction in repaired tetralogy of Fallot as a result of longstanding pressure overload.Reference Redington, Penny, Rigby and Hayes 4 This late diastolic flow in the pulmonary artery coincides with premature pulmonary valve opening.Reference Redington, Penny, Rigby and Hayes 4 Simultaneous catheter pressure monitoring demonstrated that this flow occurred when the right ventricular end diastolic pressure was equal to or exceeded the pulmonary arterial diastolic pressure.Reference Redington, Penny, Rigby and Hayes 4 , Reference Kisanuki, Tei and Otsuji 7 Such findings suggested that the right ventricular compliance fell and the cavity became stiff and therefore acted as a passive conduit between the right atrium and the pulmonary artery during atrial systole.Reference Redington, Penny, Rigby and Hayes 4 Right ventricular diastolic function has been shown to predate clinical systolic dysfunction, and right ventricular diastolic parameters may represent a screening tool in patients at risk for developing right ventricular dysfunction. Late gadolinium enhancement is a method where cardiovascular MRIs are obtained after administration of gadolinium contrast material that accumulates into a tissue with increased extra-cellular space; this method is suggestive of fibrosis in both right and left ventricles.Reference Babu-Narayan, Goktekin and Moon 8 In addition, evolving clinical applications include stain analysis using myocardial tagging and diastology assessment using phase-contrast cardiac magnetic resonance to measure the deceleration time and isovolumic relaxation time.Reference Rathi and Biederman 9 The aim of this study was to establish whether late gadolinium enhancement was present in patients with restrictive right ventricular physiology, after balloon valvuloplasty for critical pulmonary valve stenosis. We also studied whether the patient’s age, right ventricular end diastolic volume, and right ventricular mass index correlated with late gadolinium enhancement.
Methods
Study population
This study included a total of 44 patients with isolated critical pulmonary valve stenosis. Patients underwent balloon pulmonary valvuloplasty between 2008 and 2012 at the National Heart Institute in Cairo. The inclusion criteria were cyanosis, restrictive right ventricular physiology, right ventricular systolic dysfunction, and right ventricular failure. The NYHA functional class, other cardiovascular symptoms, and co-morbidities were recorded. Repeated pulmonary valvuloplasty was successfully performed in five patients who had residual stenosis after initial valvuloplasty.
A subset of the studied population (n=33 patients) who were able to return to our institute for follow-up (6–60 months) underwent further detailed imaging by echocardiography. Some of the patients with right ventricular dysfunction referred from southern Egypt and remote areas, who were once rehabilitated, were not keen for follow-up. Included results were compared with 33 controls matched for age and gender, and comprised children and adolescents randomly sampled from our database with a structurally normal hearts and without a history of cardiovascular diseases.
Out of 33 patients, 21 underwent cardiac MRI with late gadolinium enhancement to assess the presence of right ventricular fibrosis. We also studied whether the patient’s age, right ventricular end diastolic volume ml/m2, and right ventricular mass g/m2 correlate with late gadolinium enhancement.
Invasive pressure monitoring
We applied a standard technique for pulmonary valvuloplasty using a balloon over a guide wire technique, through the femoral vein approach, as first described by Kan et alReference Kan, White, Mitchell and Gardner 2 and Al Kassab et alReference Al Kassab, Ribeiro, AlZaibag, Halim and Shahid 10 Initially, right ventricular angiography was carried out with a pigtail catheter. Haemodynamic data were recorded during catheterisation with an end-hole catheter under blood pressure monitoring. Some patients with impaired systolic function needed dopamine support. Right atrial mean pressure, right ventricular systolic and end diastolic pressure, and pulmonary artery systolic and end diastolic pressure were measured before and after balloon valvuloplasty. Single-balloon technique was performed in 30 patients with balloon size 1.3 times the annulus diameter. Double-balloon techniqueReference Park, Yoon and Yeon 11 was performed in 14 patients with balloon size 0.65 times the annulus diameter using guiding catheter (launcher) 6th Fr Catheter, which accepts two guide wires 0.35 Fr. After balloon valvuloplasty, the haemodynamic data were checked, and right ventriculogram was performed again for the final result.
Echocardiographic assessment
A subset of 33 patients from the population was able to return to our institute for follow-up. All of them underwent two-dimensional color flow Doppler and spectral Doppler examination. When necessary, younger patients were sedated to facilitate examination. Transthoracic imaging of the heart was performed using a commercially available ultrasound system Vivid 3 (General Electric/Vingmed ultrasound, Horten, Norway). At least three consecutive beats in sinus rhythm were recorded and the average value was considered; two-dimensional images were obtained from the apical four-chamber view for the determination of right ventricular end diastolic and end systolic area.Reference Horton, Meece and Hill
5
The change in right ventricular fractional area is expressed as percentage change in the right ventricular chamber area from end diastole to end systole, and is calculated as follows:
 ${{{\rm end}\,{\rm diastolic}\,{\rm area}\,{\rm (cm}^{{\rm 2}} {\rm )}\,-{\rm {\hyphen}}\,{\rm end}\,{\rm systolic}\,{\rm area}\,{\rm (cm}^{{\rm 2}} {\rm )}} \over {{\rm end}\,{\rm diastolic}\,{\rm area \ (cm}^{{\rm 2}} {\rm )}}}\,\%\,.$
Reference Horton, Meece and Hill
5
The right ventricular free wall thickness was measured from the apical and sub-costal views.Reference Matsukubo, Matsuura, Endo, Asayama and Watanbe
12
M-mode measurements were made from the parasternal short-axis view at the level of the tips of the papillary muscles, with placement of the M-mode cursor, guided by two-dimensional imaging and by using the leading edge-to-leading edge technique.Reference Kampmann, Wiethoff and Wenzel
13
Measurements of the left ventricular end systolic, end diastolic and right ventricular end diastolic dimensions were calculated in cm and Z scores.Reference Pettersen, Wei, Skeens and Humes
14
Data of M-mode were available before valvuloplasty and during follow-up for the 33 patients who came for follow-up.
${{{\rm end}\,{\rm diastolic}\,{\rm area}\,{\rm (cm}^{{\rm 2}} {\rm )}\,-{\rm {\hyphen}}\,{\rm end}\,{\rm systolic}\,{\rm area}\,{\rm (cm}^{{\rm 2}} {\rm )}} \over {{\rm end}\,{\rm diastolic}\,{\rm area \ (cm}^{{\rm 2}} {\rm )}}}\,\%\,.$
Reference Horton, Meece and Hill
5
The right ventricular free wall thickness was measured from the apical and sub-costal views.Reference Matsukubo, Matsuura, Endo, Asayama and Watanbe
12
M-mode measurements were made from the parasternal short-axis view at the level of the tips of the papillary muscles, with placement of the M-mode cursor, guided by two-dimensional imaging and by using the leading edge-to-leading edge technique.Reference Kampmann, Wiethoff and Wenzel
13
Measurements of the left ventricular end systolic, end diastolic and right ventricular end diastolic dimensions were calculated in cm and Z scores.Reference Pettersen, Wei, Skeens and Humes
14
Data of M-mode were available before valvuloplasty and during follow-up for the 33 patients who came for follow-up.
Echocardiographic data (two-dimensional views) describing the right ventricle were categorised as follows:
-
∙ A normal right ventricle – that is, left ventricle to right ventricle ratio of 3:1.
-
∙ Severely dilated right ventricle – that is, right ventricular dimension equal or even exceeding the left ventricular dimension.
-
∙ Anything in between was classified as a mildly dilated right ventricle.Reference De Ruijter, Weenin, Hitchcock, Meijboom and Bennink 15
Pulsed-wave Doppler of the pulmonary arterial flow was obtained with the sample volume 1 cm distal to the pulmonary valve.Reference Redington, Penny, Rigby and Hayes 4 , Reference Cullen, Shore and Redington 6 , Reference Kisanuki, Tei and Otsuji 7 Peak pulmonary valve gradient was measured from continuous wave Doppler recording from parasternal short axis at the pulmonary valve level by modified Bernoulli equation.Reference Johnson, Kwan, Handshoe, Noonan and DeMaria 16 , Reference Silvilairat, Cabalka, Cetta, Hagler and O’Leary 17 The right ventricular filling indices were obtained by placing a 2-mm pulsed-wave Doppler sample volume at the tip of the tricuspid valve leaflet from apical four-chamber view. Peak early diastolic velocity E-wave and late diastolic velocity A-wave and the E/A ratio were then measured.Reference Horton, Meece and Hill 5
The Right ventricular free wall was imaged from the apex during quiet breathing. Colour-coded velocities of the tricuspid annulus were recorded. Myocardial velocities during early diastole (Ea), late diastole (Aa), and peak myocardial velocity during systole (Sa) were measured at the lateral tricuspid annulus.Reference Lam, Kaya, Goktekin, Gatzoulis, Henein and Li 18 , Reference Lam, Kaya, Goktekin, Gatzoulis, Li and Henein 19 The E/Ea ratio was calculated as a non-invasive indicator of right ventricular filling pressure.Reference Nageh, Kopelen, Zoghbi, Quinones and Nagueh 20 All recordings were made using a sweep speed of 100 mm/s with an electrocardiogram (lead II) superimposed.
Cardiac MRI
For imaging, a 1.5-T scanner was used, MR system (Gyroscan Intera CV and Achiva; Philips Medical Systems, Best, The Netherlands). Localiser sequences in three orthogonal planes were taken followed by standard cardiac two-, three-, and four-chamber views as well as short-axis cine images in steady-state free precession; typically, 7-mm contiguous slices covering the ventricle from the atrioventricular valve plane to the apex were acquired. The scans were performed using the breath-hold technique; scan time per slice was 9–13 seconds with up to 1 minute between scans for the patient to recover between successive breath-holds.Reference Babu-Narayan, Kilner and Li 21 , Reference Lorenz 22
Contrast media (gadolinium–diethylenetriamine pentaacetic acid) was injected intravenously of about 0.2 mmol/kg body weight with acquisition of real-time retrospective gated dynamic cine short-axis view in three slices in free breathing fashion (at rest). Subsequently, late gadolinium enhancement images were obtained 10 minutes after the injection of the contrast material using an inversion recovery sequence. Imaging of the left ventricle was from base to the apex, and the acquisition was performed in the short-axis view and in a four-chamber view. Images were acquired during end-expiration breath hold. Acquisition parameters of inversion recovery sequence are repetition time ms/echo time ms, 6.1/3; section thickness, 5 mm; gap, 0 mm; field of view, 361 mm2; matrix, 224; and TI, which are variable for every patient.Reference Babu-Narayan, Kilner and Li 21 , Reference Lorenz 22
Ventricular volumes and mass
Ventricular volume was calculated by summation of the ventricular cavity areas, assessed by manual tracing of the endocardial border on a stack of gradient-echo image sections of a specific time frame, and multiplied by section thickness, with correction for the inter-slice gap. Papillary muscles and the moderator band were not included in the ventricular area. In end systolic frames, epicardial contours were drawn to determine right ventricular free wall mass, excluding the interventricular septum. Ventricular wall volume was calculated as myocardial area – pericardial minus endocardial area – multiplied by the sum of slice and inter-slice gap thickness. A specific gravity of 1.05 g/ml was used for the calculation of ventricular mass.Reference Lorenz 22 , Reference Pennell 23
Functional image analysis
Short-axis cine images were transferred to the off-line workstation (extended work space), Pride software (Philips Medical Systems, DA Best, The Netherlands). Assessment of late gadolinium enhancement was performed using both location and scoring extends of the right ventricular late gadolinium enhancement. The right ventricular wall was divided into six segments in slices aligned in a short axis. The late enhancement images were visually assessed and each segment was graded according to the extent of enhanced myocardium in a given segment as follows: 0=no enhancement, 1=up to 2 cm, 2=2–3 cm, and 3=>3 cm in length. Enhancement seen in trabeculation, including the moderator band, was graded as 0=no enhancement, 1=enhancement of one trabeculation, 2=enhancement of two to four trabeculation, and 3=enhancement of more than four trabeculation. The inferior and superior right ventricular insertion points were originally scored either 0 for the absence or 1 for the presence of visible late gadolinium enhancement. Walls were divided as follows: wall segment 1=anterior right ventricular outflow tact, wall segment 2=anterior right ventricle, wall segment 3=inferior right ventricle, wall segment 4=septal right ventricle, wall segment 5=trabecular wall, and wall segment 6=right ventricular insertion points.Reference Babu-Narayan, Kilner and Li 21
Statistical analysis
Continuous variables are expressed as mean±SD. Echocardiographic indices between patients and controls were compared using an unpaired Student t-test. A p-value<0.05 was considered statistically significant. Correlation was calculated using linear regression. A two-tailed p-value of <0.05 was considered statistically significant. All the statistical analyses were performed using SPSS version 11.5.
Results
Study population
The mean age group of our patients with critical pulmonary valve stenosis was 10±7.7 years (age ranging from 1 month to 33 years), mean weight was 32±22 Kg (weight with a range from 3 to 75 kg), and there were 25 males and 19 females. All patients had restrictive right ventricular physiology pattern, severe pulmonary valve stenosis, right-to-left shunt through patent foreman ovale, and cyanosis. Their mean O2 saturation was 77±6%; 24 out of 44 patients (55%) had severe right ventricular systolic dysfunction, and 10 out of those 24 had pericardial effusion and ascites, elevated liver enzymes, high level of bilirubin, and hypoalbuminaemia. All patients had undergone successful balloon pulmonary valvuloplasty, and repeated dilation was successfully performed in five patients who had residual stenosis after initial valvuloplasty. NYHA improved by 1 to 2 classes (p<0.001). Patients with elevated liver enzymes, elevated bilirubin, hypoalbuminaemia, and ascitis were successfully rehabilitated with normalisation of liver function.
Haemodynamic data
Invasive pressure monitoring is summarised in Table 1. After balloon pulmonary valvuloplasty, the right ventricular systolic pressure fell from 171±46 to 67±20 mmHg (p<0.0001), and the right ventricular outflow tract gradient fell from 148±46 to 40±18 mmHg (p<0.0001). Before balloon pulmonary valvuloplasty, the right ventricular end diastolic pressure was significantly higher (20±6 mmHg) than the pulmonary end diastolic pressure (12±3 mmHg, p<0.0001). Moreover, there was a significant decrease in right ventricular end diastolic pressure to 16±4 mmHg (p<0.0001); however, it remained higher than the pulmonary end diastolic pressure with significant (p<0.0001) value after balloon pulmonary valvuloplasty. There was significant reduction in the ratio of right ventricular/systemic systolic pressure immediately after balloon valvuloplasty from 1.7±0.5 to 0.6±0.2 (p<0.0001).
Table 1 Pressure at catheterisation (n=44).

BPV=balloon pulmonary valvuloplasty; RV=right ventricle
Angiographic finding
All patients had typically dome-shaped pulmonary valve with a rapid narrow jet across the stenotic valve, post-stenotic dilatation of the main pulmonary artery, marked right ventricular trabeculation, and hypertrophy on ventriculography. Severe right ventricular systolic dysfunction was documented in 24 out of 44 (55%) patients, with reduced forward pulmonary flow. Moreover, moderate tricuspid regurgitation was documented in 55% and mild regurgitation in 45% of the patients. After balloon pulmonary valvuloplasty, the transvalvular flow became wider because the valve was no longer narrow with better opening of the leaflet. Repeated angiogram showed better right ventricular function after relief of afterload (Fig 1).

Figure 1 Selective cine angiographic frame of the right ventricle in postero-anterior view of a 4-month-old patient at the time of balloon valvuloplasty. ( a ) Before, severe right ventricular dilatation, trabeculation with reduction of forward pulmonary flow, ( b ) repeated valvuloplasty after 6 months due to residual stenosis, selected cine angiographic frame of the right ventricle showing better right ventricular size and increased forward pulmonary flow.
Follow-up
The 33 patients who came for follow-up underwent active examination by paediatric cardiologists. The mean follow-up of our patients was 40± months period (with a range from 6 to 60 months). The mean age was 10±9 years, with 21males and 12 females; their O2 was maintained at 98%, and all patients were of NYHA class I. The study protocol included two-dimensional color flow Doppler, M-mode echocardiographic measurement for left ventricular dimension at end diastole, end systole, and right ventricular end diastolic dimension. M-mode measurement was available for 33 patients, before balloon valvuloplasty and during follow-up. Table 2 summarises the haemodynamic data of the 33 patients. There was marked improvement in symptoms, three girls got married and delivered normally; 21 out of the 33 patients with restrictive physiology were subjected to cardiac MRI with late gadolinium enhancement to detect the presence of right ventricular fibrosis, which subsequently contributes to the right ventricular stiffness (this was evident by tissue Doppler parameters during follow-up).
Table 2 Haemodynamic data of 33 patients who came for follow-up.

BPV=balloon pulmonary valvuloplasty; RV=right ventricle
Echocardiographic findings
Figure 2 demonstrates M-mode echocardiographic changes for left and right ventricular dimensions before and during follow-up (n=33 patients). The left ventricular end diastolic dimension was 2.7±0.9 cm and it increased to 3.4±0.9 cm (p<0.001); the left ventricular end systolic dimension was 1.4±0.5 cm and it increased to 2.0±0.6 cm (p<0.001); and the right ventricular end diastolic dimension was 2.9±1 cm and it decreased to 1.8±0.5 cm (p<0.01). Table 3 summarises the Z score value for M-mode measurement of the left ventricular dimension at end diastole, end systole, and right ventricular end diastolic dimensions. Figure 3 shows examples of two-dimensional echocardiographic changes of patients with critical pulmonary stenosis, restrictive right ventricular physiology, and right ventricular failure (a1, a2 before valvuloplasty and b1, b2 during follow-up). The mean right ventricular wall thickness was 9±1 mm, which indicates the presence of right ventricular hypertrophy according to the published normal value 5 mm.Reference Matsukubo, Matsuura, Endo, Asayama and Watanbe 12

Figure 2 M-mode echocardiographic changes before and during follow-up: ( a ) left ventricular end diastolic dimension. ( b ) Left ventricular end systolic dimension. ( c ) Right ventricular end diastolic dimension.

Figure 3 Two-dimensional echocardiographic changes of a patient with pulmonary stenosis, restrictive right ventricular physiology, and right ventricular failure. ( a1 ) Parasternal long-axis view, ( a2 ) short-axis view before valvuloplasty, severe right ventricular dilatation, leftward septal displacement with reduced left ventricular volume, ( b1 ) parasternal long-axis view, and ( b2 ) short-axis view during follow-up restoration of normal septal behaviour and increased left ventricular volume.
Table 3 M-mode echocardiographic measurement for left and right ventricular dimension in Z score before and during follow-up.

BPV=balloon pulmonary valvuloplasty; LV=left ventricle; RV=right ventricle
Conventional and tissue Doppler echo findings
Table 4 demonstrates the comparison of echocardiographic parameters between the subset of the population (no=33 patients) and controls. All patients had persistent restrictive right ventricular physiology and significantly larger right ventricular end systolic area (9±4.6 cm2) compared with controls (6.4±2.5 cm, p<0.001). In addition, they had lower fractional area change (mean 38±11%) than controls (49±4%, p<0.001).
Table 4 Comparison of echocardiographic parameters between patients with persistent restrictive RV physiology (no=33) and controls during follow-up.

Aa=peak tricuspid annular velocity during late diastole; Ea=peak tricuspid annular velocity during early diastole; RV=right ventricle; Sa=peak tricuspid annular velocity during systole; TV=tricuspid valve
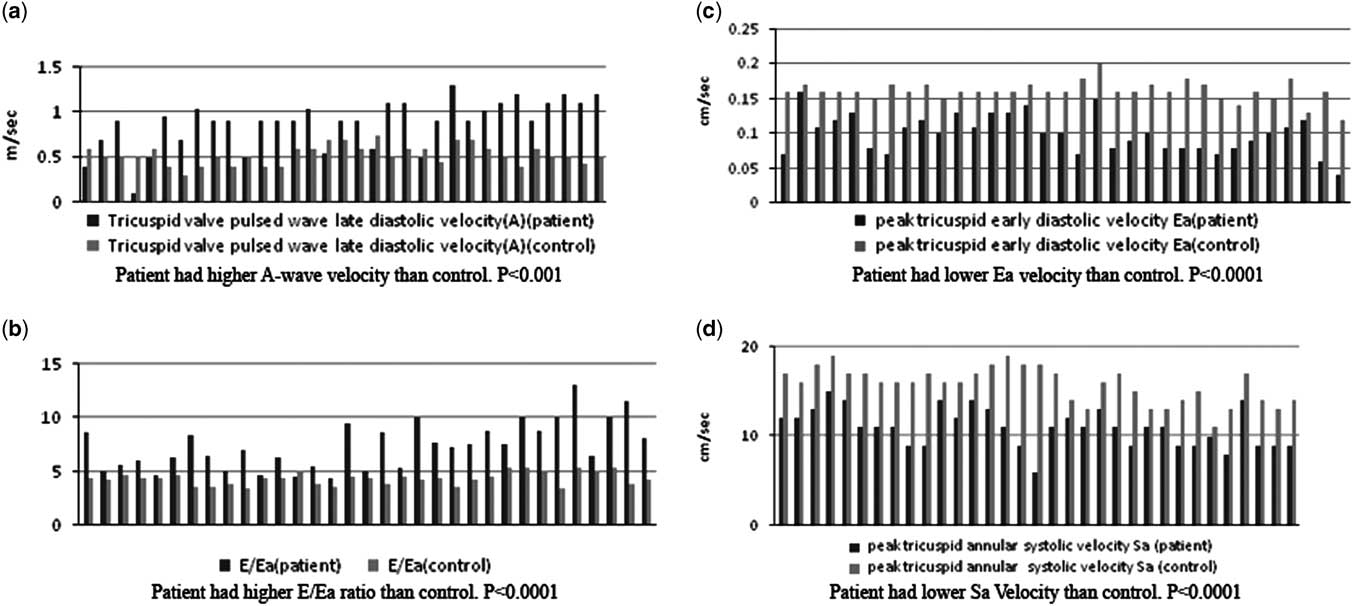
Echocardiographic data (n=33 patient) demonstrated reduction of transvalvular pressure gradient from 35±13 mmHg immediately after balloon valvuloplasty to 28±11 mmHg (p<0.001) during follow-up (Fig 4). Patients with persistent restrictive right ventricular physiology had a higher tricuspid inflow A-wave velocity than controls (A-wave velocity was 0.9±0.27 versus 0.5±0.11 m/s, p<0.001) (Fig 5a) and lower E/A than controls (E/A ratio 0.8±0.35 versus 1.4±0.19, p<0.001).

Figure 4 Demonstrates the reduction of transvalvular pressure gradient during follow-up. ( a ) Right ventricle to pulmonary artery pressure gradient immediately after balloon pulmonary valvuloplasty. ( b ) Transvalvular Doppler measured pressure gradient during follow-up.

Figure 5 Comparison of conventional and tissue Doppler echo findings between patients with persistent restrictive right ventricular physiology and controls.
Patients also had lower tricuspid annular systolic velocity (Sa) of 10±2 versus 16±2 cm/s for controls (p<0.000) (Fig 5d), lower Ea velocity of 10±2.7 compared with controls (16±1.4 cm/s) with significant p<0.001 (Fig 5c), and a higher E/Ea ratio of 7.4±2.2 versus 4.3±0.6 for controls (p<0.0001) (Fig 5b).
Cardiac MRI
Table 5 summarises the results of MRI (no=21 patients). The mean measured right ventricular ejection fraction % by MRI was 60±18 (mean±SD); 3 out of 21 patients had a measured ejection fraction of 45%. The mean right ventricular mass was 44±30 g/m2, which indicates right ventricular hypertrophy (Fig 6c) according to the published normal value 25±4 g/m2.Reference Pennell 23 Late gadolinium enhancement was considered present if there was a bright signal within the myocardium (not blood pool). Out of 21 patients, 13 showed hyper enhancement of the right ventricular myocardium, no sub-endocardial or transmural enhancement. The right ventricular late gadolinium enhancement scores are summarised in Table 6. Examples of late gadolinium enhancement are shown in (Fig 6a1 and a2) and (Fig 6b). The patterns of enhancement in patients with restrictive physiology were localised full thickness enhancement of 1–3 cm in length was visible in the anterior right ventricular out flow tract, anterior right ventricular wall, inferior wall, and right ventricular septal surface; and focal fibroses enhancement was frequently seen at right ventricular insertion points. We found a significant positive correlation between right ventricular late gadolinium scores and the patient’s age (r=0.7, p<0.001) (Fig 7). The right ventricular end diastolic volume ml/m2 measured by cardiac MRI correlated positively with late gadolinium scores (r=0.34, p<0.01) (Fig 8a) as well as the right ventricular mass g/m2 correlated positively with late gadolinium enhancement (r=0.52, p<0.001) (Fig 8b).

Figure 6 Late gadolinium enhancement (arrow) of the right ventricular anterior wall ( a1 and a2 ) and of the inferior wall, superior and inferior insertion point ( b ) in two patients. Increased right ventricular wall thickness ( c ).

Figure 7 Scatter plots showing correlation between late gadolinium enhancement scores and age (r=0.7, p<0.001).

Figure 8 Scatter plots showing positive correlation between late gadolinium enhancement scores (LGE) and the following: ( a ) right ventricular end diastolic volume (RV EDV ml/m2) (r=0.34, p<0.01); ( b ) right ventricular mass (RV mass/m2) (r=0.52, p<0.001) measured by cardiac MRI.
Table 5 Results of cardiac MRI (no=21): RV volume, mass, and function (mean±SD).

RV=right ventricle
Table 6 Late gadolinium enhancement scores in 21 patients with persistent restrictive right ventricular physiology.

RV=right ventricle
Discussion
We treated 44 patients suffering from critical pulmonary valve stenosis with late presentation, cyanosis, restrictive physiology, and right ventricular dysfunction. All were successfully treated and rehabilitated, even those with ascites, pericardial effusion, and impaired liver functions.
There was a significant decrease in right ventricular hypertension and relief of outflow tract obstruction. Moreover, in the present study, there was a significant increase of left ventricular end systolic and end diastolic dimensions during follow-up. This is likely to be the result of increased preload, caused by rise in the right ventricular effective forward flow. Echocardiography showed evidence of marked right ventricular reverse re-modelling, decrease right ventricular size, and the interventricular septum with its resumed normal position. This was accompanied by the improvement in symptoms due to improved loading condition. It has been suggested in previous studies that the increase in left ventricular end diastolic dimension and reduction in the right ventricular end diastolic dimension lead to clinical improvement related to improved diastolic chamber interaction.Reference Atherton, Moore and Lele 24
Data are scanty to address the impact of chronic increase in the right ventricular outflow resistance on right ventricular diastolic performance in patients with isolated pulmonary valve stenosis.Reference Lam, Kaya, Goktekin, Gatzoulis, Li and Henein 19 The fundamental abnormality of restrictive right ventricular physiology is reduced right ventricular compliance as a result of chronic increase in afterload. The right ventricular end diastolic pressure increases and the cavity became unfillable during atrial systole and acts as a passive conduit.Reference Redington, Penny, Rigby and Hayes 4 , Reference Cullen, Shore and Redington 6 Thus, some or all of the transtricuspid atrial systolic flow, as demonstrable by Doppler studies, results in antegrade pulmonary flow.Reference Redington, Penny, Rigby and Hayes 4 , Reference Cullen, Shore and Redington 6
In our study, the haemodynamic data before balloon pulmonary valvuloplasty demonstrated that the right ventricular restrictive pattern was associated with elevation of right ventricular end diastolic pressure, which was significantly higher than the pulmonary artery diastolic pressure; however, it also remained high immediately after balloon pulmonary valvuloplasty.
It seems that the persistence of restrictive physiology in our patients after relief of chronic increase in afterload is a signal suggestive of a sicker right ventricle. Such speculation was evident; during follow-up, when patients with right ventricular restriction were compared with controls, there was a significant reduction of tricuspid annular Ea velocity and higher E/Ea compared with controls. These parameters suggest a stiffer right ventricle. Furthermore, right ventricular systolic dysfunction was suggested by reduced tricuspid Sa systolic velocity (p<0.001). Tissue Doppler imaging velocities have been validated as surrogate markers of right ventricular function.Reference Horton, Meece and Hill 5
Restrictive right ventricular physiology is highly prevalent: 81% in patients with pulmonary atresia and intact interventricular septum, despite achievements of biventricular repair,Reference Liang, Lam, Cheung, Wu, Wong and Cheung 25 exceeding the reported prevalence of restrictive right ventricular physiology in patients at 15–35 years after repair of tetralogy of Fallot (53%).Reference Gatzoulis, Clark, Cullen, Newman and Redington 26 Although the reported incidence of restrictive right ventricular physiology in adults with isolated pulmonary valve stenosis according to Lam et alReference Lam, Kaya, Goktekin, Gatzoulis, Li and Henein 19 was 42%, in this study, such restrictive filling pattern was associated with elevation of right atrial pressure, a shorter tricuspid E-wave deceleration time, and more right ventricular long-axis dysfunction compared with other pulmonary valve stenosis patients and controls. Interestingly, they also demonstrated a trend of progressive fall in long-axis systolic amplitudes as well as Sa and Ea velocities compared with controls and patients without restrictive physiology and those with restrictive right ventricular physiology.Reference Lam, Kaya, Goktekin, Gatzoulis, Li and Henein 19
Late gadolinium enhancement has been regarded as a marker of myocardial fibrosis and scarring,Reference Choudhury, Mahrholdt and Wagner 27 or otherwise abnormal myocardium, an assumption that has been validated histologically in selected cases.Reference Moon, Reed and Sheppard 28 The finding of right ventricular late gadolinium enhancement in patients with pulmonary valve atresia with intact ventricular septum 15 years after complete repair and its inverse relationship with indices of right ventricular end diastolic function support the contention that persistent myocardial abnormalities due to fibrosis or scarring contribute to persistent right ventricular diastolic dysfunction.Reference Liang, Lam, Cheung, Wu, Wong and Cheung 25
Cardiac MRI with late gadolinium enhancement technique further demonstrated that right ventricular restriction in repaired tetralogy of Fallot patients was related to more right ventricular myocardial fibrosis and worse clinical outcome.Reference Babu-Narayan, Kilner and Li 21 Earlier studies reported a higher prevalence of right ventricular restriction in tetralogy of Fallot patients who received transannular patch repair, because of its greater association with more right ventricular scarring than transatrial repair.Reference Munkhammar, Cullen and Jogi 29 Cardiac magnetic resonance with late gadolinium enhancement technique demonstrated that right ventricular restriction in repaired tetralogy of Fallot patients was related to more right ventricular fibrosis and a worse clinical outcome.Reference Redington, Penny, Rigby and Hayes 4 , Reference Cullen, Shore and Redington 6 A mechanism for progressive fibrosis is ventricular hypertrophy and dilation resulting from severe pulmonary valve stenosis, which leads to stretching and right ventricular re-modelling.Reference Moon, Reed and Sheppard 28 In addition, late gadolinium enhancement suggestive of fibrosis has been demonstrated in systemic right ventricle.Reference Babu-Narayan, Goktekin and Moon 8 Recent histological studies reported a higher collagen load in left ventricular myocardium in aortic stenosis patients with severe diastolic dysfunction.Reference Norgard, Gatzoulis and Moraes 30 If we allow the same pathological interpretation to be applied in our patients with severe pulmonary valve stenosis and restrictive physiology, then perhaps right ventricular fibrosis can explain the diastolic restrictive physiology.
Our study demonstrated right ventricular late gadolinium enhancement in 13 out of 21 patients with restrictive physiology, which is suggestive of fibrosis. It seems that patients with right ventricular restriction are more likely to have more collagen deposition in the right ventricular myocardium, which subsequently contributes to right ventricular stiffens. It would be interesting to compare late gadolinium enhancement findings, after balloon valvuloplasty, in patients who have restrictive physiology with those with non-restrictive physiology. This needs further evidence. Delayed enhancement MRI of our patients with restrictive physiology revealed the presence of varying degrees of myocardial fibroses, which ranged from mild patchy areas of enhancement seen at the insertion points to full enhancement of the anterior right ventricular free wall. The study showed that the mean right ventricular ejection fraction measured by cardiac MRI (n=21 patients) was 60±18 (mean±SD); three patients had measured ejection fraction of 45%. Further validation of left ventricular end diastolic volume is required in patients with restrictive physiology with systematic evaluation of the left ventricular systolic and diastolic functions. We found a positive correlation between late gadolinium enhancement scores and right ventricular mass index. This increase in myocardial mass may result in demand–supply mismatch, and when a certain threshold of the right ventricular mass is reached fibrosis ensues. Further studies are needed to exclude coronary artery abnormalities. Standard exercise testing remains an important study in the follow-up of our patients to validate patients’ symptoms and the degree of fibrosis, which may further support our findings. The increase of late gadolinium enhancement with age in our patients may suggest progressive fibrosis. The recent findings may shed light on the mechanism of myocardial damage in longstanding pressure overloaded right ventricle.
Study implication
We suggest assessment of patients with pulmonary valve stenosis and restrictive right ventricular physiology by cardiac MRI with late gadolinium enhancement. The detection of right ventricular fibrosis and measurement of the right ventricular mass by cardiac MRI technique may support new therapeutic approaches that target fibrosis and right ventricular hypertrophy. Further studies need to examine whether drug therapy can prevent or reverse some of the hypertrophic and fibrotic changes reported here. Regular follow-up of patients with pulmonary valve stenosis with right ventricular dysfunction, using right ventricular Doppler echocardiographic measurement to predict the potential reversibility of right ventricular dysfunction must be carried out. Myocardial tissue Doppler imaging and speckle tracking techniques may provide regional quantitative assessment of right ventricular dysfunction. Strain and strain rate are echocardiographic technologies that quantify myocardial deformation. These technologies are relatively load-independent and can provide both regional and global assessment of right ventricular function.Reference Mertens and Friedberg 31 It would be interesting to study the effect of right ventricular fibrosis on myocardial diastolic deformation by speckle tracking technique.
Study limitation
The study included patients with late presentation of critical pulmonary valve stenosis. Not all patients underwent the same tests as some patients with right-sided heart failure came from southern Egypt and remote areas and had difficulty to follow-up regularly. Furthermore, coronary angiography was not available. In addition, we had to study the incidence of restrictive physiology in congenital pulmonary valve stenosis and compare patients who had restrictive physiology with those with non-restrictive physiology. Finally, we did not carry out objective exercise tolerance test for patients to validate patients’ symptoms and the degree of fibrosis, which may have further supported our findings.
Conclusion
In summary, these data describe a unique population with severe pulmonary stenosis, restrictive right ventricular physiology with significantly enlarged right ventricle who underwent balloon pulmonary valvuloplasty. The right ventricular chamber dimension decreased and patients with ascitis were successfully rehabilitated. Persistent right ventricular restrictive pattern after relief of chronic increase of right ventricular pressure suggests that factors other than increase in afterload itself were involved in the physiology; however, it is most likely due to fibrosis as documented by late gadolinium enhancement.
Acknowledgements
The authors are grateful for the support received from the staff at the National Heart Institute and Alfa Scan. They also extend a special thanks to Dr Sara Moharam from the National Heart Institute for her help reviewing the data of cardiac MRI. The authors are also grateful to Ayman Khalifa Biomedical Engineering from Diagnosoft for reviewing the calculation of cardiac MRI.
Financial Support
This work was supported partially by The National Heart Institute and Alfa Scan Radiology Center (for MRI study).
Conflicts of Interest
None.
Ethical Standards
The Ethics Committee of the National Heart Institute approved the study. A written informed consent was obtained from all the patients or their parents.
Supplementary Material
To view supplementary material for this article, please visit http://dx.doi.org/10.1017/S1047951115000724