


In utero displacement of the septum primum with absence of septum secundum can cause the normally located pulmonary veins to drain anomalously into the right atrium.Reference Neill1, Reference Van Praagh, Carrera, Sanders, Mayer and Van Praagh2 This displacement is most commonly found in heterotaxy syndrome of the polysplenia type and hypoplastic left heart syndrome.Reference Neill1, Reference Chin, Weinberg and Barber3 Diagnosis of this condition is straightforward if proper attention is paid to the relationship of pulmonary venous drainage to the position of the atrial septum, and surgical repair has excellent success rates.Reference Hiramatsu, Takanashi and Imai4, Reference Kouchoukos, Blackstone, Hanley and Kirklin5
Isolated severe displacement of the septum primum in patients with situs solitus has been described in recent literature.Reference Cuttone, Hadeed and Lacour-Gayet6 We present a previously undescribed case of septum primum malposition leading to anomalous pulmonary venous drainage and interatrial communication in a child with dextrocardia and situs inversus totalis.
Case summary
A 5-year-old asymptomatic male presented for an evaluation of a murmur that was noted at his recent well-child visit. His cardiac examination was significant for a point of maximal impulse in the right chest, widely split fixed S2, and a grade 2/6 systolic ejection murmur noted at the right upper sternal border. He had no crackles, hepatomegaly, or peripheral oedema. His electrocardiogram performed on the right chest showed normal sinus rhythm with an incomplete right bundle branch block.
Transthoracic echocardiogram revealed dextrocardia with abdominal and atrial situs inversus. The ventricles were L-looped, and the atrioventricular and ventriculoarterial connections were concordant. The right atrium and right ventricle were moderately dilated (Fig 1a). Bilateral superior vena caval veins were visualised with a small bridging vein. The right-sided vena caval vein drained into a dilated roofed coronary sinus (Fig 1b). There was normal atrioventricular valve morphology and function. The septum primum appeared to be deviated towards the left atrium (Supplementary Fig 1) causing a large anterosuperior atrial septal defect. Superior limbic band of septum secundum was not seen. The right-sided pulmonary veins drained normally into the right-sided morphological left atrium, while the left-sided veins drained into the left-sided morphological right atrium (Fig 1c and d). A cardiac CT scan was performed to further delineate this anatomy, which confirmed our findings (Fig 2a and b). At the time of surgery, part of the atrial septum was resected and pericardial patch reconstruction of the atrial septum was done such that the systemic and pulmonary venous connections were separated and were draining to morphological right and left atrium, respectively. The patient had an uneventful postoperative course with no residual defects.
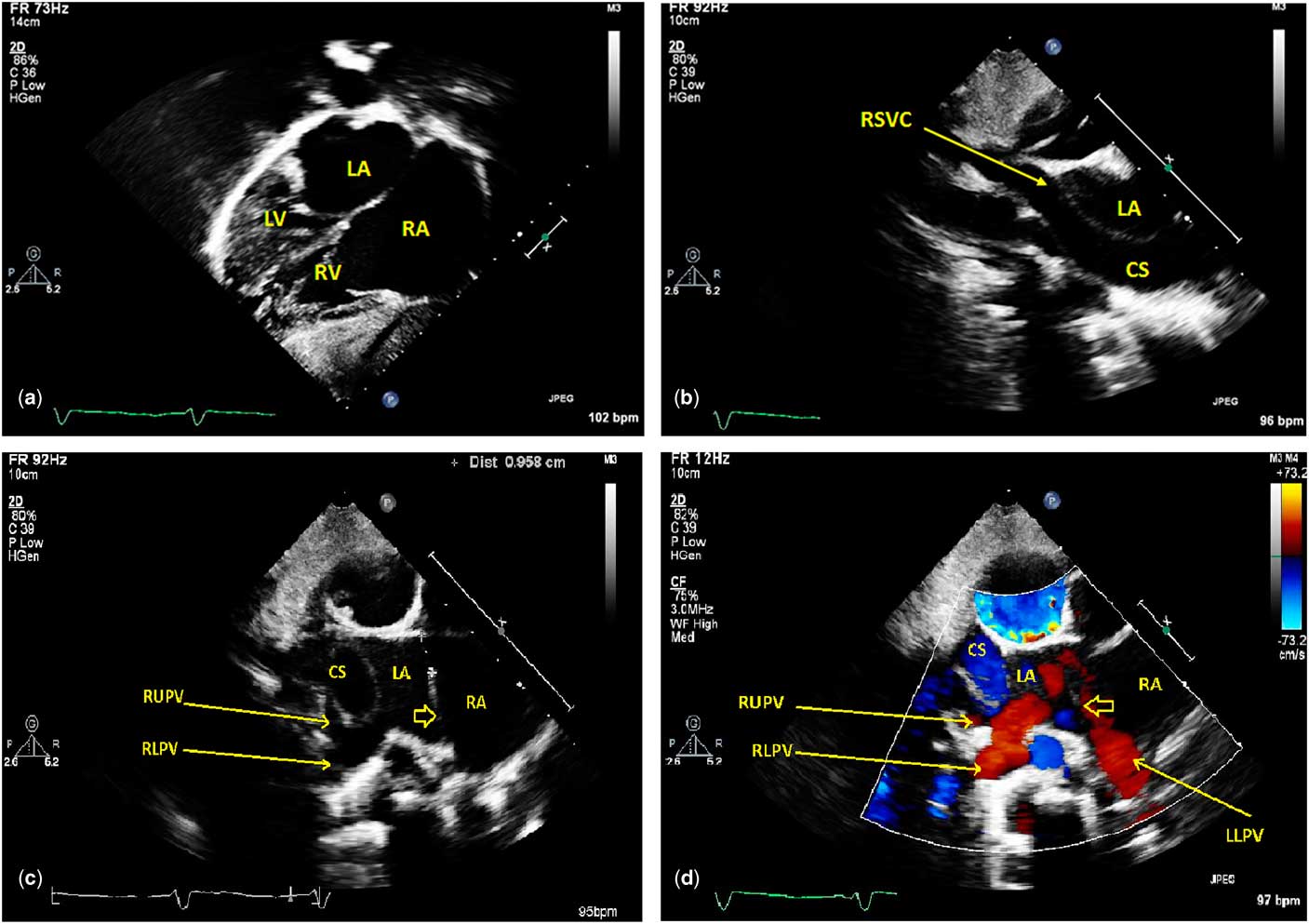
Figure 1 Preoperative transthoracic echocardiographic findings Subcostal long view (a) demonstrating dextrocardia, atrial situs inversus, and L-looped ventricles with mild right-sided enlargement. Modified right parasternal view (b) demonstrating RSVC (arrow) draining into the dilated CS behind the LA. Modified crab view without color Doppler (c) and with color Doppler (d). These images demonstrate the unusual position of the atrial septum (thick arrow), which normally is not seen from a crab view. In a normal patient, the crab view is a coronal view that typically lies completely posterior to the plane of the atrial septum. The LLPV is seen draining into the morphological RA, whereas the RUPV and RLPV drain normally into the left atrium. CS = coronary sinus; IAC = interatrial communication; LA = morphologic left atrium; LLPV = left lower pulmonary vein; LUPV = left upper pulmonary vein; LV = left ventricle; RA = morphologic right atrium; RLPV = right lower pulmonary vein; RSVC = right-sided superior vena caval vein; RUPV = right upper pulmonary vein; RV = right ventricle.

Figure 2 CT scan axial views demonstrating pulmonary venous drainage (a) Left lower pulmonary vein drains anomalously to the morphologic right atrium due to the malposed atrium septum, whereas the right lower pulmonary vein drains normally into the morphologic left atrium. A hypothetical plane of the septum (dotted line) had it been truly a mirror image of normal as would be expected in situs inversus totalis, which would have incorporated all the pulmonary veins in the morphologic left atrium. (b) Left upper pulmonary vein drains into the morphological right atrium, whereas the right upper pulmonary vein drains into the morphologic left atrium. Anterior and superior interatrial communication is seen. CS = coronary sinus; LA = morphologic left atrium; LLPV = left lower pulmonary vein; LUPV = left upper pulmonary vein; RA = morphologic right atrium; RLPV = right lower pulmonary vein; RSVC = right-sided superior vena caval vein; RUPV = right upper pulmonary vein; IAC = interatrial communication.
Discussion
Through multi-modality imaging, we report a rare case of atrial septal malposition in a patient with dextrocardia and situs inversus without heterotaxy syndrome. Embryologically, septum primum grows to the leftward aspect of the sinus venosus, thus appropriately dividing the primitive atrium such that the systemic veins drain into the right atrium. The common pulmonary vein then grows to become incorporated in the back wall of the left atrium, leftward to the septum primum. Normal growth of the septum primum is essential to ensure alignment of the pulmonary veins to the respective atria.Reference Neill1 Edwards and Moller first observed that displacement of this septum primum can cause an interatrial communication as well as false incorporation of the pulmonary veins to the morphological right atrium.Reference Moller, Nakib, Anderson and Edwards7 Based on the degree of malposition, half or all of the pulmonary veins drain anomalously into the right atrium. In 1995, van Praagh et al proposed the term “septum primum malposition” defect for this conglomeration of findings.Reference Van Praagh, Carrera, Sanders, Mayer and Van Praagh2
Malposition of the septum causing anomalous pulmonary venous drainage has been most commonly associated in patients with visceral heterotaxy, with a preponderance towards polysplenia type.Reference Silvestri, Scarabotti and Marino8 Absence of the superior limbic band of septum secundum (~95%) in these patients was hypothesised to cause malposition of the septum primum.Reference Moller, Nakib, Anderson and Edwards7, Reference Park, Fedderly and Frommelt9 In the series by van Praagh et al, all but three of 36 cases with septum primum malposition defects had confirmed heterotaxy syndrome.Reference Van Praagh, Carrera, Sanders, Mayer and Van Praagh2 A recent study of patients with hypoplastic left heart syndrome showed that 64% of patients had leftward displacement of the septum primum.Reference Tomar, Radhakrishnan and Shrivastava10 Their paper theorised that decreased in utero flow to the left atrium from the malposed septum could cause small left-sided structures. Although isolated deviation of the septum primum without other intracardiac defects has been reported in situs solitus,Reference Van Praagh, Carrera, Sanders, Mayer and Van Praagh2, Reference Tomar, Radhakrishnan and Shrivastava10 our patient was a unique presentation of isolated septum primum displacement in situs inversus totalis.
Echocardiography is typically sufficient for diagnosis of this condition, although CT or MRI can enhance visualisation. Normally, in both situs solitus and situs inversus, the atrial septum runs obliquely such that on axial views the left atrium appears as a midline chamber in front of the trachea. However, for our patient, the septum was positioned more sagittally than normal, and the morphologic left atrium was, therefore, not a midline chamber. The pathognomic finding is deviation in the plane of the atrial septum seen with normal connections but abnormal drainage of the pulmonary veins. It is important to distinguish this defect from sinus venosus defect of the right atrial type as well as large secundum defects that extend posteriorly, allowing the right-sided pulmonary veins to drain anomalously into the right atrium despite their normal connection with the left atrium.Reference Kouchoukos, Blackstone, Hanley and Kirklin5
Repair in this defect is uncomplicated with good results. The typical operation consists of complete resection of the septum primum and replacement of the excised tissue with a pericardial patch.Reference Van Praagh, Carrera, Sanders, Mayer and Van Praagh2 Complete resection has been recommended to avoid pulmonary venous obstruction which can occur as a late complication.Reference Hiramatsu, Takanashi and Imai4 Atrial septal displacement technique without using pericardial patch has also been described with a proposed benefit of avoiding patch retraction and allowing natural septal growth.Reference Van Praagh, Carrera, Sanders, Mayer and Van Praagh2 Our patient underwent a successful repair with partial excision of the septum and placement with a pericardial patch.
In conclusion, it is important to maintain a high index of suspicion for a septum primum malposition defect in patients with anomalous pulmonary venous drainage. To our knowledge, we report the first case of a septum primum malposition defect in a patient with dextrocardia and situs inversus totalis without visceral heterotaxy syndrome.
Supplementary materials
To view supplementary material for this article, please visit https://doi.org/10.1017/S1047951118002263
Acknowledgements
None.
Financial Support
This research received no specific grant from any funding agency, or from commercial or not-for-profit sectors.
Conflicts of Interest
None.




