Introduction
Congenital cardiac tumours are rare with an estimated prevalence of 0.14% during fetal life.Reference Uzun, Wilson, Vujanic, Parsons and De Giovanni 1 Among them, the cardiac teratomas are usually benign masses and reveal as multi-cystic lesions with derivatives of all three germ layers – endoderm, mesoderm, and ectoderm. Most of the cases involves the pericardium and the anterior mediastinum and can cause severe fetal pericardial effusion requiring drainage during the pregnancy. Very rarely, they can be located inside the cardiac cavities and be responsible for one or more classic symptoms seen in case of heart tumours considering their size and location, such as outflow obstruction, systemic or pulmonary embolisation, and arrhythmias. Unlike rhabdomyomas, regression potential of the teratomas is low and perinatal growth can be rapid.Reference Campagne, Quereda and Merino 2
We report here the uncommon neonatal rhythmic presentation of an intracardiac teratoma involving the right ventricle and requiring rescue extracorporeal support (ECMO) before surgical resection.
Case report
A fetus was referred at 23 gestational weeks for a circumscribed heart mass located inside the right ventricle. The previous routine scans were normal. According to the sonographic characteristics of the tumour, the diagnosis of intracardiac teratoma was already suggested (Supplementary Video S1). As there was no haemodynamic issue and no extracardiac anomalies, the parents decided to pursue the pregnancy. At 36+5 gestational weeks, the repeated ultrasound examination confirmed the cystic heterogeneous structure of the tumour measuring 25×35 mm and filling almost all the right ventricular cavity, but without altering the fetal cardiac physiology. Over pregnancy, fetal wellbeing scores remained good and cardiac rhythm was sinus.
A male infant weighing 2800 g was finally delivered at term by caesarean section after a brief episode of tachycardia during labour. He was admitted to our cardiac department to monitor haemodynamic during the transition period. Transthoracic echocardiography confirmed the prenatal findings and suggested a well-limited heterogeneous lesion inside the right ventricle with a moderate left-outflow obstruction caused by the ventricular septum subaortic bulging. The cardiac function was preserved. The multi-cystic mass measured 18×30 mm and was adherent to the entire right interventricular septum. Cardiac CT was consistent with the previous imaging and revealed a large nonvascularised mass measuring 35×25×25 mm and occupying almost all the right ventricular cavity causing a significant obstruction of the pulmonary infundibulum and a deviation of the epicardial course of the coronary arteries without compression. At day 3, a sustained ventricular arrhythmia was responsible for the low cardiac output. Despite multiple electric shocks and high-dose antiarrhythmic medical treatment, including intravenous amiodarone and lidocaine, the haemodynamic situation remains compromised with intractable recurrent ventricular tachycardia. An ECMO was started and it was decided to attempt to resect part of tumour to improve the haemodynamic and potentially to suppress the substrate of the ventricular tachycardia.
An incomplete surgical resection of the tumour was performed by direct opening of the right ventricle. As expected, the tumour protruded into the right ventricle and invaded the tricuspid valve reducing its diameter. Careful lesion excision required cardiac arrest for 54 minutes.
The post-operative course was complicated by persisting low cardiac output requiring continuation of ECMO. Immediately after the intervention, the transthoracic echocardiography showed severe systolic dysfunction of both ventricles, but no inflow or outflow obstruction. There were no recurrent arrhythmias. Unfortunately, serious bleeding on ECMO and infectious issues finally led to death on day 9.
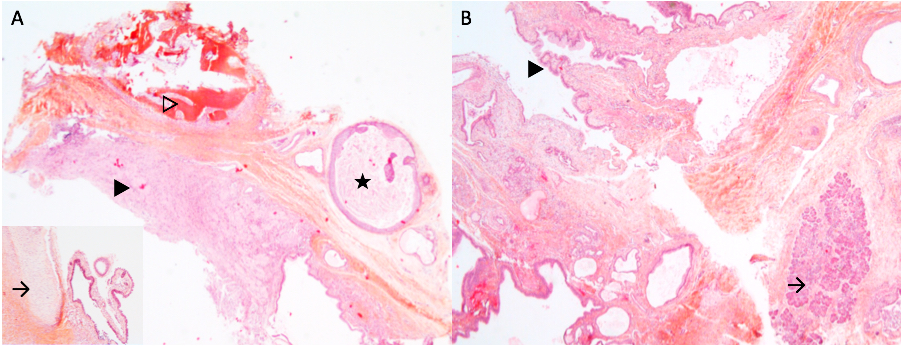
The post-mortem pathologic examination revealed a large heterogeneous multi-cystic and haemorrhagic tumour developing from the all length of the interventricular septum except the apical portion and spreading into the right ventricle cavity (Fig 1). The left ventricle was deemed clogged by both the interventricular septum deformation caused by the tumour and an unusual large Moulaert muscle. Histopathologic examination of the tumour confirmed the diagnosis of mature cystic cardiac teratoma without immature or malignant elements. It included organised structures derived from all three embryonic layers (Supplemental Figure S2).

Figure 1 Macroscopical examination reveals RV expensive tumour spreading into the outflow tract ( a ) and the tricuspid valve (arrow, b ). The interventricular septum is occupied by cysts and haemorrhagic areas (arrows, c ). The detailed examination ( d ) reveals fragments of mature cartilage (1), cystic structures (2), and hairy components (3). LV=left ventricle; PA=pulmonary artery; RV=right ventricle.
Discussion
To date, only a few cases of true intracardiac teratomas have been reported, with the majority found during autopsy or during surgery when performed later during childhood.Reference Campagne, Quereda and Merino 2 – Reference Ou, Dorrière, Sidi, Bonnet and Vouhé 4 These tumours are usually appended to the interventricular septum and grow into the right ventricle. Symptomatic patients are at high risk of sudden death and might require urgent surgery.Reference Campagne, Quereda and Merino 2 , Reference Stiller, Hetzer and Meyer 5 The most common presenting symptoms are cyanosis, isolated murmur, and less frequently heart failure. Our case presented with unusual refractory ventricular tachycardia requiring rescue extracorporeal support. So far, the only curative available treatment for cardiac teratoma is the surgical excision that must be very thorough.
Nowadays, tumours can be diagnosed in utero allowing an organised fetal and neonatal management.Reference Campagne, Quereda and Merino 2 , Reference Gembicki, Hartge, Hoffmann, Krapp, Vokuhl and Weichert 3 We report here the third prenatally diagnosed intracardiac teratoma. Although the published cases had a favourable outcome in older children,Reference Stiller, Hetzer and Meyer 5 attempting a resection of the tumour in a neonate is highly challenging. In our case, even if the ventricular arrhythmia could be controlled after surgery, the complete resection of the tumour was not possible and the ventricular function was severely altered after the bypass. Neonatal symptomatic intramyocardial teratomas are exceedingly rare but despite their benign histology, prognosis appears finally poor when surgery is performed early in life. Almost all the perinatal cases in the literature died when requiring an urgent operation in the first days of life even if the pregnancy was uneventful (Table 1). Imaging by ultrasounds and CT, before and after birth, fails to predict the neonatal outcome. Moreover, whatever the perinatal presenting features and management, the outcome is unfavourable and likely related with the inevitable and quick growth of the tumour. The most recent cases including ours suffered right ventricular diastolic dysfunction after surgery and required extracorporeal haemodynamic support. Despite this aggressive post-operative management, heart failure and various multi-organs complications led them to death. The only two reported infants who survived after the surgical resection were haemodynamically asymptomatic before the operation and presented solely with a murmur or a cyanosis.
Table 1 Features of perinatal benign intracardiac teratomas. Tumours found at autopsy are not included.

AVV=atrioventricular valves; ECMO=extracorporeal membrane oxygenation; IAS=interatrial septum; IVS=interventricular septum; LV=left ventricle; OFT=outflow tract; RA=right atrium; RV=right ventricle; TV=tricuspid valve; WG=week of gestation.
In conclusion, intracardiac teratomas demonstrate severe prognosis when displaying during the perinatal course. Even in the absence of apparent complications during pregnancy, the lack of identified predictors of outcome should lead to caution when counselling parents prenatally.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/S1047951118002354
Acknowledgements
The authors greatly acknowledge Dr V.V. and Dr C.P. for their precious help in histology imaging and comments.
Financial support
This research received no specific grant from any funding agency, or from commercial or not-for-profit sectors.
Conflicts of interest
None.