


Case report
A 21-year-old woman underwent the fourth median sternotomy for the progression of the pulmonary stenosis and regurgitation, aortic regurgitation. Her initial diagnosis was truncus arteriosus; the previous operations included a conduit replacement from the right ventricle to the pulmonary artery and ventricular septal defect closure at 11 days of age, left pulmonary arterial angioplasty at 3 years of age, and bilateral pulmonary arterial angioplasty at 7 years of age. During the third operation, the right pulmonary artery was dual supplied with a placement of a 14-mm expanded polytetrafluoroethylene graft anteriorly to the ascending aorta from the main pulmonary artery to the distal right pulmonary artery for a supplemental flow of the right pulmonary artery to the narrowed native right pulmonary artery. Despite no apparent symptom, her aortic and pulmonary regurgitation were progressed significantly; a surgical intervention was indicated.
A preoperative cardiac catheterisation revealed pulmonary to systemic flow ratio of 1.47, main pulmonary arterial pressure of 44/12/25 mmHg, and right and left ventricular end-diastolic volume index of 150 and 139% of normal.
The graft from the main pulmonary artery to the right pulmonary artery was sandwiched between the sternum and the aorta, and a part of the graft was calcified and embedded to the retro-sternum.
A cardiopulmonary bypass through the femoral artery and vein was commenced before the redo sternotomy; this graft was excised carefully from the surrounding tissues to approach the ascending aorta. While dissecting further, the right pulmonary veins entering to the right atrium were found unexpectedly. During a cardiac arrest, the ascending aorta was incised, and the incompetent truncal valve, which had four cusps, was replaced with a 23-mm bioprosthetic valve (Edwards Lifesciences, Irvine, California, United States of America). The atrial septal defect was created, and the anomalous pulmonary veins were rerouted to the left atrium through the atrial septal defect by using an expanded polytetrafluoroethylene baffle, and the superior caval vein to the right atrium was supplemented with another expanded polytetrafluoroethylene patch. For the right ventricle to pulmonary artery, the highly calcified pulmonary valve was removed, and a 25 mm Crown valve (Sorin Group, Saluggia, Italy) was sewn and the anterior aspect of the main pulmonary artery was enlarged with another expanded polytetrafluoroethylene patch. Finally, an alternative 14-mm expanded polytetrafluoroethylene graft was placed as it was anterior to the ascending aorta. A thin sheet of expanded polytetrafluoroethylene was placed in the retro-sternal space. No adverse event was observed postoperatively.
Discussion
There are several issues for this case. First, the partial anomalous venous drainage was diagnosed at the fourth operation. This was because the dilated right atrium and ventricle owing to severe pulmonary regurgitation masked partial anomalous pulmonary venous drainage. However, considering the pulmonary to systemic flow ratio of 1.47 and high pulmonary arterial pressure, we should have investigated the reason for this unexplainable number preoperatively. Second, we found that the expanded polytetrafluoroethylene is not always calcification-free after the implantation. There are several reports regarding the calcification after implantation of the expanded polytetrafluoroethylene graft.Reference Hayabuchi, Mori, Kitagawa, Sakata and Kagami 1 Hayabuchi et al reported the incidence of calcification of the implanted expanded polytetrafluoroethylene. In total, 17% (5/29) of the cases for ventricular septal defect patch and 81% (26/32) for right ventricular outflow tract prosthesis showed calcification in their retrospective study. In the present case, the calcified expanded polytetrafluoroethylene was embedded into the retro-sternum (Fig 1). Although this is a very rare case, attention is necessary at the time of redo sternotomy when the expanded polytetrafluoroethylene graft or prosthesis is attached to the sternum. Third, as this is a case of adult CHD, these patients often encompass multiple lesions, some of which are related to the underlying CHD and others are newly developed or undiagnosed lesions. The initial diagnosis of this patient was truncus arteriosus; her aortic and pulmonary valves were susceptible to be impaired as the patient grew. The partial anomalous pulmonary venous drainage also contributed to dilatation of the right atrium and right ventricle resulting in cardiac failure.Reference Sormani, Roghi and Cereda 2 Therefore, a multidisciplinary preoperative investigation is vital for making a surgical strategy. Furthermore, for these patients with adult CHD, it is most important to address all these complicating factors as much as possible at the redo surgeryReference Sughimoto, Matsuo and Niwa 3 (Fig 2).
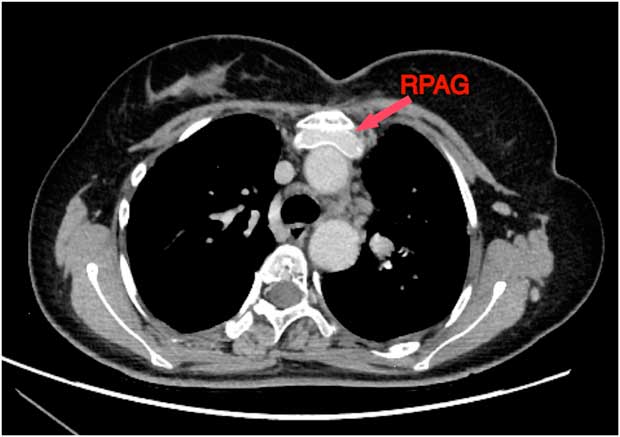
Figure 1 Highly calcified expanded polytetrafluoroethylene graft embedded into the retro-sternum. RPAG=graft of the right pulmonary artery.

Figure 2 Undiagnosed partial anomalous pulmonary venous drainage into the superior caval vein. PAPVD=partial anomalous pulmonary venous drainage; SCV=superior caval vein.
Acknowledgements
None.
Financial Support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Conflicts of Interest
None.


