Cardiac involvement is a recognised complication of systemic lupus erythematosus seen in 30% cases and involves most cardiac components including pericardium, conduction system, myocardium, heart valves, and coronaries.Reference Moder, Miller and Tazelaar 1 The Libman–Sacks endocarditis is characterised by sterile fibrinous vegetations affecting mainly mitral and aortic valves and is reported in 11% cases of systemic lupus erythematosus in adults.Reference Moyssakis, Tektonidou, Vasilliou, Samarkos, Votteas and Moutsopoulos 2 A handful of case reports of Libman–Sacks endocarditis are reported in children.Reference Durand, Blaysat, Chauvaud, Tron and Kachner 3 – Reference Kriebel, Sasse, Fink, Paul, Holtvogt and Hausdorf 5 The association of systemic lupus erythematosus with antiphospholipid antibodies was first reported in 1985 in a young woman with systemic lupus erythematosus and lupus anticoagulant.Reference D'Alton, Preston, Bormanis, Green and Kraag 6 The prevalence of valvular abnormalities is much higher when systemic lupus erythematosus is accompanied by antiphospholipid antibodies. Libman–Sacks endocarditis is usually mild and asymptomatic in a majority of the cases and complications include superimposed bacterial endocarditis, thromboembolic events, and severe valvular dysfunction requiring surgery.
Case report
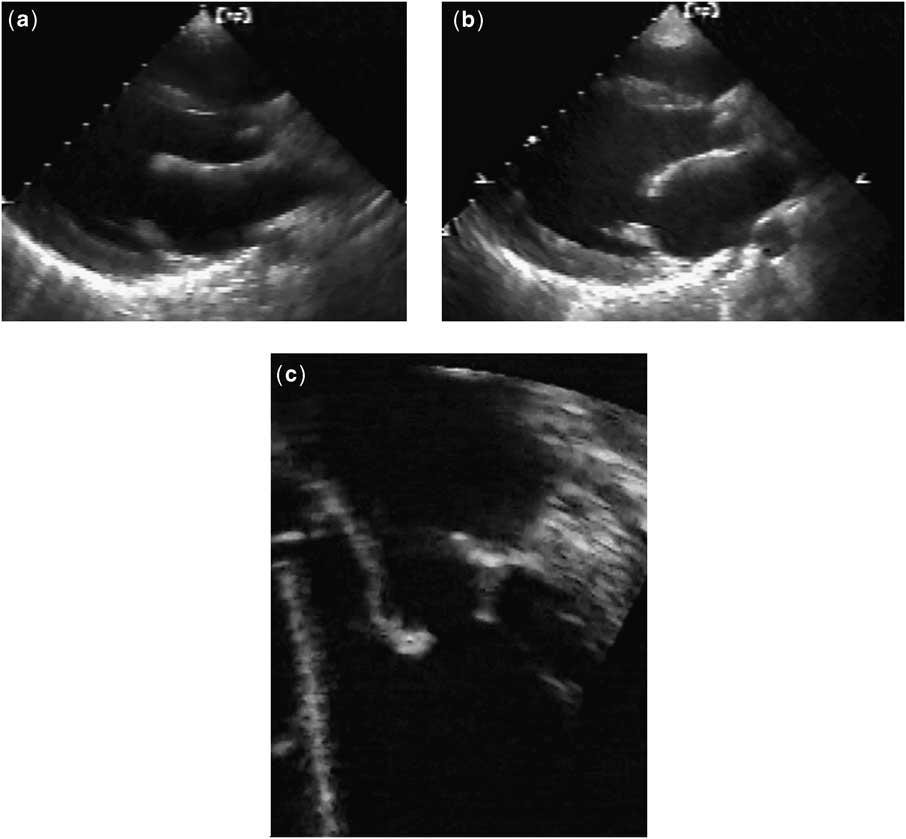
A 14-year-old girl with recent onset of worsening exercise tolerance was referred for cardiac surgery owing to chronic mitral regurgitation and progressive dilatation of left ventricle with preserved systolic function. Her pre-operative two-dimensional echo-Doppler study showed thickened and nodular-looking mitral leaflets with obvious incomplete closure giving rise to severe mitral regurgitation (Fig 1, Video clip-1). The subvalvar apparatus of mitral valve and proximal coronaries were normal. She had been diagnosed with isolated mitral regurgitation in early childhood, with a thick and myxomatous-looking mitral valve. Her mitral regurgitation deteriorated from mild to severe degree in the next decade with worsening valve pathology, as demonstrated by serial echocardiographic illustrations at age 4, 7, and 10 years (Fig 2). There was no history of persistent fever of unknown origin, joint pain, skin rash, or asymptomatic proteinuria during that period. Family history was also negative for connective tissue disorders. She underwent mitral valve repair in the form of wedge resection of anterior mitral leaflet, commissuroplasty, and posterior annuloplasty ring, and was placed on anticoagulation for 3 months.

Figure 1 Thickened and nodular mitral leaflets with incomplete closure.

Figure 2 ( a , b , c ): Transition of thick and myxomatous-looking mitral valve to a thick and nodular one at age 4,7, and 10 years, respectively.
She developed persistent fever 2 months after cardiac surgery without obvious focus. In view of the recent valve repair, she underwent work-up for endocarditis including blood counts, sedimentation rate, multiple blood cultures, and repeat echocardiogram. Her total white cell count was 10.8 thousands without leftward shift, with a sedimentation rate of 85 millimetres/first hour and negative blood cultures. Her transthoracic echocardiogram showed a good mitral valve repair but was inconclusive for vegetations owing to multiple artifacts caused by the annuloplasty ring, and the transoesophageal study was negative for vegetations or clot. Her international normalised ratio was 3.5 despite low-dose warfarin and continued to be abnormally elevated even after discontinuation of warfarin. She had persistent bouts of fever in the face of intravenous antibiotic therapy for presumptive endocarditis and ultimately underwent a work-up to rule out a connective tissue disorder. On further analysis, she had positive antinuclear antibodies with a titre more than 1:160, positive double-stranded deoxyribonucleic acid, and total haemolytic complement level of less than 6 units/millilitre. Her anticardiolipin antibody titre was 48 international units/millilitre with positive lupus anticoagulant, which remained abnormal several weeks later at follow-up. The histopathology of her mitral valve was reviewed in the light of this new diagnosis of systemic lupus erythematosus with antiphospholipid antibodies and demonstrated typical findings of Libman–Sacks endocarditis (Fig 3). She subsequently developed proteinuria and underwent renal biopsy, which confirmed the diagnosis of lupus nephritis.
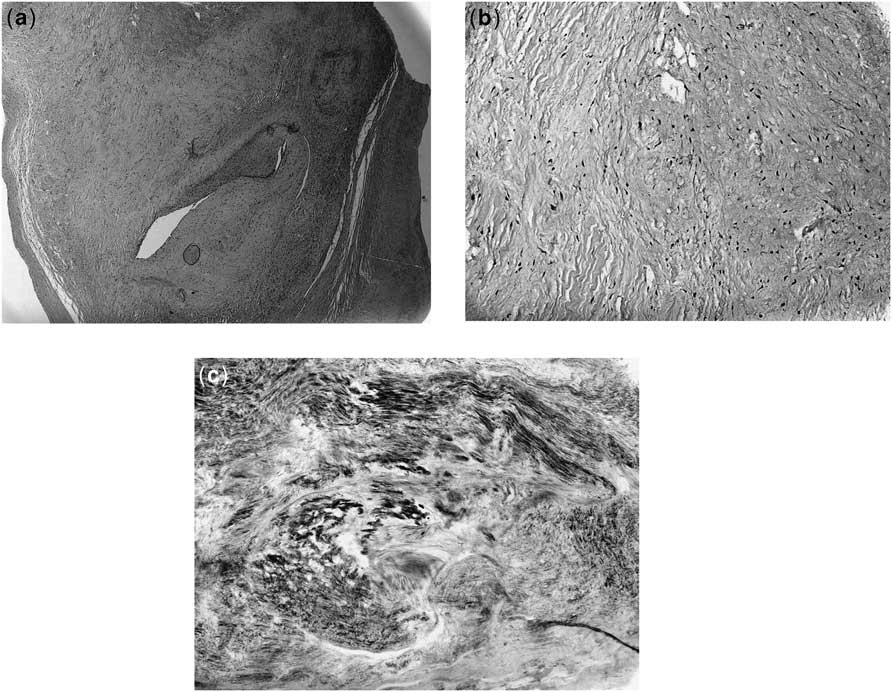
Figure 3 ( a , b , c ): Haematoxylin and eosin stain and Giemsa stain showing areas of dense vascularised fibrous tissue with myxoid changes.
She was placed on steroids with intermittent immunosuppressive therapy. She has been doing reasonably well with mild residual mitral regurgitation and thickened mitral leaflets at the 10-year follow-up (Video clip-2).
Discussion
Systemic lupus erythematosus is rare in infancy and early childhood. Libman–Sacks endocarditis was originally described in 1924 in four patients with atypical sterile verrucous lesions of valvular and mural endocardium.Reference Libman and Sacks 7 Such verrucous endocarditis is reported in both systemic lupus erythematosus and antiphospholipid antibody syndrome and they occur 5–9 times more often in women.
The lesions of Libman–Sacks endocarditis, based on post-mortem studies, are described as “mulberry-like” firm clusters of verrucae on the ventricular surface of the mitral valve leaflets, with adherence of leaflet and chordae to the mural endocardium. There is a predilection for the mitral valve in both systemic lupus erythematosus and primary antiphospholipid antibody syndrome, similar to rheumatic heart disease, the most common immune-related valvulopathy, but rarely involves valves of the right heart.Reference Moaref, Afifi, Rezaian and Rezaian 8 The morphology of the valvular lesion of Libman–Sacks endocarditis includes a fibrous vegetation or rigid and thickened valve leaflet prone to haemodynamic deterioration and valvular dysfunction. Both variants represent different stages of the same pathological process. The shift in valve pathology from vegetations to emergence of fibrosed malfunctioning valve is related to steroid therapy and longer survival.Reference Bulkley and Roberts 9 , Reference Galve, Candell-Riera, Pigrau, Soler-soler, Permanyer-Miralda and Garcia-Del-Castillo 10
Macroscopically, Libman–Sacks endocarditis valvular lesions at the time of cardiac surgery are typically wart like and small, varying from pinhead to 3–4 millimetres in size, firmly attached to valve surface, exhibiting no independent motion. Microscopically, they are characterised by fibrin deposits at various stages of fibroblastic organisation, neovascularisation, and variable degree of inflammation with mononuclear cell infiltration. The different stages of Libman–Sacks endocarditis have been described as active, active and healed, and healed lesions. The healed form of Libman–Sacks endocarditis is a fibrous plaque with marked scarring, thickening, and deformity of the valve, leading to valve dysfunction.Reference Bulkley and Roberts 9 , Reference Bouma, Klinkenberg and Erasmus 11
Antiphospholipid antibodies are a family of autoantibodies that recognise various combinations of phospholipids and phospholipid-binding proteins. Antiphospholipid antibody syndrome is defined by the presence of antiphospholipid antibodies, venous or arterial thrombosis, recurrent pregnancy loss, or thrombocytopenia. Antiphospholipid antibody syndrome is considered to be the most common acquired hypercoagulation state of autoimmune disorder in children and is associated with high spontaneous international normalised ratio as antiphospholipid antibodies interfere with coagulation profile, as in this case. Antiphospholipid antibody syndrome is primary in half of the cases and secondary in the remaining, mainly because of systemic lupus erythematosus.Reference Lee, Von scheven and Sandborg 12 Patients with primary antiphospholipid antibody syndrome exhibit valvular abnormalities on echo evaluation in 30% cases, which is considerably higher than in general population (0–4%).Reference Lee, Von scheven and Sandborg 12 , Reference Hojnik, George, Ziporen and Shoenfeld 13 Therefore, valvular heart disease is accepted as an integral part of the antiphospholipid antibody syndrome. A significantly higher level of immunoglobulin G anticardiolipin antibodies in patients with mitral valve nodules supports the notion of a causative relationship between circulating antibodies and such lesions.Reference Farzaneh-Far, Roman and Lockshin 14 Bidani et alReference Bidani, Roberts, Schwartz and Lewis 15 demonstrated granular deposits of immunoglobulins and complement components in endocardial stroma along edges of valve leaflets and in vegetations from patients with systemic lupus erythematosus. The prevalence of mitral valve nodules is three times higher in the antiphospholipid antibody-positive group than in the antiphospholipid antibody-negative group of systemic lupus erythematosus, and more frequently associated with moderate to severe mitral regurgitation.Reference Khamashta, Cervera and Asherson 16 Thus, Libman–Sacks endocarditis is considered an immune-induced valvulopathy and is a cardiac manifestation of both systemic lupus erythematosus and antiphospholipid antibody syndrome.
The use of corticosteroids in the management of systemic lupus erythematosus seems to have decreased the prevalence of Libman–Sacks endocarditis, which is supported by observation of 59% incidence of Libman–Sacks endocarditis in the pre-steroid era on autopsy series as compared with 35% after their use.Reference Doherty and Seigel 17 Corticosteroids actually do not prevent Libman–Sacks endocarditis, but they facilitate healing over time by decreasing the amount of inflammation. However, they can also increase fibrosis and scarring, ultimately worsening valvular damage and dysfunction.
Echocardiography can help identify the lesions of Libman–Sacks endocarditis in the context of systemic lupus erythematosus or antiphospholipid antibody syndrome; however, these findings are non-specific. The definitive diagnosis of Libman–Sacks endocarditis can only be made by histopathological examination of the affected valves. The differential diagnosis of Libman–Sacks endocarditis includes pseudoinfective endocarditis and papillary fibroelastoma of the mitral valve.
A handful of cases of Libman–Sacks endocarditis are reported in the paediatric age group (Table 1).Reference Durand, Blaysat, Chauvaud, Tron and Kachner 3 – Reference Kriebel, Sasse, Fink, Paul, Holtvogt and Hausdorf 5
Table 1 Cases of Libman–Sacks endocarditis in Children.
APS = antiphospholipid antibody syndrome; MR = mitral regurgitation; SLE = systemic lupus erythematosus
Systemic lupus erythematosus is a complex and protean disease, frequently present with subtle manifestations before eventual full-blown clinical disease. The clinical and biological symptoms of systemic lupus erythematosus may be delayed by several years after initial isolated cardiac or renal involvement, as in our case.Reference Gianviti, Barsotti, Barbera, Paraggiana and Rizzoni 18 , Reference Nakahara, Hayashi and Matsui 19
The valvular abnormalities in Libman–Sacks endocarditis are usually clinically silent without significant valve dysfunction. In 1974, Myerowitz et alReference Myerowitz, Michaelis and McIntosh 20 were the first to report a successful surgical management of severe mitral regurgitation through mitral valve replacement in a patient with systemic lupus erythematosus. Heart valve surgery in Libman–Sacks endocarditis with significant valvular dysfunction depends on age, valve pathology, and presence of antiphospholipid antibodies.Reference Bouma, Klinkenberg and Erasmus 11 Thromboembolic complications are common after heart valve surgery in the presence of antiphospholipid antibodies. Children with antiphospholipid antibodies generally do not experience a high rate of thromboembolic events, which is partly related to developmental differences in the levels of coagulation proteins, as well as to the relative health of vascular endothelium compared with that of adults.Reference Myones 21 Therefore, a prophylactic long-term anticoagulation therapy is not justified in children without evidence of recurrent thrombosis. The patient in the present case was also not placed on warfarin for the same reason. Tissue heart valve prosthesis is considered an ideal substitute in patients with antiphospholipid antibody syndrome, minimising the risks of morbidity and mortality due to hypercoagulable state.Reference Colli, Mestres and Espinosa 22 Mitral valve repair with removal of leaflet vegetations and ring annuloplasty is preferred in young patients, as in our case, to avoid long-term anticoagulation and afford for somatic growth.Reference Perier, Jeserich, Vieth, Pohle, Hohenberger and Diegeler 23 There are limited data available in the literature regarding mitral valve repair in children in the context of Libman–Sacks endocarditis, but in adults it gives good results without recurrence of mitral regurgitation in selected cases in the midterm follow-up.Reference Bouma, Klinkenberg and Erasmus 11 When significant valve thickening and extensive tissue destruction occur in Libman–Sacks endocarditis, prosthetic valve replacement remains the only option.
Our case presents several interesting aspects of Libman–Sacks endocarditis and disease process of systemic lupus erythematosus. Systemic lupus erythematosus is rare in infancy and early childhood. Our patient had a cardiac involvement starting in early childhood, for almost a decade, based on serial echocardiographic evidence without clinical findings of lupus before its incidental diagnosis after cardiac surgery. Serial echocardiographic images show transition from a thick and myxomatous appearance of the mitral leaflets to a nodular one with worsening regurgitation. Libman–Sacks endocarditis was the first manifestation of systemic lupus erythematosus in our case. The clinical laboratory data confirming diagnosis of systemic lupus erythematosus and secondary antiphospholipid antibody syndrome appeared several weeks later. The surgical repair in our young patient with resection of valve vegetation and annuloplasty ring gave good results at the 10-year follow-up. In retrospect, the possibility of systemic lupus erythematosus/antiphospholipid antibody syndrome should be considered in cases with isolated valvular regurgitation with abnormal looking thick valve in the paediatric age group.
Supplementary materials
For supplementary materials referred to in this article, please visit http://dx.doi.org/doi:10.1017/S1047951112001023